Introduction: The first two years of a child's life are particularly important. Inadequate breastfeeding practices during this period considerably compromise the health, development and survival of infants, children and mothers. Several studies have assessed the impact of breastfeeding on infant mortality. The objectives of our study were to investigate changes in exclusive breastfeeding practices during the first six months of life according to DHS data from 2010-2011 to 2019 and to identify the various associated factors. Methodology: This is a quantitative analysis of secondary data based on cross-sectional data from the DHS from 2010-2011 to 2019 on changes in exclusive breastfeeding practices for infants under six months of age. Our study focused on women aged 15 to 49 years interviewed during the DHS and residing in Senegal at the time of the various surveys who had children under two years of age. Data were collected on exclusive breastfeeding rates in different years, the socio-demographic and gyneco-obstetric characteristics of mothers, and the characteristics of newborn children. A multivariate analysis was performed to identify factors associated with exclusive breastfeeding. Results: showed that exclusive breastfeeding rates remained below 50% from 2010-11 to 2019. Analysis by region showed a disparity between the different regions. The associated factors were: ethnic group: Wolof are less likely to practice EBF with an adjusted AOR of 0.59 with a CI95: [0.38, 0. 90], maternal literacy: mothers who could not read were less likely to perform EBF with an adjusted AOR of 0.71 and a CI95: [0.53-095], birth order: mothers with 6 or more children were more likely to perform EBF, with an AOR of 3.20 and a CI95: [1.68-6.17], maternal occupation: Working mothers were less likely to practice EBF than non-working mothers, with an AOR of 0.60 and a CI95 [0.46-0.79], access to the media: Mothers with access to the media were less likely to practice assisted fertilization, with an AOR of 0.57 and a CI95: [0.37-0.90] and use of modern contraception: Mothers using modern contraception were less likely to practice exclusive breastfeeding, with an AOR of 0.53 and a CI95: [0.38-0.72]. Conclusion: Despite all the efforts made by the Senegalese government and its technical and financial partners, rates are still low. To strengthen the practice of exclusive breastfeeding, it is important and urgent to design and implement innovative evidence-based interventions covering the different levels of the socio-ecological model (individuals, families, communities and public policies).
| Published in | World Journal of Public Health (Volume 9, Issue 2) |
| DOI | 10.11648/j.wjph.20240902.16 |
| Page(s) | 156-177 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Evolution, Excluse Breastfeeding, Associated Factors, DHS 2010-2019, Senegal
3.1. Type of Study
3.2. Study Population
3.3. Sampling
3.4. Data Collection
3.4.1. Data Collection Tools
3.4.2. Data Collected
3.4.3. Data Processing
3.5. Data Analysis
3.6. Limits
3.7. Ethical Considerations
4.1. Evolution of Exclusive Breastfeeding from 2010-2011 to 2019
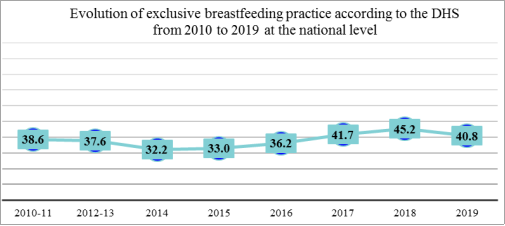
4.1.1. Evolution of Exclusive Breastfeeding at the National Level
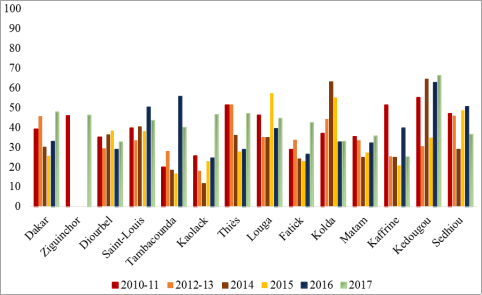
4.1.2. Evolution of Exclusive Breastfeeding at the Regional Level
4.1.3. Ranking of Regions According to the National Average for 2010-2017
4.2. Descriptive Results According to the DHS 2017 Data
4.3. Analysis Result
5.1. Evolution of Exclusive Breastfeeding in Senegal According to the DHS from 2010-2011 to 2019
5.2. Factors Associated with Exclusive Breastfeeding
DHS surveys | 2010-1011 | 2012-2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|---|---|---|
Number of households selected | 8212 | 4 399 | 4 400 | 1 846 | 4 708 | 8 800 | 4 708 | 4 708 |
Number of households surveyed | 7902 | 4 175 | 4 231 | 1 754 | 4 437 | 8 380 | 4 592 | 4 538 |
Household response rate (%) | 98,40 | 98,70 | 98,70 | 98,20 | 98,60 | 98,30 | 99,40 | 99,10 |
Number of eligible women | 16931 | 9 042 | 8 831 | 3 367 | 9 244 | 17 586 | 9 673 | 8 998 |
Number of eligible women surveyed | 15688 | 8 636 | 8 488 | 3 244 | 8 865 | 16 787 | 9 414 | 8 649 |
Response rate for eligible women (%) | 92,20 | 95,50 | 96,10 | 96,30 | 95,90 | 95,50 | 97,30 | 96,1 |
Number of women aged 15-49 with children under two surveyed | 4502 | 2512 | 2377 | 2399 | 2312 | 4416 | 2434 | 2336 |
Socio-demographic characteristics | Frequency absolute N=4368 | Frequency Relative (%) |
|---|---|---|
Mother's age | ||
15-19 | 377 | 8.6 |
20-24 | 985 | 22.5 |
25-29 | 1,102 | 25.2 |
30-34 | 976 | 22.3 |
35-39 | 601 | 13.8 |
40-44 | 268 | 6.1 |
45-49 | 58 | 1.3 |
Place of residence (4367) | ||
rural | 2,798 | 64.1 |
urban | 1,57 | 35.9 |
Religion | ||
Muslim | 4,255 | 97.4 |
Chistian | 112 | 2.6 |
Unknow | 1 | |
Ethnic group | ||
Wolof | 1,583 | 36.2 |
Poular | 1,207 | 27.6 |
Serere | 793 | 18.2 |
Mandingue/Socé | 264 | 6.0 |
Autres | 522 | 11.9 |
Household wealth quintile | ||
poorest | 1,068 | 24.4 |
poorer | 975 | 22.3 |
middle | 901 | 20.6 |
richer | 751 | 17.2 |
richest | 674 | 15.4 |
Mother's level of education | ||
No eduque | 2,614 | 59.9 |
Primary | 935 | 21.4 |
Secondary | 696 | 15.9 |
High | 122 | 2.8 |
Literacy | ||
Able to read only parts of or Whole sentence | 1,486 | 34.2 |
Cannot read | 2,853 | 65.8 |
Unknown | 29 | |
Early marriage | ||
No | 2,348 | 55.5 |
Yes | 1,881 | 44.5 |
Unknown | 139 | |
Age 1st marriage | ||
Before 15 years | 537 | 12.7 |
15-17 years | 1,344 | 31.8 |
From age 18 | 2,348 | 55.5 |
Unknown | 139 | |
Polygamy | ||
Non | 2,982 | 72.9 |
Oui | 1,107 | 27.1 |
Unknown | 279 | |
Household Size | ||
Large household (8) | 3,243 | 74.2 |
Medium household (8 and 5) | 745 | 17.1 |
Small household (5) | 380 | 8.7 |
Occupation of mothers’ | ||
Non | 1,923 | 46.8 |
Oui | 2,186 | 53.2 |
Unknown | 259 | |
Mother's health care decision | ||
Husband | 3,057 | 74.6 |
Wife herself | 954 | 23.3 |
Someone else | 70 | 1.7 |
Other | 15 | 0.4 |
Unknown | 272 | |
Time taken to search for water | ||
On site | 2,604 | 62.7 |
At least One hour | 1,462 | 35.2 |
Less than an hour | 86 | 2.1 |
Unknown | 216 | |
Access to media | ||
Yes | 4,008 | 91.8 |
No | 360 | 8.2 |
Distance travelled to seek healthcare | ||
more than 15 km | 1,241 | 28.4 |
less than 15 km | 3,127 | 71.6 |
Gyneco-obstetrical characteristics | Frequency absolute | Frequency Relative (%) |
|---|---|---|
Prenatal consultation (PNC) | ||
4PNC++ | 1,84 | 49.5 |
Less than 4 PCN | 1,799 | 48.4 |
No visit PCN | 76 | 2.0 |
Unknown | 653 | |
Place of delivery | ||
Public | 3,321 | 76.3 |
Home | 808 | 18.6 |
Private | 165 | 3.8 |
Other | 56 | 1.3 |
Unknown | 18 | |
Delivery assistance by qualified personnel | ||
Yes | 3,084 | 70.6 |
No | 1,284 | 29.4 |
Use modern contraception | ||
Yes | 3,094 | 70.8 |
No | 1,274 | 29.2 |
Cesarean delivery | ||
No | 4,119 | 94.3 |
Yes | 248 | 5.7 |
Unknown | 1 | |
Child characteristics | Frequency absolute | Frequency Relative (%) |
|---|---|---|
Birth rank | ||
1 rank | 1,079 | 24.7 |
2 rank | 847 | 19.4 |
3 rank | 658 | 15.1 |
4 rank | 544 | 12.5 |
5 rank | 394 | 9.0 |
6 rank | 845 | 19.4 |
Sex | ||
Male | 2,207 | 50.5 |
Female | 2,161 | 49.5 |
Birth weight | ||
>= 2500g | 2,714 | 90.3 |
< 2500 g | 292 | 9.7 |
Unknown | 1,362 | |
Independent variables | Exclusive breastfeeding practice | ||
|---|---|---|---|
No N = 3887 | Yes N = 481 | p-value | |
Mother's average age and standard deviation | 28.7 Ecart type:6.9 | 27.8 Ecart type:7.0 | 0.032 |
Mother's age | 0.7 | ||
15-19 | 328 (86.8%) | 50 (13.2%) | |
20-24 | 872 (88.6%) | 112 (11.4%) | |
25-29 | 974 (88.4%) | 128 (11.6%) | |
30-34 | 883 (90.5%) | 93 (9.5%) | |
35-39 | 534 (88.8%) | 67 (11.2%) | |
40-44 | 243 (90.6%) | 25 (9.4%) | |
45-49 | 53 (90.6%) | 6 (9.4%) | |
Place of residence | 0.7 | ||
Rural | 2,485 (88.8%) | 313 (11.2%) | |
Urban | 1,402 (89.3%) | 168 (10.7%) | |
Religion | 0.11 | ||
Chistian | 94 (83.5%) | 19 (16.5%) | |
Muslim | 3,793 (89.1%) | 462 (10.9%) | |
Unknown | 1 | 0 | |
Ethnic group | 0.2 | ||
Autres | 446 (85.5) | 76 (14.5) | |
Mandingue/Socé | 235 (89.1) | 29 (10.9) | |
Poular | 1,072 (88.8) | 135 (11.2) | |
Serere | 722 (91.1) | 71 (8.9) | |
Wolof | 1,412 (89.2) | 171 (10.8) | |
Household wealth quintile | 0.9 | ||
Middle | 802 (89.0%) | 99 (11.0%) | |
Poorer | 860 (88.2%) | 115 (11.8%) | |
Poorest | 957 (89.7%) | 110 (10.3%) | |
richer | 664 (88.4%) | 87 (11.6%) | |
richest | 604 (89.6%) | 70 (10.4%) | |
Mother's level of education | 0.2 | ||
High | 108 (88.3%) | 14 (11.7%) | |
No eduque | 2,353 (90.0%) | 261 (10.0%) | |
Primary | 822 (88.0%) | 113 (12.0%) | |
Secondary | 603 (86.6%) | 93 (13.4%) | |
Unknown | 0 | 0 | |
Literacy | 0.027 | ||
Able to read only parts or whole sentence | 1,295 (87.2%) | 190 (12.8%) | |
Cannot read | 2,570 (90.1%) | 284 (9.9%) | |
Unknown | 22 | 7 | |
Early marriage | 0.5 | ||
No | 2,081 (88.6%) | 267 (11.4%) | |
Yes | 1,680 (89.3%) | 200 (10.7%) | |
Unknown | 126 | 13 | |
Age at first marriage | 0.8 | ||
Under 15 | 478 (89.0) | 59 (11.0) | |
15-17 years old | 1,202 (89.5) | 141 (10.5) | |
From age 18 | 2,081 (88.6) | 267 (11.4) | |
Unknown | 126 | 13 | |
Birth rank | 0.3 | ||
1 rank | 950 (88.1) | 129 (11.9) | |
2 rank | 772 (91.2) | 75 (8.8) | |
3 rank | 575 (87.4) | 83 (12.6) | |
4 rank | 487 (89.6) | 57 (10.4) | |
5 rank | 354 (89.8) | 40 (10.2) | |
6 rank | 748 (88.5) | 97 (11.5) | |
PreNatal Consultation (PNC) | 0.6 | ||
4 PNC ++ | 1,625 (88.3) | 216 (11.7) | |
Less than 4 PNC | 1,597 (88.8) | 202 (11.2) | |
No PNC | 70 (91.8) | 6 (8.2) | |
Unknown | 595 | 57 | |
Place of delivery | 0.5 | ||
Other | 51 (90.6) | 5 (9.4) | |
Home | 730 (90.3) | 78 (9.7) | |
Private | 151 (91.6) | 14 (8.4) | |
Public | 2,942 (88.6) | 379 (11.4) | |
Unknown | 13 | 5 | |
Birth assistance by qualified personnel | 0.028 | ||
No | 1,165 (90.7) | 119 (9.3) | |
Yes | 2,722 (88.3) | 362 (11.7) | |
Polygamy | 0.3 | ||
No | 2,634 (88.4) | 347 (11.6) | |
Yes | 994 (89.7) | 114 (10.3) | |
Unknown | 259 | 20 | |
Household Size | 0.7 | ||
Large household (>8) | 2,877 (88.7) | 366 (11.3) | |
Medium household (≤8 and>5) | 671 (90.1) | 74 (9.9) | |
Small household (≤5) | 339 (89.2) | 41 (10.8) | |
Mother's occupation | <0.001 | ||
No | 1,645 (85.6) | 278 (14.4) | |
Yes | 2,000 (91.5) | 187 (8.5) | |
Unknown | 242 | 17 | |
Mother's health care decision | 0.8 | ||
Other | 14 (93.3) | 1 (6.7) | |
Woman herself | 848 (88.9) | 106 (11.1) | |
Husband | 2,708 (88.6) | 349 (11.4) | |
Someone else | 65 (92.1) | 6 (7.9) | |
Unknown | 253 | 19 | |
Time taken to find water | 0.9 | ||
At least one hour | 1,303 (89.1) | 159 (10.9) | |
Less than an hour | 76 (88.4) | 10 (11.6) | |
On site | 2,327 (89.4) | 277 (10.6) | |
Unknown | 181 | 35 | |
Media access | 0.003 | ||
No | 303 (84.2) | 57 (15.8) | |
Yes | 3,584 (89.4) | 424 (10.6) | |
Distance travelled to seek healthcare | 0.3 | ||
More than 15 km | 1,115 (89.8) | 127 (10.2) | |
Less than 15 km | 2,772 (88.7) | 354 (11.3) | |
Use contraception moderne | <0.001 | ||
No | 2,695 (87.1) | 399 (12.9) | |
Yes | 1,193 (93.6) | 82 (6.4) | |
Caesarean section | 0.022 | ||
No | 3,652 (88.7) | 467 (11.3) | |
Yes | 234 (94.5) | 14 (5.5) | |
Unknown | 1 | 0 | |
Sex | 0.9 | ||
Female | 1,922 (89.0) | 239 (11.0) | |
Male | 1,965 (89.0) | 242 (11.0) | |
Birth weight | 0.8 | ||
≥ 2500 g | 2,381 (87.7) | 333 (12.3) | |
<2500 g | 258 (88.3) | 34 (11.7) | |
Unknown | 1,249 | 114 | |
Characteristic | AOR1 | 95% CI1 |
|---|---|---|
Age of Mother | ||
45-49 | — | — |
15-19 | 2.47 | 0.61, 12.8 |
20-24 | 2.56 | 0.73, 12.1 |
25-29 | 2.70 | 0.82, 12.3 |
30-34 | 1.68 | 0.53, 7.49 |
35-39 | 1.64 | 0.52, 7.29 |
40-44 | 0.75 | 0.21, 3.64 |
Ethnie | ||
Serere | — | — |
Autres | 0.58 | 0.35, 0.95 |
Mandingue/Socé | 0.86 | 0.48, 1.55 |
Poular | 0.84 | 0.54, 1.30 |
Wolof | 0.59 | 0.38, 0.90 |
Literacy | ||
Able to read only parts of sentence or whole sentence | — | — |
Cannot read | 0.71 | 0.53, 0.95 |
Birth rank | ||
1 | — | — |
2 | 1.18 | 0.76, 1.83 |
3 | 1.54 | 0.94, 2.53 |
4 | 1.71 | 0.97, 3.02 |
5 | 1.82 | 0.95, 3.47 |
A partir de 6 | 3.20 | 1.68, 6.17 |
Mother's occupation | ||
Non | — | — |
Oui | 0.60 | 0.46, 0.79 |
Media access | ||
Non | — | — |
Oui | 0.57 | 0.37, 0.90 |
Use contraception moderne | ||
Non | — | — |
Oui | 0.53 | 0.38, 0.72 |
Birth weight | ||
Non (>=2,5Kg) | — | — |
Oui (<2,5 kg) | 0.71 | 0.43, 1.12 |
| [1] |
World Health Organization (WHO), United Nations Children's Fund (UNICEF) & World Bank. and trends in child malnutrition: UNICEF /WHO / The World Bank Group joint child malnutrition estimates: In: key findings of the 2021edition. World Health Organization, 2021.
https://apps.who.int/iris/handle/10665/341135 [Accessed February 2022]. |
| [2] | Black RE, Victora CG, Walker SP, Bhutta ZA, Parul C, De Onis M, Ezzati M, Grantham-McGS, Katz J, Martorell R and R Uauy Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet, 2013; Volume 382, ISSUE 9890, P427-451, June 06, 2013 |
| [3] | UNICEF-OMS-Groupe de la Banque mondiale. Child malnutrition estimates for the indicators stunting, wasting, overweight and underweight describe the magnitude and patterns of under- and overnutrition. UNICEF-WHO-WB Joint Child Malnutrition Estimates inter-agency group updates regularly the global and regional estimates in prevalence and numbers for each indicator. Edition d’avril 2021. Consulté le 2 Mai 2022. |
| [4] |
ALIVE AND THRIVE:
http://www.aliveandthrive.org/fr/news/stronger-with-breastmilk-only-campaign-aims-to-save-lives-reduce-child-malnutrition-in-west-and consulté le 2 septembre 2022. |
| [5] | Black RE, Allen LH, Bhutta ZA et al, for the Maternal and Child Undernutrition Group. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008; 371: 243-260. |
| [6] | Nigel C Rollins, MD, Nita Bhandari, PhD, Nemat Hajeebhoy, MHS, Susan Horton, PhD, Chessa K Lutter, PhD, Jose C Martines, PhD et al. Why invest, and what it will take to improve breastfeeding practices? SERIES|BREASTFEEDING| The Lancet VOLUME 387, ISSUE 10017, P491-504, JANUARY 30, 2016 Published: January 30, 2016. |
| [7] |
Horta BV and CG Victora Long-term effects of breastfeeding-a systematic review, 2013. ISBN 9789241505307.
https://apps.who.int/iris/handle/10665/79198 Accessed November 2021. |
| [8] | Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J Murch S, Sankar MJ, Walker N, Rollins NC; et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016; 387(10017): 475–490. |
| [9] | WHO. Infant and Young Child feeding. Model Chapter for textbooks for medical students and allied health professionals. Geneva: World Health Organization, 2009. |
| [10] | Victora CG, Smith PG, Vaughan JP, Nobre LC, Lombardi C, Teixeira AM, Fuchs SM, Moreira LB, Gigante LP, Barros FC. 1987. Evidence for protection by breast-feeding against infant deaths from infectious diseases in Brazil. Lancet. 2: 319-22. |
| [11] |
United Nations Children’s Fund. UNICEF data: monitoring the situation of children and women. Access the data: infant and young child feeding.
http://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/ (consulté le 7 mars 2018). |
| [12] | Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, Bellagio Child Survival Study G. How many child deaths can we prevent this year? Lancet 2003; Volume 362, ISSUE 9377, P65-71, JULY 05, 2003 |
| [13] | OMS-UNICEF: |
| [14] | Bhutta ZA, Ahmed T, Black RE et al. for the Maternal and Child Undernutrition Group What works? Interventions for maternal and child undernutrition and survival. Lancet. 2008; 371: 417-440. |
| [15] | Walters D, Phan L, Mathisen R. The cost of not breastfeeding: global results from a new tool. Health Policy and Planning. 2019 June 24. |
| [16] | D. Turck. Allaitement maternel: les bénéfices pour la santé de l'enfant et de sa mère. Breast feeding: health benefits for child and mother. Archives de Pédiatrie. Volume 12, Supplement 3, December 2005, Pages S145-S165 |
| [17] | Armstrong J, Reilly JJ & Child Health Information Tea. Breastfeeding and lowering the risk of childhood obesity. Lancet volume 359, ISSUE 9322, P2003-2004, June 08, 2002 |
| [18] | Horta BL, Bahl R, Martines JC & Victora CG (2007) Evidence on the Long-Term Effects of Breastfeeding: Systematic Reviews and Meta-Analysis. WHO, Geneva. |
| [19] | Sadauskaite-Kuehne V, Samuelsson U, Jasinskiene E, Padaiga Z, Urbonaite B, Edenvall H & Ludvigsson J (2002) Severity at onset of childhood type 1 diabetes in countries with high and low incidence of the condition. Diabetes Research and Clinical Practice Volume 55, ISSUE 3, P247-254, MARCH 2002. |
| [20] | Singhal A, Cole TJ, Fewtrell M & Lucas A (2004) Breastmilk feeding and lipoprotein profile in adolescents born preterm: follow-up of a prospective randomized study. Lancet volume 363, ISSUE 9421, P1571-1578, MAY 15, 2004. |
| [21] | The Collaborative Group on Hormonal Factors in Breast Cancer (2002) Breast cancer and breastfeeding: collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease. Lancet Volume 360, ISSUE 9328, P187-195, JULY 20, 2002. |
| [22] |
UNICEF. 2021. Infant and Young Child Feeding: Exclusive breastfeeding. Dans: UNICEF Data: Monitoring the Situation of Children and Women.
https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding |
| [23] | Imdad, A., Yakoob, MY, Bhutta, ZA. 2011. Effect on breastfeeding promotion interventions on breastfeeding rates, with special focus on developing countries. BMC Public Health. 11 (Suppl.3): S24. |
| [24] | Isabelle Michaud-Létourneau, Marion Gayard, David Louis Pelletier. Contribution of the Alive & Thrive–UNICEF advocacy efforts to improve infant and young child feeding policies in Southeast Asia First published: 22 February 2019. |
| [25] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal. Enquête Démographique et de Santé Continue (EDS-Continue), 2017. The DHS Program ICF Rockville, Maryland, USA Septembre 2018. |
| [26] | Enquête Démographique et de Santé à Indicateurs Multiples Sénégal (EDS-MICS) 2010-2011 Rapport final Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal MEASURE DHS ICF International Calverton, Maryland, USA Février 2012. |
| [27] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue) 2019. The DHS Program ICF Rockville, Maryland, USA Novembre 2020. |
| [28] | Agence Nationale de la Statistique et de la Démographie (ANSD): Rapport sur la population du Sénégal 2020. |
| [29] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal. Enquête Démographique et de Santé Continue (EDS-Continue) 2014. The DHS Program ICF International Rockville, Maryland, USA Mai 2015. |
| [30] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue) 2018. The DHS Program ICF Rockville, Maryland, USA Novembre 2018. |
| [31] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal. Les comptes nationaux trimestriels (3ème Trimestre 2019): synthèse de l’évolution de l’activité économique au troisième trimestre 2019. |
| [32] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal. Note sur les évolutions économiques récentes. |
| [33] | Agence Nationale de la Statistique et de la Démographie (ANSD): Rapport définitf du RGPHAE 2013; Publication (Jour/Mois/Année), 2014; Editeur, Agence Nationale de la Statistique et de la Démographie (ANSD); Ville, Dakar. |
| [34] | COSFAM/MI/UCAD. Rapport de la situation de base en vitamine A, fer et zinc chez les enfants de 12-59 mois et les femmes en âge de procréer (15-49 ans) dans le cadre du programme de fortification des aliments en micronutriments au Sénégal. 2012. p 153. |
| [35] | Division de l’Alimentation et de la Nutrition, Ministere de la Santé et de l’Action Sociale Dakar, Senegal. Enquête Nutritionnelle Nationale Utilisant la Méthodologie SMART: Rapport Final. Dakar, Sénégal. 2016b. p 87. Available at: |
| [36] | Anna Vanderkooy, Elaine L. Ferguson, Ndèye Yaga Sy, Rosenette Kane, Maty Diagne, Aminata Mbodji and Alissa M. Pries4. High unhealthy food and beverage consumption is associated with poor diet quality among 12–35-month-olds in Guédiawaye Department, Senegal. Frontiere Nutrition., 19 June 2023, Sec. Nutritional Epidemiology, Volume 10 - 2023, P: 1-12. |
| [37] | Agence Nationale de la Statistique et de la Démographie (ANSD). Enquête Démographique et de Santé Continue au Sénégal (EDS-Continue) 2012-2013. Rapport final 1ère année Dakar, Sénégal MEASURE DHS ICF International Calverton, Maryland, USA Juillet 2013. |
| [38] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal Enquête Démographique et de Santé Continue au Sénégal (EDS-Continue) 2015. Rapport sur les Indicateurs Clés 3ème année. The DHS Program ICF International Rockville, Maryland, USA March 2016. |
| [39] | Agence Nationale de la Statistique et de la Démographie (ANSD) Dakar, Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue) 2016. The DHS Program ICF Rockville, Maryland, USA Août 2017. |
| [40] | The DHS Program - Questionnaires and Manuals. |
| [41] | Alive & Thrive and UNICEF. Factors Influencing the Practice of Exclusive Breastfeeding and Other Infant Feeding Practices in the First Six Months of Life in West and Central Africa. Alive & Thrive and UNICEF: 2022. |
| [42] | Sakamoto Y, Ishiguro M, Kitagawa G, 1986. Akaike information criterion statistics [Internet]. Tokyo, Dordrecht, Boston: KTK Scientific Publishers ; D. Reidel ; Sold and distributed in the U.S.A. and Canada by Kluwer Academic Publishers; 1986 [cité 21 mai 2023]. 290 p. (Mathematics and its applications (D. Reidel Publishing Company)). Disponible sur: |
| [43] |
Hosmer DW, Lemeshow S. Apply logistic regression. New-York, Willey-Blackwell, 2013, 528p [Internet]. [cité 21 mai 2023]. Disponible sur:
https://www.wiley.com/en-us/Applied+Logistic+Regression%2C+3rd+Edition-p-9780470582473 |
| [44] | AMERICAN ACADEMY OF PEDIATRICS (AAP). Breastfeeding and the use of human milk. Pediatrics, 2012; 129: e827-841. |
| [45] |
ORGANISATION MONDIALE DE LA SANTÉ (OMS). Déclaration: alimentation au sein exclusive pendant six mois pour les nourrissons du monde entier.
http://www.who.int/mediacentre/news/statements/2011/breastfeeding_20110115/fr/.2011 |
| [46] | Organisation Mondiale de la Santé: Cibles mondiales de nutrition 2025: Note d’orientation sur l’allaitement au sein. |
| [47] | Boubacar Gueye, Oumar Bassoum, Dieynaba Bassoum, Ndéye Marième Diagne, Martial Coly Bop, Alioune Badara Tall, Abdoul Aziz Ndiaye, Cheikh Tacko Diop, Papa Gallo Sow, Ousseynou Ka, Ibrahima Seck. Facteurs associés à la pratique de l´allaitement maternel exclusif chez les mères d´enfants âgés de 6 à 12 mois dans la commune de Kaolack (Sénégal). Pan African Medical Journal. 2023; 45: 55. |
| [48] | Mar MM. Étude des facteurs associés à la pratique de l´allaitement maternel exclusif chez les mères d´enfants âgés de 6 à 12 mois dans la commune de Thiès (Thèse de doctorat d´état en médecine) Dakar. Université Cheikh Anta Diop de Dakar Faculté de Médecine de Pharmacie et d´Odontostomatologie, 2021; N°106: 20140676Q. |
| [49] | UNICEF. 2022. L’alimentation du nourrisson et du jeune enfant. Dans: UNICEF. [Consulté le 6 avril2023]. |
| [50] | Amed Coulibaly, Odile Ake Tano, Joseph Bénie Bi Vroh, Youssouf Traoré, N’cho Simplice Dagnan acteurs socioprofessionnels et pratique de l'allaitement exclusif par les primipares à Abidjan (Côte d'Ivoire. Dans Santé Publique 2014/4 (Vol. 26), pages 555 à 562). |
| [51] | Leena Hannula Marja Kaunonen, Marja-Terttu Tarkka: A systematic review of professional support interventions for breastfeeding. (2008) Journal of Clinical Nursing 17, 1132–1143 First published: 14 April 2008 |
| [52] | BRITTON, C., MCCORMICK, F. M., RENFREW, M. J., et al. Support for breastfeeding mothers (Review). The Cochrane Collaboration. 2007. John Wiley & Sons, Ltd; 2007. |
| [53] | AKSU H, KÜÇÜK M, DÜZGÜN G. The effect of postnatal breastfeeding education/support offered at home 3 days after delivery on breastfeeding duration and knowledge: A randomized trial. The Journal of Maternal-Fetal and neonatal medicine, volume 24, February 2011; 24: 354-361. |
| [54] | BEAKE S, PELLOWE C, DYKES F, SCHMIED V, BICK D. A systematic review of structured compared with non-structured breastfeeding programs to support the initiation and duration of exclusive and any breastfeeding in acute and primary health care settings. Maternal and Child Nutrition, April 2012; 8: 141-161.]. First published: 20 December 2011. |
| [55] | Mahamadou Traoré, Issa Traore, Oumar Thiero, Aminata Sidibé, Habiyata Maiga, Oumar A. Maiga, ChakaCoulibaly, ModiboDiarra, Hamadoun Sangho. Facteurs associés à la cessation de l’allaitement maternel exclusif en milieux rural et urbain au Mali Dans Santé Publique 2019/3 (Vol. 31), pages 451 à 458. Mis en ligne sur Cairn. info le 25/09/2019. |
| [56] | LAURENCE M GRUMMER-STRAWN. The Effect of Changes in Population Characteristics on Breastfeeding Trends in Fifteen Developing Countries. International Journal of Epidemiology, Volume 25, Issue 1, February 1996, Pages 94–102, |
| [57] | World Health Organization & United Nations Children's Fund: Maternal, Newborn, Child & Adolescent Health & Ageing (MCA), Nutrition and Food Safety (NFS). Number of pages 32 Reference numbers ISBN: 978-92-4-004460. |
APA Style
Camara, M. D., Ndiaye, I., Gueye, B., Dramé, A., Bassoum, O., et al. (2024). Evolution of Exclusive Breastfeeding Practices According to Continuous Demographic and Health Surveys (DHS-C) from 2010-2011 to 2019 and Associated Factors in Senegal. World Journal of Public Health, 9(2), 156-177. https://doi.org/10.11648/j.wjph.20240902.16
ACS Style
Camara, M. D.; Ndiaye, I.; Gueye, B.; Dramé, A.; Bassoum, O., et al. Evolution of Exclusive Breastfeeding Practices According to Continuous Demographic and Health Surveys (DHS-C) from 2010-2011 to 2019 and Associated Factors in Senegal. World J. Public Health 2024, 9(2), 156-177. doi: 10.11648/j.wjph.20240902.16
AMA Style
Camara MD, Ndiaye I, Gueye B, Dramé A, Bassoum O, et al. Evolution of Exclusive Breastfeeding Practices According to Continuous Demographic and Health Surveys (DHS-C) from 2010-2011 to 2019 and Associated Factors in Senegal. World J Public Health. 2024;9(2):156-177. doi: 10.11648/j.wjph.20240902.16
@article{10.11648/j.wjph.20240902.16,
author = {Maty Diagne Camara and Ibrahima Ndiaye and Boubacar Gueye and Aboubacry Dramé and Oumar Bassoum and Anna Toure and Aita Sarr-Cisse and Aminata Ndiaye Coly and Maguette Fall Beye and Nafissatou Ba Lo},
title = {Evolution of Exclusive Breastfeeding Practices According to Continuous Demographic and Health Surveys (DHS-C) from 2010-2011 to 2019 and Associated Factors in Senegal
},
journal = {World Journal of Public Health},
volume = {9},
number = {2},
pages = {156-177},
doi = {10.11648/j.wjph.20240902.16},
url = {https://doi.org/10.11648/j.wjph.20240902.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20240902.16},
abstract = {Introduction: The first two years of a child's life are particularly important. Inadequate breastfeeding practices during this period considerably compromise the health, development and survival of infants, children and mothers. Several studies have assessed the impact of breastfeeding on infant mortality. The objectives of our study were to investigate changes in exclusive breastfeeding practices during the first six months of life according to DHS data from 2010-2011 to 2019 and to identify the various associated factors. Methodology: This is a quantitative analysis of secondary data based on cross-sectional data from the DHS from 2010-2011 to 2019 on changes in exclusive breastfeeding practices for infants under six months of age. Our study focused on women aged 15 to 49 years interviewed during the DHS and residing in Senegal at the time of the various surveys who had children under two years of age. Data were collected on exclusive breastfeeding rates in different years, the socio-demographic and gyneco-obstetric characteristics of mothers, and the characteristics of newborn children. A multivariate analysis was performed to identify factors associated with exclusive breastfeeding. Results: showed that exclusive breastfeeding rates remained below 50% from 2010-11 to 2019. Analysis by region showed a disparity between the different regions. The associated factors were: ethnic group: Wolof are less likely to practice EBF with an adjusted AOR of 0.59 with a CI95: [0.38, 0. 90], maternal literacy: mothers who could not read were less likely to perform EBF with an adjusted AOR of 0.71 and a CI95: [0.53-095], birth order: mothers with 6 or more children were more likely to perform EBF, with an AOR of 3.20 and a CI95: [1.68-6.17], maternal occupation: Working mothers were less likely to practice EBF than non-working mothers, with an AOR of 0.60 and a CI95 [0.46-0.79], access to the media: Mothers with access to the media were less likely to practice assisted fertilization, with an AOR of 0.57 and a CI95: [0.37-0.90] and use of modern contraception: Mothers using modern contraception were less likely to practice exclusive breastfeeding, with an AOR of 0.53 and a CI95: [0.38-0.72]. Conclusion: Despite all the efforts made by the Senegalese government and its technical and financial partners, rates are still low. To strengthen the practice of exclusive breastfeeding, it is important and urgent to design and implement innovative evidence-based interventions covering the different levels of the socio-ecological model (individuals, families, communities and public policies).
},
year = {2024}
}
TY - JOUR T1 - Evolution of Exclusive Breastfeeding Practices According to Continuous Demographic and Health Surveys (DHS-C) from 2010-2011 to 2019 and Associated Factors in Senegal AU - Maty Diagne Camara AU - Ibrahima Ndiaye AU - Boubacar Gueye AU - Aboubacry Dramé AU - Oumar Bassoum AU - Anna Toure AU - Aita Sarr-Cisse AU - Aminata Ndiaye Coly AU - Maguette Fall Beye AU - Nafissatou Ba Lo Y1 - 2024/05/10 PY - 2024 N1 - https://doi.org/10.11648/j.wjph.20240902.16 DO - 10.11648/j.wjph.20240902.16 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 156 EP - 177 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20240902.16 AB - Introduction: The first two years of a child's life are particularly important. Inadequate breastfeeding practices during this period considerably compromise the health, development and survival of infants, children and mothers. Several studies have assessed the impact of breastfeeding on infant mortality. The objectives of our study were to investigate changes in exclusive breastfeeding practices during the first six months of life according to DHS data from 2010-2011 to 2019 and to identify the various associated factors. Methodology: This is a quantitative analysis of secondary data based on cross-sectional data from the DHS from 2010-2011 to 2019 on changes in exclusive breastfeeding practices for infants under six months of age. Our study focused on women aged 15 to 49 years interviewed during the DHS and residing in Senegal at the time of the various surveys who had children under two years of age. Data were collected on exclusive breastfeeding rates in different years, the socio-demographic and gyneco-obstetric characteristics of mothers, and the characteristics of newborn children. A multivariate analysis was performed to identify factors associated with exclusive breastfeeding. Results: showed that exclusive breastfeeding rates remained below 50% from 2010-11 to 2019. Analysis by region showed a disparity between the different regions. The associated factors were: ethnic group: Wolof are less likely to practice EBF with an adjusted AOR of 0.59 with a CI95: [0.38, 0. 90], maternal literacy: mothers who could not read were less likely to perform EBF with an adjusted AOR of 0.71 and a CI95: [0.53-095], birth order: mothers with 6 or more children were more likely to perform EBF, with an AOR of 3.20 and a CI95: [1.68-6.17], maternal occupation: Working mothers were less likely to practice EBF than non-working mothers, with an AOR of 0.60 and a CI95 [0.46-0.79], access to the media: Mothers with access to the media were less likely to practice assisted fertilization, with an AOR of 0.57 and a CI95: [0.37-0.90] and use of modern contraception: Mothers using modern contraception were less likely to practice exclusive breastfeeding, with an AOR of 0.53 and a CI95: [0.38-0.72]. Conclusion: Despite all the efforts made by the Senegalese government and its technical and financial partners, rates are still low. To strengthen the practice of exclusive breastfeeding, it is important and urgent to design and implement innovative evidence-based interventions covering the different levels of the socio-ecological model (individuals, families, communities and public policies). VL - 9 IS - 2 ER -
Institute of Health and Development Department of Preventive Medicine and Public Health, Faculty of Medicine, Pharmacy and Odontology, Cheikh Anta Diop University, Dakar, Senegal
Biography: Maty Diagne Camara is a public health specialist, nutritionist and assistant professor at Cheikh Anta Diop University in Dakar. She holds a doctorate in medicine from Cheikh Anta Diop University in Dakar, a certificate of specialization in public health and a master's degree in public health with a nutrition option. She has 20 years' experience in public health. She was head doctor of a health district before joining the Health and Development Institute at Cheikh Anta Diop University in Dakar. She coordinates the Master's degree in Public Health/Nutrition, specializing in nutrition. She is also head of the Food and Nutrition Division at Senegal's Ministry of Health and Social Action, where I have been coordinating food and nutrition projects and programs since 2013. She is a member of the Senegalese Association of Public Health Professionals (PHPS) and the Senegalese Association of Nutrition and Food.
Research Fields: Infant and Young Child Feeding; Dietary Diversification in Pregnant Women; Routine Vitamin Supplementation in Children 6-59 Months of Age; Factors Associated with Low Birth Weight; Management of Children with Severe Acute Malnutrition
Institute of Health and Development Department of Preventive Medicine and Public Health, Faculty of Medicine, Pharmacy and Odontology, Cheikh Anta Diop University, Dakar, Senegal
Research Fields: Factors Associated with the Completion of Antenatal Care
Université Alioune Diop University of Bambey, Training and Research Unit, Health and Sustainable Development, Dakar, Senegal
Research Fields: Factors associated with practice of exclusive breastfeeding
Department of Mother and Child Health, Ministry of Health and Social Action, Dakar, Senegal
Research Fields: Neonatal mortality according to DHS data in Senegal
Institute of Health and Development Department of Preventive Medicine and Public Health, Faculty of Medicine, Pharmacy and Odontology, Cheikh Anta Diop University, Dakar, Senegal
Research Fields: Determinants of hepatitis B vaccine administration at birth in Senegal. Evaluation of prescription indicators for pediatric outpatient consultations Senegal. Vaccination against tuberculosis, poliomyelitis and hepatitis B Podor district, Senegal. Coverage Timeliness Birth Dose Vaccination Sub-Saharan Africa. Assessment general public's knowledge antibiotic use bacterial resistance
Information