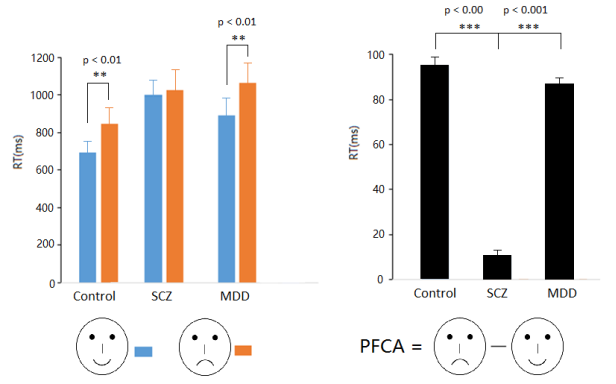
Background: Emotional stimuli affect basic and cognitive operations, such as perception, attention and memory and changes in emotional perception are associated with various mental disorders. Changes in emotional perception are associated with various mental disorders, such as major depressive disorder (MDD) and schizophrenia (SCZ). However, the differences in emotional cognition and their mechanisms among different mental disorders are still unclear. Objective: Different from negative expression processing preferences (attention, memory, etc.), categorizing positive facial expressions are much faster than emotion neutral and negative facial expressions, i.e., positive face classification advantage (PFCA). The present experiment directly investigated the difference in categorizing emotional faces between patients with MDD and SCZ. Main ideas: In healthy controls, happy faces were classified faster than sad faces (i.e., positive face classification advantage, PFCA). Although the ability of expression classification in both MDD and SCZ patients was reduced, the processing patterns of the two groups were different. The PFCA in patients with MDD was similar to that in normal controls. On the contrary, the PFCA was absent in patients with SCZ due to the need to invest more attention resources in classifying a face as happy emotion, suggesting that patients with SCZ have greater obstacles in processing positive facial expressions. Conclusion: The patterns of categorizing emotional faces was different between SCZ and MDD patients, which has important clinical significance for the differential diagnosis of the two diseases and the cognitive evaluation during treatment.
| Published in | American Journal of Applied Psychology (Volume 14, Issue 3) |
| DOI | 10.11648/j.ajap.20251403.11 |
| Page(s) | 70-75 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Major Depressive Disorder, Schizophrenia, Facial Expression, Positive Face Classification Advantage, Face Perception
Controls | SCZ | MDD | ||
|---|---|---|---|---|
RTs (ms) | Happy faces | 626 | 866 | 736 |
Sad faces | 708 | 887 | 826 | |
PFCA size | 82 | 11 | 90 | |
Accuracy (%) | Happy faces | 98.0 | 87.5 | 89.9 |
Sad faces | 95.2 | 85.4 | 88.3 |
MDD | Major Depressive Disorder |
PFCA | Positive Face Classification Advantage |
SCZ | Schizophrenia |
| [1] | Bauser, D. S, Thoma, P., Aizenberg, V., et al. (2012). Face and body perception in schizophrenia: a configural processing deficit? Psychiatry Research, 195(1-2): 9-17. |
| [2] | Benoit, B., Brunelin, J., d’Amato, T., Shirley, F., Mohamed, S., & Hénaff M. (2012). A comparison of facial emotion processing in neurological and psychiatric conditions. Frontiers in Psychology, 3, 98. |
| [3] | Gill, B. K., Balodis, I. M., Minuzzi, L., et al. (2024). Neural correlates of emotion dysregulation in adolescents: a systematic review. Discover Psychology, 4: 31. |
| [4] | Grave, J., Soares, S. C., Martins, M. J., & Madeira, N. (2017). Facial emotion processing in schizophrenia: a review of behavioural and neural correlates. Journal of Clinical Neurosciences and Mental Health, 4: S06. |
| [5] | Häfner, H. (2010). The early Kraepelin's dichotomy of schizophrenia and affective disorder - evidence of separate diseases? European Journal of Psychiatry, 24(2), 98-113. |
| [6] | Halperin, E. & Tagar, M. F. (2017). Emotions in conflicts: understanding emotional processes sheds light on the nature and potential resolution of intractable conflicts. Current Opinion in Psychology, 17: 94-98. |
| [7] | Hwang, H. C., Kim, S. M., & Han, D. H. (2021). Different facial recognition patterns in schizophrenia and bipolar disorder assessed using a computerized emotional perception test and fMRI. Journal of Affective Disorders, 279, 83-88. |
| [8] | Kang, W., Kim, G., Kim, H., & Lee, S. H.. (2019). The influence of anxiety on the recognition of facial emotion depends on the emotion category and race of the target faces. Experimental Neurobiology, 28(2): 261-269. |
| [9] | Karparova, S., Kersting, A., & Suslow, T. (2005). Disengagement of attention from facial emotion in unipolar depression. Psychiatry and Clinical Neurosciences, 59(6): 723-729. |
| [10] | Kohler, C., Walker, J., Martin, E., Healey, K, & Moberg, P. (2010). Facial emotion perception in schizophrenia: a meta-analytic review. Schizophrenia Bulletin, 36, 1009-1019. |
| [11] | Kosonogov, V. V., Vorobyeva, E., Kovsh, E., Ermakov, P. N. (2019). A review of neurophysiological and genetic correlates of emotional intelligence. International Journal of Cognitive Research in Science, Engineering and Education, 7(1): 137–142. |
| [12] | Kramer, M., Stetter, M., Heinisch, C., Baumgart, P., Brüne, M., Mavrogiorgou, P., & Juckel, G. (2024). Emotional context effects on the rating of ambiguous facial expressions in depression and schizophrenia spectrum disorders. Psychiatry, 87(1), 36–50. |
| [13] | Leppänen, J. M., & Hietanen, J. K. (2004). Positive facial expressions are recognized faster than negative facial expressions, but why? Psychological Research, 69, 22–29. |
| [14] | Liang, S., Chen, S., Zhao, L., & Miao, D. (2019). Categorization of emotional faces in schizophrenia patients: An ERP study. Neuroscience Letters, 713, 134493. |
| [15] | Liu, X. F., Liao, Y., Zhou, L., Sun, G., Li, M., & Zhao, L. (2013). Mapping the time course of the positive face classification advantage: an ERP study. Cognition Affective Behavioral Neuroscience, 13, 491–500. |
| [16] | Mendoza, R., Cabral-Calderin, Y., Domínguez, M., et al. (2011) Impairment of emotional expression recognition in schizophrenia: A Cuban familial association study. Psychiatry Research, 185(1-2), 44-48. |
| [17] | Mikhailova, E., Vladimirova, T., Iznak, A., et al. (1996). Abnormal recognition of facial expression of emotions in depressed patients with major depression disorder and schizotypal personality disorder. Biological Psychiatry, 40(8), 697-705. |
| [18] | Mioni, G., Grondin, S., Meligrana, L., et al. (2018). Effects of happy and sad facial expressions on the perception of time in Parkinson’s disease patients with mild cognitive impairment. Journal of Clinical and Experimental Neuropsychology, 40(2), 123-138. |
| [19] | Prisco, M., Oliva, V., Fico, G., Montejo, L., Possidente, C., Bracco, L., et al. (2023). Differences in facial emotion recognition between bipolar disorder and other clinical populations: A systematic review and meta-analysis. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 127, 110847. |
| [20] | Sachs, G., Steger-Wuchse, D., Kryspin-Exner, I., et al. (2004). Facial recognition deficits and cognition in schizophrenia. Schizophrenia Research, 68(1), 27-35. |
| [21] | Šoštarič, M., & Zalar, B. (2011). The overlap of cognitive impairment in depression and schizophrenia: a comparative study. Psychiatria Danubina, 23, 251–25. |
| [22] | Venn, H., Watson, S., Gallagher, P., et al. (2006). Facial expression perception: an objective outcome measure for treatment studies in mood disorders? International Journal of Neuropsychopharmacology, 9(2), 229-245. |
| [23] | Wang, Y., Ge, M., Zhu, G., et al. (2020). Emotion–behavior decoupling in individuals with schizophrenia, bipolar disorder, and major depressive disorder. Journal of Abnormal Psychology, 29(4), 331-342. |
| [24] | Yang, C., Qi, A., Yu, H., et al. (2018). Different levels of facial expression recognition in patients with first-episode schizophrenia: a functional MRI study. General Psychiatry, 31(2), e000014. |
| [25] | Yin, G., Li, H., & Zhao, L. (2020). Dysfunction of categorization of emotional faces in people with schizophrenia. Social Behavior and Personality: An international journal, 48(10), e8673. |
| [26] | Zhao L, Wang X, & Sun G. (2022). Positive classification advantage of categorizing emotional faces in patients with major depressive disorder. Frontiers in Psychology, 13, 734405. |
APA Style
Chen, Y., Wu, J., Che, L., Du, Y., Gao, X. (2025). Different Perceptual Mechanism of Categorizing Emotional Faces in Depression and Schizophrenia. American Journal of Applied Psychology, 14(3), 70-75. https://doi.org/10.11648/j.ajap.20251403.11
ACS Style
Chen, Y.; Wu, J.; Che, L.; Du, Y.; Gao, X. Different Perceptual Mechanism of Categorizing Emotional Faces in Depression and Schizophrenia. Am. J. Appl. Psychol. 2025, 14(3), 70-75. doi: 10.11648/j.ajap.20251403.11
@article{10.11648/j.ajap.20251403.11,
author = {Yang Chen and Jiayu Wu and Lu Che and Yuping Du and Xi Gao},
title = {Different Perceptual Mechanism of Categorizing Emotional Faces in Depression and Schizophrenia
},
journal = {American Journal of Applied Psychology},
volume = {14},
number = {3},
pages = {70-75},
doi = {10.11648/j.ajap.20251403.11},
url = {https://doi.org/10.11648/j.ajap.20251403.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajap.20251403.11},
abstract = {Background: Emotional stimuli affect basic and cognitive operations, such as perception, attention and memory and changes in emotional perception are associated with various mental disorders. Changes in emotional perception are associated with various mental disorders, such as major depressive disorder (MDD) and schizophrenia (SCZ). However, the differences in emotional cognition and their mechanisms among different mental disorders are still unclear. Objective: Different from negative expression processing preferences (attention, memory, etc.), categorizing positive facial expressions are much faster than emotion neutral and negative facial expressions, i.e., positive face classification advantage (PFCA). The present experiment directly investigated the difference in categorizing emotional faces between patients with MDD and SCZ. Main ideas: In healthy controls, happy faces were classified faster than sad faces (i.e., positive face classification advantage, PFCA). Although the ability of expression classification in both MDD and SCZ patients was reduced, the processing patterns of the two groups were different. The PFCA in patients with MDD was similar to that in normal controls. On the contrary, the PFCA was absent in patients with SCZ due to the need to invest more attention resources in classifying a face as happy emotion, suggesting that patients with SCZ have greater obstacles in processing positive facial expressions. Conclusion: The patterns of categorizing emotional faces was different between SCZ and MDD patients, which has important clinical significance for the differential diagnosis of the two diseases and the cognitive evaluation during treatment.
},
year = {2025}
}
TY - JOUR T1 - Different Perceptual Mechanism of Categorizing Emotional Faces in Depression and Schizophrenia AU - Yang Chen AU - Jiayu Wu AU - Lu Che AU - Yuping Du AU - Xi Gao Y1 - 2025/06/23 PY - 2025 N1 - https://doi.org/10.11648/j.ajap.20251403.11 DO - 10.11648/j.ajap.20251403.11 T2 - American Journal of Applied Psychology JF - American Journal of Applied Psychology JO - American Journal of Applied Psychology SP - 70 EP - 75 PB - Science Publishing Group SN - 2328-5672 UR - https://doi.org/10.11648/j.ajap.20251403.11 AB - Background: Emotional stimuli affect basic and cognitive operations, such as perception, attention and memory and changes in emotional perception are associated with various mental disorders. Changes in emotional perception are associated with various mental disorders, such as major depressive disorder (MDD) and schizophrenia (SCZ). However, the differences in emotional cognition and their mechanisms among different mental disorders are still unclear. Objective: Different from negative expression processing preferences (attention, memory, etc.), categorizing positive facial expressions are much faster than emotion neutral and negative facial expressions, i.e., positive face classification advantage (PFCA). The present experiment directly investigated the difference in categorizing emotional faces between patients with MDD and SCZ. Main ideas: In healthy controls, happy faces were classified faster than sad faces (i.e., positive face classification advantage, PFCA). Although the ability of expression classification in both MDD and SCZ patients was reduced, the processing patterns of the two groups were different. The PFCA in patients with MDD was similar to that in normal controls. On the contrary, the PFCA was absent in patients with SCZ due to the need to invest more attention resources in classifying a face as happy emotion, suggesting that patients with SCZ have greater obstacles in processing positive facial expressions. Conclusion: The patterns of categorizing emotional faces was different between SCZ and MDD patients, which has important clinical significance for the differential diagnosis of the two diseases and the cognitive evaluation during treatment. VL - 14 IS - 3 ER -
Department of Neurology, The 904th Hospital of PLA, Wuxi, China;Medical School, Anhui Medical University, Hefei, China
Department of Radiology, Jiangnan University Medical Center, Jiangnan University, Wuxi, China
Information