Malaria is classified as either uncomplicated (UM) or severe (SM), but the mechanism underlying the progression from uncomplicated to severe is still unclear. This study aimed to assess haematologic and biochemical parameters as potential prognostic biomarkers for differentiating SM from UM in a Ghanaian population. A descriptive cross-sectional study was conducted to sample 166 participants, comprising 42 healthy controls, 78 uncomplicated malaria cases, and 46 severe malaria cases. Blood samples were analysed for full blood count, liver function test, renal function test, and serum angiopoietins. Statistical analyses were carried out using GraphPad Prism 9 software. Median and interquartile ranges, Mann-Whitney U test, and Kruskal-Wallis analysis were done to compare groups. The haemoglobin and platelet counts of SM patients were significantly lower than those of the UM group (p < 0.05). However, the White Blood Cell (WBC) counts of severe malaria patients (7.4, IQR: 5.4 - 10.6) were significantly higher than the uncomplicated malaria population (5.7, IQR: 5.0 - 6.5) (p < 0.001). Serum levels of bilirubin (total and direct), alanine transaminase (ALT), aspartate transaminase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), and total proteins in severe malaria were significantly higher than uncomplicated malaria group (p < 0.001). These findings indicate that haemoglobin, platelet, creatinine, urea, AST, ALT, GGT and bilirubin levels may serve as biomarkers for distinguishing severe from uncomplicated malaria.
| Published in | American Journal of Laboratory Medicine (Volume 11, Issue 1) |
| DOI | 10.11648/j.ajlm.20261101.11 |
| Page(s) | 1-8 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Malaria, Haematologic, Biochemical, Prognostic
Demographic characteristics | Uncomplicated malaria | Severe Malaria | ||||
|---|---|---|---|---|---|---|
n | Parasitaemia (/µL) Median (IQR) | P value | n | Parasitaemia (/µL) Median (IQR) | P value | |
Age range | ||||||
<5 | 6 | 7346 (1994 - 26693) | 16 | 29589 (17150 - 102905) | ||
5-17 | 14 | 2808 (1397 - 7568) | 14 | 29793 (14542 - 88230) | ||
≥18 | 58 | 2670 (1109 - 6716) | 0.649 | 16 | 5461 (1871 - 32617) | 0.075 |
Sex | ||||||
Female | 42 | 2670 (680 - 6716) | 22 | 26823 (2595 - 179603) | ||
Male | 36 | 3623 (1208 - 8470) | 0.190 | 24 | 23542 (5856 - 57785) | 0.744 |
Marital status | ||||||
Single | 26 | 2670 (1208 - 8470) | 10 | 26823 (6542 - 50000) | ||
Marriage | 30 | 1275 (787 - 6112) | 0.546 | 4 | 3079 (1777 - 4380) | 0.120 |
Educationb | ||||||
No education | ||||||
Basic | 36 | 2413 (840 - 4400) | 14 | 29793 (9439 - 88705) | ||
Secondary | 18 | 4208 (2670 - 8676) | 14 | 6542 (2282 - 40296) | 0.037 | |
Tertiary | 8 | 1641 (947 - 4531) | 0.071 | NA | ||
Occupationa | ||||||
Student | 18 | 2670 (1208 - 8470) | 8 | 28271 (5250 - 53455) | ||
Informal sector | 32 | 3623 (1103 - 6586) | 8 | 3141 (1871 - 9991) | 0.253 | |
Formal sector | 6 | 2041 (1441 - 9510) | 0.937 | NA | - | |
Variable | Healthy controls (HC), n= 42 | Uncomplicated malaria (UM), n=78 | Severe malaria (SM), n = 46 | P value for UM vs. SM |
|---|---|---|---|---|
Haemoglobin | 11.8 (11.3 - 12.4) | 11.8 (10.8 - 13.1) | 10.9 (9.2 - 12.5) | 0.003 |
WBC | 6.22 (5.0 - 8.1) | 5.7 (5.0 - 6.5) | 7.4 (5.4 - 10.6) | <0.001 |
Platelet count | 270 (229 - 342) | 149 (117 - 196) | 108 (46 - 130) | <0.001 |
NEUT | 41.6 (37.8 - 60.7) | 69.8 (55.2 - 78.1) | 71.5 (61.9 - 82.7) | 0.124 |
LYMP | 46.5 (30.3 - 53.3) | 23.5 (14.9 - 33.5) | 19.0 (12.1 - 29.9) | 0.249 |
MXD | 8.8 (7.2 - 10.2) | 7.7 (6.1 -12.1) | 7.9 (4.7 - 8.9) | 0.012 |
Total Bilirubin | 5.2 (3.8 - 6.2) | 8.1 (5.4 - 10.7) | 11.2 (7.4 - 24.3) | <0.001 |
Direct Bilirubin | 2.1 (1.2 - 3.2) | 3.4 (1.9 - 4.3) | 6.6 (4.1 - 16.1) | <0.001 |
ALT | 7 (6 - 8) | 9 (5.3 - 11.8) | 12 (10 - 18.7) | <0.001 |
AST | 21 (13 - 26) | 17 (12 - 23.3) | 26 (16.3 - 50) | <0.001 |
GGT | 18 (11 - 22) | 20 (13.3 - 28.8) | 40 (18.3 - 49.5) | <0.001 |
ALP | 80 (66 - 97) | 66 (49.3 - 107.5) | 92 (67.8 - 126.8) | 0.054 |
Total protein | 69.2 (64.9 - 70.7) | 64.1 (60 - 69.4) | 68.3 (66.2 - 72.7) | 0.002 |
Albumin | 38.6 (37.1 - 41.6) | 37.6 (35.9 - 39.7) | 35.9 (31.7 -37.9) | 0.002 |
Parasite count | NA | 2808 (1090 - 8189) | 24615 (3943 - 60541) | <0.001 |
Ang-1 | 9.6 (3.5 - 15.3) | 6.3 (3.3 - 8.0) | 3.8 (2.2 - 12.7) | 0.129 |
Ang-2 | 18.7 (12.4 - 22.1) | 15.7 (2.6 - 27.4) | 19.1 (9.0 - 25.8) | 0.429 |
Ang-2/Ang-1 | 1.9 (1.2 - 3.5) | 2.0 (0.6 - 3.2) | 3.1 (1.4 - 5.3) | 0.152 |
UM | Uncomplicated Malaria |
SM | Severe Malaria |
WHO | World Health Organization |
EDTA | Ethylenediaminetetraacetic Acid |
ELISA | Enzyme-linked Immunosorbent Assay |
mL | Milliliters |
FBC | Full Blood Count |
ANG | Angiopoietins |
HC | Healthy Controls |
IQR | Interquartile Range |
ALT | Alanine Transaminase |
AST | Aspartate Transaminase |
GGT | Gamma-Glutamyl Transferase |
ALP | Alkaline Phosphatase |
eGFR | Estimated Glomerular Filtration Rate |
AKI | Acute Kidney Injury |
| [1] | Cullen, K. A. et al. (2011) ‘Division of parasitic diseases and malaria’, Centre for Global Health, Centres for Disease Control and Prevention (CDC). |
| [2] | Anvikar, A. R. et al. (2020) ‘Clinical and epidemiological characterisation of severe Plasmodium vivax malaria in Gujarat. |
| [3] | Diema Konlan, K. et al. (2019) ‘Utilisation of insecticide-treated bed nets (ITNs) among caregivers of children under five years in the Ho municipality’, Interdisciplinary. |
| [4] | Higgins, S. et al. (2016) ‘Dysregulation of angiopoietin 1 plays a mechanistic role in the pathogenesis of cerebral malaria. Science translational medicine,8(358),358ra 128. pp. 1-25. Available at: |
| [5] | Lovegrove, F. E., et al. (2009) ‘Serum angiopoietin-1 and -2 levels discriminate cerebral malaria from uncomplicated malaria and predict clinical outcome in African children’, PLoS ONE, 4(3), pp. 1-8. Available at: |
| [6] | Snow, R. W. et al., (2005) ‘The global distribution of clinical episodes of Plasmodium falciparum malaria’, Nature, 434(7030), pp. 214-217. |
| [7] | Li, G. et al.,(2020) ‘Distribution of malaria patients seeking care in different types of health facilities during the implementation of National Malaria Elimination Programme’, Malaria journal, 19(1), pp. 1-10. |
| [8] | Dhangadamajhi, G. et al. (2019) ‘Effect of Plasmodium falciparum infection on blood parameters and their association with clinical severity in adults of Odisha, India’, Acta tropica, 190, pp. 1-8. Perspectives on infectious diseases, 2019. |
| [9] | Muwonge, H. et al.(2013) ‘How reliable are haematological parameters in predicting uncomplicated Plasmodium falciparum malaria in an endemic region?’, International Scholarly Research Notices, 2013(1), p. 673798. |
| [10] | Zuberi, U. et al. (2024) ‘Altered haematological parameters in children with malaria infection, a systematic review and meta-analysis’, Diagnostic Microbiology and Infectious Disease, 108(4), p. 116190. |
| [11] | Awosolu, O. B. et al. (2021) ‘Prevalence, Parasite Density and Determinants of Falciparum Malaria Among Febrile Children in Some Peri-Urban Communities in Southwestern Nigeria: A Cross-Sectional Study’, Infection and drug resistance, pp. 3219-3232. |
| [12] | Ayyadevara, R. (2022) ‘Effect of malaria on biochemical and haematological parameters: a hospital-based case-control study’, MRIMS Journal of Health Sciences, 10(3), pp. 41-46. |
| [13] | Squire, D. S. et al. (2016) ‘Effect of Plasmodium falciparum malaria parasites on haematological parameters in Ghanaian children’, Journal of parasitic diseases, 40, pp. 303-311. |
| [14] | Bhattacharya, D. (2016) ‘Indian Monsoon Climate and Malaria: Medical Meteorology’, Journal of Malaria Control & Elimination, 5(2), pp. 2-6. |
| [15] | Devineni, S. B. et al. (2015) ‘Study of platelet count in malaria patients and the correlation between the presence and severity of platelet count with type of malaria’, Journal of Evolution of Medical and Dental Sciences, Malaria surveillance-United States, pp. 1-17. |
| [16] | Kumar, N. (2016) ‘Correlation of type of species and parasite density in malaria with platelet count, mean platelet volume and platelet distribution width’, Journal of Evolution of Medical and Dental Sciences-Jemds, 5(89), pp. 6622-6625. |
| [17] | Asare, I. D. (2019) ‘Evaluation of Renal and Hepatic Dysfunction among Children Less than Five Years with Malaria in Jasikan District, Oti Region-Ghana’. University of Ghana. 4(67), pp. 11734-11747. |
| [18] | Koopmans, L. C. et al., (2015) ‘Acute kidney injury in imported Plasmodium falciparum malaria’, Malaria journal, 14(1), pp. 1-7. |
| [19] | Storm, J., & Craig, A. G. (2014). Pathogenesis of cerebral malaria—inflammation and cytoadherence. Frontiers in cellular and infection microbiology, 4, 100. |
| [20] | Fang, Y., Li, C., Shao, R., Yu, H., & Zhang, Q. (2018). The role of biomarkers of endothelial activation in predicting morbidity and mortality in patients with severe sepsis and septic shock in intensive care: a prospective observational study. Thrombosis research, 171, 149-154. |
| [21] | Vinhaes, C. L., et al. (2021). Dissecting disease tolerance in Plasmodium vivax malaria using the systemic degree of inflammatory perturbation. PLoS Neglected Tropical Diseases, 15(11), e0009886. |
| [22] | Rivera-Correa, et al. (2019). Autoantibody levels are associated with acute kidney injury, anaemia and post-discharge morbidity and mortality in Ugandan children with severe malaria. Scientific Reports, 9(1), 14940. |
| [23] | Bhardwaj, N., et al. (2020). Clinicopathological study of potential biomarkers of Plasmodium falciparum malaria severity and complications. Infection, Genetics and Evolution, 77, 104046. |
| [24] | Storm, J., & Craig, A. G. (2014). Pathogenesis of cerebral malaria—inflammation and cytoadherence. Frontiers in cellular and infection microbiology, 4, 100. |
| [25] | Fang, Y., et al. (2018). The role of biomarkers of endothelial activation in predicting morbidity and mortality in patients with severe sepsis and septic shock in intensive care: a prospective observational study. Thrombosis research, 171, 149-154. |
APA Style
Boadi, E., Annani-Akollor, M. E., Nkrumah, C., Paintsil, E. K., Eshun, A. E., et al. (2026). Haematologic and Biochemical Parameters to Differentiate Severe Malaria from Uncomplicated Malaria in a Ghanaian Population in Sub-Saharan Africa. American Journal of Laboratory Medicine, 11(1), 1-8. https://doi.org/10.11648/j.ajlm.20261101.11
ACS Style
Boadi, E.; Annani-Akollor, M. E.; Nkrumah, C.; Paintsil, E. K.; Eshun, A. E., et al. Haematologic and Biochemical Parameters to Differentiate Severe Malaria from Uncomplicated Malaria in a Ghanaian Population in Sub-Saharan Africa. Am. J. Lab. Med. 2026, 11(1), 1-8. doi: 10.11648/j.ajlm.20261101.11
AMA Style
Boadi E, Annani-Akollor ME, Nkrumah C, Paintsil EK, Eshun AE, et al. Haematologic and Biochemical Parameters to Differentiate Severe Malaria from Uncomplicated Malaria in a Ghanaian Population in Sub-Saharan Africa. Am J Lab Med. 2026;11(1):1-8. doi: 10.11648/j.ajlm.20261101.11
@article{10.11648/j.ajlm.20261101.11,
author = {Enoch Boadi and Max Efui Annani-Akollor and Christopher Nkrumah and Ellis Kobina Paintsil and Anthony Eric Eshun and Lydia Omari and Yaw Frimpong and Egote Alexander Kofi},
title = {Haematologic and Biochemical Parameters to Differentiate Severe Malaria from Uncomplicated Malaria in a Ghanaian Population in Sub-Saharan Africa},
journal = {American Journal of Laboratory Medicine},
volume = {11},
number = {1},
pages = {1-8},
doi = {10.11648/j.ajlm.20261101.11},
url = {https://doi.org/10.11648/j.ajlm.20261101.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20261101.11},
abstract = {Malaria is classified as either uncomplicated (UM) or severe (SM), but the mechanism underlying the progression from uncomplicated to severe is still unclear. This study aimed to assess haematologic and biochemical parameters as potential prognostic biomarkers for differentiating SM from UM in a Ghanaian population. A descriptive cross-sectional study was conducted to sample 166 participants, comprising 42 healthy controls, 78 uncomplicated malaria cases, and 46 severe malaria cases. Blood samples were analysed for full blood count, liver function test, renal function test, and serum angiopoietins. Statistical analyses were carried out using GraphPad Prism 9 software. Median and interquartile ranges, Mann-Whitney U test, and Kruskal-Wallis analysis were done to compare groups. The haemoglobin and platelet counts of SM patients were significantly lower than those of the UM group (p < 0.05). However, the White Blood Cell (WBC) counts of severe malaria patients (7.4, IQR: 5.4 - 10.6) were significantly higher than the uncomplicated malaria population (5.7, IQR: 5.0 - 6.5) (p < 0.001). Serum levels of bilirubin (total and direct), alanine transaminase (ALT), aspartate transaminase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), and total proteins in severe malaria were significantly higher than uncomplicated malaria group (p < 0.001). These findings indicate that haemoglobin, platelet, creatinine, urea, AST, ALT, GGT and bilirubin levels may serve as biomarkers for distinguishing severe from uncomplicated malaria.},
year = {2026}
}
TY - JOUR T1 - Haematologic and Biochemical Parameters to Differentiate Severe Malaria from Uncomplicated Malaria in a Ghanaian Population in Sub-Saharan Africa AU - Enoch Boadi AU - Max Efui Annani-Akollor AU - Christopher Nkrumah AU - Ellis Kobina Paintsil AU - Anthony Eric Eshun AU - Lydia Omari AU - Yaw Frimpong AU - Egote Alexander Kofi Y1 - 2026/01/16 PY - 2026 N1 - https://doi.org/10.11648/j.ajlm.20261101.11 DO - 10.11648/j.ajlm.20261101.11 T2 - American Journal of Laboratory Medicine JF - American Journal of Laboratory Medicine JO - American Journal of Laboratory Medicine SP - 1 EP - 8 PB - Science Publishing Group SN - 2575-386X UR - https://doi.org/10.11648/j.ajlm.20261101.11 AB - Malaria is classified as either uncomplicated (UM) or severe (SM), but the mechanism underlying the progression from uncomplicated to severe is still unclear. This study aimed to assess haematologic and biochemical parameters as potential prognostic biomarkers for differentiating SM from UM in a Ghanaian population. A descriptive cross-sectional study was conducted to sample 166 participants, comprising 42 healthy controls, 78 uncomplicated malaria cases, and 46 severe malaria cases. Blood samples were analysed for full blood count, liver function test, renal function test, and serum angiopoietins. Statistical analyses were carried out using GraphPad Prism 9 software. Median and interquartile ranges, Mann-Whitney U test, and Kruskal-Wallis analysis were done to compare groups. The haemoglobin and platelet counts of SM patients were significantly lower than those of the UM group (p < 0.05). However, the White Blood Cell (WBC) counts of severe malaria patients (7.4, IQR: 5.4 - 10.6) were significantly higher than the uncomplicated malaria population (5.7, IQR: 5.0 - 6.5) (p < 0.001). Serum levels of bilirubin (total and direct), alanine transaminase (ALT), aspartate transaminase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), and total proteins in severe malaria were significantly higher than uncomplicated malaria group (p < 0.001). These findings indicate that haemoglobin, platelet, creatinine, urea, AST, ALT, GGT and bilirubin levels may serve as biomarkers for distinguishing severe from uncomplicated malaria. VL - 11 IS - 1 ER -
Laboratory Department, Bremang Seventh-Day Adventist Hospital, Kumasi, Ghana;Department of Medical Laboratory Science, Miezah University College, Kumasi, Ghana
Department of Molecular Medicine, School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Department of Molecular Medicine, School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana;Laboratory Department, Wenchi Methodist Hospital, Wenchi, Ghana
Laboratory Department, Kumasi Centre for Collaborative Research in Tropical Medicine (KCCR), Kumasi, Ghana;Department of Theoretical and Applied Biology, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Laboratory Department, Bremang Seventh-Day Adventist Hospital, Kumasi, Ghana
Department of Midwifery, Nursing and Midwifery Training School, Fomena, Ghana
Department of Medical Laboratory, Unilab Diagnostics Limited, Kumasi, Ghana
Department of Nursing, Miezah College of Health, Kumasi, Ghana
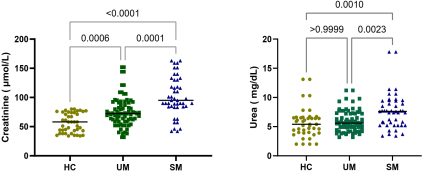
Figure 1. Comparison of serum creatinine and urea levels in malaria patients (UM and SM) and healthy controls (HC).
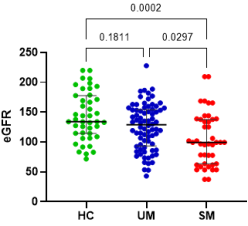
Figure 2. Comparison of eGFR levels in malaria patients (UM and SM) and healthy controls (HC).
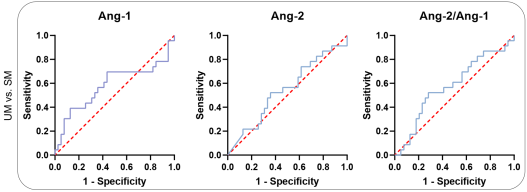
Figure 3. Assessment of angiopoietin levels in discriminating between severe malaria (SM) and uncomplicated malaria (UM).
Information

