Background: There has been a considerable increase in number of people who are diagnosed with Alcohol Dependence Syndrome (ADS). Psychiatric comorbidities are found in high proportion in association with ADS. Depressive disorders, anxiety and other psychiatric disorders are diagnosed in patients with ADS with bidirectional relationship and a high proportion of relapses are attributable to these comorbidities. Methods: A descriptive cross-sectional study was conducted over one year in the psychiatric inpatient department of Kathmandu Medical College Teaching Hospital. Sixty-one patients diagnosed with ADS based on ICD-10 DCR criteria were enrolled. Psychiatric comorbidities were assessed using the ICD -10 guidelines. Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI) scores were used to assess depressive and anxiety disorders with their severity. Results: Out of 61 patients with ADS, 78.7% had psychiatric comorbidities. Depressive disorders in (35.4%), anxiety disorders in (27.1%), psychotic disorders in (18.8%), bipolar affective disorder (10.4%), and personality disorder (8.3%) were common diagnoses made. Moderate to severe depression and anxiety were most common psychiatric comorbidities. Conclusion: Psychiatric comorbidities are highly prevalent among ADS patients. Integrated management approaches addressing both mental and physical health, along with caregiver support, are essential to improve health outcomes and reduce relapse in ADS.
| Published in | American Journal of Psychiatry and Neuroscience (Volume 13, Issue 3) |
| DOI | 10.11648/j.ajpn.20251303.13 |
| Page(s) | 89-101 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Alcohol Dependence Syndrome, Psychiatric Comorbidities, BAI, BDI, ICD-DCR
Address | Frequency | Percent |
|---|---|---|
From inside Kathmandu valley | 26 | 42.7% |
From Outside of Kathmandu Valley | 35 | 57.3% |
Diagnosis | Frequency | Valid Percent |
|---|---|---|
ADS in Uncomplicated Withdrawal | 28 | 45.9% |
ADS in Complicated Withdrawal | 33 | 54.1% |
Medical comorbidities | Frequency | Percent |
|---|---|---|
Present | 49 | 80.3 |
Absent | 12 | 19.7 |
Total | 61 | 100.0 |
Physical comorbidities | Frequency |
|---|---|
Fatty liver | 34 (55.74%) |
Mild hepatomegaly | 12 (19.67%) |
Diabetes | 8 (13.11%) |
HTN | 18 (29.50%) |
Cholelithiasis | 2 (3.28%) |
Characteristics | Category | Prevalence of Psychiatric comorbidities | Total | P-value | |
|---|---|---|---|---|---|
Present | Absent | ||||
Sex | Male | 45 | 13 | 58 | 0.481 |
Female | 3 | 0 | 3 | ||
Address | From Kathmandu | 19 | 7 | 26 | 0.271 |
From Outside Kathmandu Valley | 29 | 6 | 35 | ||
Religion | Hindu | 41 | 11 | 52 | 0.620 |
Buddhist | 7 | 2 | 9 | ||
Education | Under SLC | 23 | 4 | 27 | 0.216 |
SLC and Above SLC | 25 | 9 | 34 | ||
Family Type* | Nuclear | 26 | 11 | 37 | 0.043* |
Joint | 22 | 2 | 24 | ||
Diagnosis | Uncomplicated withdrawal | 21 | 7 | 28 | 0.368 |
ADS in complicated withdrawal | 27 | 6 | 33 | ||
Medical comorbidities* | Present | 42 | 7 | 49 | 0.014* |
Absent | 6 | 6 | 12 | ||
Characteristics | Category | Prevalence of Medical comorbidities | Total | P-value | |
|---|---|---|---|---|---|
Present | Absent | ||||
Sex | Male | 46 | 13 | 58 | 0.512 |
Female | 3 | 0 | 3 | ||
Address | From Kathmandu | 20 | 6 | 26 | 0.398 |
From Outside Kathmandu Valley | 29 | 6 | 35 | ||
Religion | Hindu | 40 | 12 | 52 | 0.118 |
Buddhist | 8 | 1 | 9 | ||
Education | Under SLC | 20 | 7 | 27 | 0.220 |
SLC and Above SLC | 29 | 5 | 34 | ||
Family Type | Nuclear | 29 | 8 | 37 | 0.448 |
Joint | 20 | 4 | 24 | ||
Diagnosis | Uncomplicated withdrawal | 22 | 6 | 28 | 0.500 |
ADS in complicated withdrawal | 27 | 6 | 33 | ||
Presence of Anxiety | Present | 12 | 1 | 13 | 0.209 |
Absent | 37 | 11 | 48 | ||
Presence of Depression | Present | 15 | 2 | 17 | 0.281 |
Absent | 34 | 10 | 44 | ||
Characteristics | Category | Diagnosis of the patients (withdrawal state) | Total | P-value | |
|---|---|---|---|---|---|
Uncomplicated | Complicated | ||||
Sex | Male | 27 | 31 | 58 | 0.562 |
Female | 1 | 2 | 3 | ||
Address* | From Kathmandu | 16 | 10 | 26 | 0.032* |
From Outside Kathmandu Valley | 12 | 23 | 35 | ||
Religion | Hindu | 23 | 29 | 52 | 0.393 |
Buddhist | 5 | 4 | 9 | ||
Education* | Under SLC | 8 | 19 | 27 | 0.021* |
SLC and Above SLC | 20 | 14 | 34 | ||
Family Type | Nuclear | 17 | 20 | 37 | 0.601 |
Joint | 11 | 13 | 24 | ||
Presence of Anxiety* | Present | 10 | 5 | 15 | 0.059* |
Absent | 18 | 28 | 46 | ||
Presence of Depression | Present | 8 | 5 | 13 | 0.168 |
Absent | 20 | 28 | 48 | ||
Medical comorbidities | Present | 22 | 27 | 49 | 0.500 |
Absent | 6 | 6 | 12 | ||
Psychiatric comorbidities | Present | 21 | 27 | 48 | 0.368 |
Absent | 7 | 6 | 13 | ||
ADS | Alcohol Dependence Syndrome |
BDI | Beck Depression Inventory |
BAI | Beck Anxiety Inventory |
| [1] | Feinstein A. The pre-therapeutic classification of co-morbidity in chronic disease. Journal of Chronic Diseases. 1970; 23(7): 455-468. |
| [2] | Wittchen H, Perkonigg A, Reed V. Comorbidity of Mental Disorders and Substance Use Disorders. European Addiction Research. 1996; 2(1): 36-47. |
| [3] | Johnson JG, Spitzer RL, Williams JBW, Kroenke K, Linzer M, et al. Psychiatric Comorbidity, Health Status, and Functional Impairment Associated With Alcohol Abuse and Dependence in Primary Care Patients: Findings of the Prime MD-1000 Study. Journal of Consulting and Clinical Psychology. 1995; 63(1): 133-40. |
| [4] | Goodwin DW, Gabrielli WF. Alcohol: Clinical Aspects. In: Lowinson JH, Ruiz P, Millman RB, Langrod JG editor. Substance Abuse, 3rd Edition, Williams and Wilkins, 1997; 142-8. |
| [5] | Gururaj G, Girish N, Benegal V. Burden and socio-economic impact of Alcohol- The Bangalore Study, Alcohol control series-1. WHO Regional office for South East Asia; 2006. |
| [6] | World Health Organization. WHO Global Status Report on Alcohol, Country profile, South-East Asian Region, Nepal. 2004: 79-94. |
| [7] | Sher L. Depression and alcoholism. QJM. 2004; 97(4): 237-240. |
| [8] | Sachdeva A, Choudhary M, Chandra M. Alcohol withdrawal syndrome: Benzodiazepines and beyond. Journal of clinical and diagnostic research: Journal of Clinical and Diagnostic Research. 2015; 9(9): VE01. |
| [9] | WHO: International Classification of disease and related Health problems, Tenth revision: Clinical description and diagnostic guideline; Geneva. World Health Organization. 1992. |
| [10] | World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders Diagnostic Criteria for Research. WHO. Geneva; 1993. |
| [11] | World Health Organization. Global report in Alcohol. Geneva. 1999. |
| [12] | Winokur G, Black DW, Nasrallah A. Depressions secondary to other psychiatric disorders and medical illnesses. The American journal of psychiatry. 1988 1; 145(2): 233. |
| [13] | Helzer JE, Pryzbeck TR. The co-occurrence of alcoholism with other psychiatric disorders in the general population and its impact on treatment. Journal of Studies on Alcohol 1988; 49(3): 219-24. |
| [14] | Gilder DA, Lau P, Gross A, Ehlers CL. Morbidity of Alcohol Dependence with Other Psychiatric Disorders in Young Adult Mexican Americans. Journal of Addictive Disease. 2007; 26(10): 31-40. |
| [15] | Farrell M, Howes S, Bebbington P, BrughaT, Jenkins R, et al. Nicotine, alcohol and drug dependence and psychiatric co morbidity-Results of a national household survey. British Journal of Psychiatry 2001; 179: 432-7. |
| [16] | Schuckit MA. The clinical implications of primary diagnostic groups among alcoholics. Archieves of General Psychiatry. 1985; 42: 1043-9. |
| [17] | Clark RE, Drake RE. Expenditures of time and money by families of people whit several mental illness and substance use disorders. Community Mental Health Journal. 1994; 30: 145-63. |
| [18] | Duke PJ, Pantelis C, Barnes TR. South Westminster schizophrenia survey. Alcohol use and its relationship to symptoms, tardive dyskinesia and illness onset. The British Journal of Psychiatry. 1994; 164(5): 630-6. |
| [19] | Yesavage JA, Zarcone V. History of drug abuse and dangerous behavior in inpatient schizophrenics. Journal of Clinical Psychiatry 1983; 44: 259-61. |
| [20] | Sher KJ, Trull TJ. Personality and disinhibitory psychopathology: alcoholism and antisocial personality disorder. Journal of abnormal psychology. 1994; 103(1): 92. |
| [21] | McGue M, Slutske W, Taylor J, Lacono WG. Personality and substance use disorders: I. Effects of gender and alcoholism subtype. Alcoholism: Clinical and Experimental Research. 1997; 21(3): 513-20. |
| [22] | Babor TF, Hofmann M, DelBoca FK, Hesselbrock V, Meyer RE, Dolinsky ZS, Rounsaville B. Types of alcoholics, I: evidence for an empirically derived typology based on indicators of vulnerability and severity. Archives of general Psychiatry. 1992; 49(8): 599-608. |
| [23] | Vanderplasschen WOI, Colpaert KAG, Broekaert EKM. Determinants of relapse and readmission among alcohol abusers after intensive residential treatment. Arch Public Health 2009; 67: 194-211. |
| [24] | Verheul R. Co-morbidity of personality disorders in individuals with substance use disorders. European Psychiatry. 2001; 16(5): 274-82. |
| [25] | Haynes JC, Farrell M, Singleton N, Meltzer H Araya R, Lewis G, et al. Alcohol consumption as a risk factor for anxiety and depression. British Journal of Psychiatry. 2005; 187: 544-51. |
| [26] | Sabourin B, Stewart S. Alcohol Use and Anxiety Disorders. Anxiety in Health Behaviors and Physical Illness. 2008; 29-54. |
| [27] | Bibb J, Chambless D. Alcohol use and abuse among diagnosed agoraphobics. Behaviour Research and Therapy. 1986; 24(1): 49-58. |
| [28] | Cappell H, Herman CP. Alcohol and tension reduction: A review. Journal of Studies on Alcohol. 1972; 33: 33-64. |
| [29] | Hasin D, Grant B. Major Depression in 6050 Former Drinkers. Archives of General Psychiatry. 2002; 59(9): 794. |
| [30] | Kessler R. Lifetime Co-occurrence of DSM-III-R Alcohol Abuse and Dependence with Other Psychiatric Disorders in the National Comorbidity Survey. Arch Gen Psychiatry. 1997; 54(4): 313. |
| [31] | Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990; 264(19): 2511-8. |
| [32] | Dixon L, Haas G, Weiden P, and Sweeney J, Frances A. Acute effects of drug abuse in schizophrenic patients: clinical observations and patients' self-report. Schizophrenia Bulletin. 1990; 16(1): 69. |
| [33] | Cuffel BJ, Chase P. Remission and Relapse of Substance Use Disorders in Schizophrenia Results from a One-Year Prospective Study. The Journal of nervous and mental disease. 1994; 182(6): 342-8. |
| [34] | Sonne SC, Brady KT. Bipolar disorder and alcoholism. Alcohol Research & Health. 2002; 26(2): 103-9. |
| [35] | Schoepf D, Heun R. Alcohol dependence and physical comorbidity: Increased prevalence but reduced relevance of individual comorbidities for hospital-based mortality during a 12.5-year observation period in general hospital admissions in urban North-West England. Eur Psychiatry. 2015; 30(4): 459-68. |
| [36] | World Health Organization. Global Status Report on Alcohol and health. 2014. |
| [37] | Grant B. F, Dufour M. C, Harford T. C. Epidemiology of alcoholic liver disease. Seminars in Liver Disease. 1988; 8(1): 12-25. |
| [38] | Urbano-Marquez A, Estruch R, Navarro-Lopez F, Grau JM, Mont L, Rubin E. The effects of alcoholism on skeletal and cardiac muscle. New England Journal of Medicine. 1989; 320(7): 409-15. |
| [39] | Berman, M. O. Severe brain dysfunction: Alcoholic Korsakoff's syndrome. Alcohol Health & Research World. 1990; 14(2): 120-129. |
| [40] | Lieber C. S, Garro A. J, Leo M. A, Worner T. M. Mechanisms for the interrelationship between alcohol and cancer. Alcohol Health & Research World. 1986; 10(3): 10-17, 48-50. |
| [41] | Szabo G, Mandrekar P. A recent perspective on alcohol, immunity, and host defense. Alcoholism: Clinical and Experimental Research. 2009; 33(2): 220-32. |
| [42] | Kelleher M. Drugs and alcohol: physical complications. Psychiatry. 2006; 5(12): 442-445. |
| [43] | Woody G, McLellan A, Bedrick J. Comorbidade - um desafio no tratamento de dependência de drogas. R Psiquiatr RS. 1995; 17(3): 189-200. |
| [44] | Dhital R, Subedi G, Gurung Y. B, Hamal P. Alcohol and Drug Use in Nepal with Reference to Children. Kathmandu: Child Workers in Nepal Concerned Centre (CWIN). 2001. |
| [45] | ShakyaDhana R, ShyangwaPramod M, Sen B. Psychiatric Comorbidity in Cases Admitted for Alcohol Dependence. Delhi Psychiatry Journal. 2009; 12(2): 252-257. |
| [46] | Shakya DR, Shyangwa PM, Sen B. Physical Diseases in Cases Admitted for Alcohol Dependence. Health Renaissance Journal. 2008; 5(1): 27-31. |
| [47] | Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of general psychiatry. 1961; 4(6): 561-71. |
| [48] | Beck AT, Steer RA, Ball R, Ranieri WF. Comparison of Beck Depression Inventories-IA and-II in psychiatric outpatients. Journal of personality assessment. 1996; 67(3): 588-97. |
| [49] | Kohrt BA, Kunz RD, Koirala NR, Sharma VD, Nepal MK. Validation of a Nepali version of the Beck Depression Inventory. Nepalese Journal of Psychiatry. 2002; 2(4): 123-30. |
| [50] | Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clinical psychology review. 1988; 8(1): 77-100. |
| [51] | Petrakis I, Gonzalez G, Rosenheck R, Krystal J. Comorbidity of alcoholism and psychiatric disorders. An overview. |
| [52] | Risal A, Tharoor H. A cross-sectional comparison of drinking patterns, alcohol use and relate medical morbidities in a secondary versus tertiary setting. Kathmandu University Medical Journal. 2013; 11(42): 152-7. |
| [53] | Kumar Vivek, Dalal Pronab K, Trivedi Jitendra K, Kumar Pankaj. A Study of Psychiatric Comorbidity in Alcohol Dependence. Delhi Psychiatry Journal. 2010; 13(2): 291-293. |
| [54] | Pradhan S, Adhikary S, Sharma S. A prospective study of comorbidity of alcohol and depression. Kathmandu University Medical Journal. 2009; 6(3): 340-345. |
| [55] |
Npal-Census-2011-Vol 1.
https://nepal.unfpa.org/en/publications/national-population-and-housing-census-2011le |
| [56] | Chandini S, Mathai P. Prevalence of medical comorbidity in alcohol dependence syndrome. Muller Journal of Medical Sciences and Research. 2013; 4(2): 68-73. |
| [57] | Sedhain CP. Study of psychiatric comorbidity of alcohol use disorder. Nepal Health Research Counc J. 2013; 11(1): 66-69. |
| [58] | Abhay Singh, Santosh Kumar, Chandra Shekhar Sharma, Vidhata Dixit, Rohit Kant Srivastava, RakeshYaduvanshi. Other psychiatric comorbidities in male patients of alcohol dependence syndrome: A cross sectional study. Indian Journal of Basic and Applied Medical Research; 2016; 5(2): 828-838. |
| [59] | Vohra AK, Yadav BS, Khurana H. A study of psychiatric comorbidity in-alcohol dependence. Indian journal of psychiatry. 2003; 45(4): 247-250. |
| [60] | Anthenelli RM, Schuckit MA. Affective and anxiety disorders and alcohol and drug dependence: diagnosis and treatment. Journal of Addictive Diseases. 1993; 12(3): 73-87. |
| [61] | Kessler R, Nelson C, McGonagle K, Edlund M, Frank R, Leaf P. The epidemiology of co-occurring addictive and mental disorders: Implications for prevention and service utilization. American Journal of Orthopsychiatry. 1996; 66(1): 17-31. |
| [62] | Schneider U, Altmann A, Baumann M, Bernzen J, Bertz B, Bimber U, et al. Comorbid anxiety and affective disorder in alcohol-dependent patients seeking treatment: the first Multicentre Study in Germany. Alcohol and alcoholism. 2001; 36(3): 219-23. |
| [63] | Kattimani S, Balaji Bharadwaj S, Vikas Menon S. Medical Comorbidities in Patients with Alcohol Dependence, “Does Nicotine Matter?’’ International Journal of Emergency Mental Health and Human Resilience. 2015; 17: 3616-617. |
| [64] | Kaur D, Ajinkya S. Psychological impact of adult alcoholism on spouses and children. Medical Journal of Dr DY Patil University. 2014; 7(2): 124. |
| [65] | Dr. S. Thasnim Begam, Dr. R. Gandhi Babu, Dr. M. Asok Kumar, Dr. S. Arun. Psychiatric Morbidity in Spouses of Patients with Alcohol Dependence Syndrome. International Journal of Modern Research and Reviews. 2015; 3(10): 876-881. |
| [66] | Gohil J, Patel M, Samani M. Quality of Life and Psychiatric Morbidity in Caregiver of Alcohol Dependence Patients. IOSR Journal of Dental and Medical Sciences. 2016; 15(08): 98-101. |
APA Style
Samadarshi, S., Pradhan, S. N., Khanal, A. (2025). Study of Psychiatric Comorbidities in Patients Diagnosed with Alcohol Dependence Syndrome in Kathmandu Medical College. American Journal of Psychiatry and Neuroscience, 13(3), 89-101. https://doi.org/10.11648/j.ajpn.20251303.13
ACS Style
Samadarshi, S.; Pradhan, S. N.; Khanal, A. Study of Psychiatric Comorbidities in Patients Diagnosed with Alcohol Dependence Syndrome in Kathmandu Medical College. Am. J. Psychiatry Neurosci. 2025, 13(3), 89-101. doi: 10.11648/j.ajpn.20251303.13
@article{10.11648/j.ajpn.20251303.13,
author = {Sushil Samadarshi and Sudarshan Narsing Pradhan and Asmita Khanal},
title = {Study of Psychiatric Comorbidities in Patients Diagnosed with Alcohol Dependence Syndrome in Kathmandu Medical College
},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {13},
number = {3},
pages = {89-101},
doi = {10.11648/j.ajpn.20251303.13},
url = {https://doi.org/10.11648/j.ajpn.20251303.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20251303.13},
abstract = {Background: There has been a considerable increase in number of people who are diagnosed with Alcohol Dependence Syndrome (ADS). Psychiatric comorbidities are found in high proportion in association with ADS. Depressive disorders, anxiety and other psychiatric disorders are diagnosed in patients with ADS with bidirectional relationship and a high proportion of relapses are attributable to these comorbidities. Methods: A descriptive cross-sectional study was conducted over one year in the psychiatric inpatient department of Kathmandu Medical College Teaching Hospital. Sixty-one patients diagnosed with ADS based on ICD-10 DCR criteria were enrolled. Psychiatric comorbidities were assessed using the ICD -10 guidelines. Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI) scores were used to assess depressive and anxiety disorders with their severity. Results: Out of 61 patients with ADS, 78.7% had psychiatric comorbidities. Depressive disorders in (35.4%), anxiety disorders in (27.1%), psychotic disorders in (18.8%), bipolar affective disorder (10.4%), and personality disorder (8.3%) were common diagnoses made. Moderate to severe depression and anxiety were most common psychiatric comorbidities. Conclusion: Psychiatric comorbidities are highly prevalent among ADS patients. Integrated management approaches addressing both mental and physical health, along with caregiver support, are essential to improve health outcomes and reduce relapse in ADS.},
year = {2025}
}
TY - JOUR T1 - Study of Psychiatric Comorbidities in Patients Diagnosed with Alcohol Dependence Syndrome in Kathmandu Medical College AU - Sushil Samadarshi AU - Sudarshan Narsing Pradhan AU - Asmita Khanal Y1 - 2025/08/26 PY - 2025 N1 - https://doi.org/10.11648/j.ajpn.20251303.13 DO - 10.11648/j.ajpn.20251303.13 T2 - American Journal of Psychiatry and Neuroscience JF - American Journal of Psychiatry and Neuroscience JO - American Journal of Psychiatry and Neuroscience SP - 89 EP - 101 PB - Science Publishing Group SN - 2330-426X UR - https://doi.org/10.11648/j.ajpn.20251303.13 AB - Background: There has been a considerable increase in number of people who are diagnosed with Alcohol Dependence Syndrome (ADS). Psychiatric comorbidities are found in high proportion in association with ADS. Depressive disorders, anxiety and other psychiatric disorders are diagnosed in patients with ADS with bidirectional relationship and a high proportion of relapses are attributable to these comorbidities. Methods: A descriptive cross-sectional study was conducted over one year in the psychiatric inpatient department of Kathmandu Medical College Teaching Hospital. Sixty-one patients diagnosed with ADS based on ICD-10 DCR criteria were enrolled. Psychiatric comorbidities were assessed using the ICD -10 guidelines. Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI) scores were used to assess depressive and anxiety disorders with their severity. Results: Out of 61 patients with ADS, 78.7% had psychiatric comorbidities. Depressive disorders in (35.4%), anxiety disorders in (27.1%), psychotic disorders in (18.8%), bipolar affective disorder (10.4%), and personality disorder (8.3%) were common diagnoses made. Moderate to severe depression and anxiety were most common psychiatric comorbidities. Conclusion: Psychiatric comorbidities are highly prevalent among ADS patients. Integrated management approaches addressing both mental and physical health, along with caregiver support, are essential to improve health outcomes and reduce relapse in ADS. VL - 13 IS - 3 ER -
Department of Public Health, Manmohan Memorial Institute of Health Science, Tribhuvan University, Kathmandu, Nepal
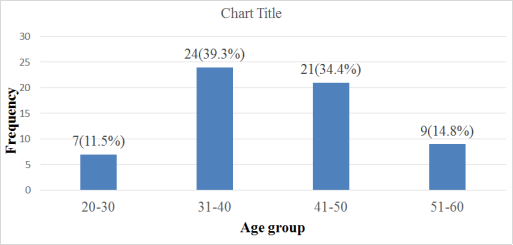
Figure 1. Distribution of patients according to age (N=61).
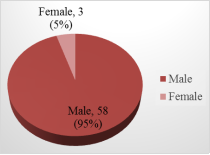
Figure 2. Distribution of patients according to sex (N=61).
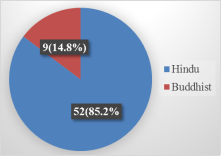
Figure 3. Distribution of patients according to the religion (N=61).
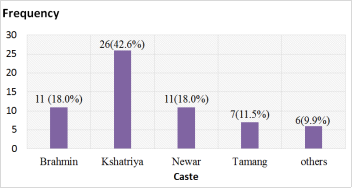
Figure 4. Distribution of patients according to the Caste (N=61).
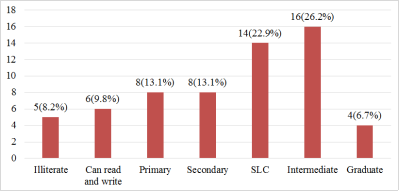
Figure 5. Distribution according to the Education (N=61).
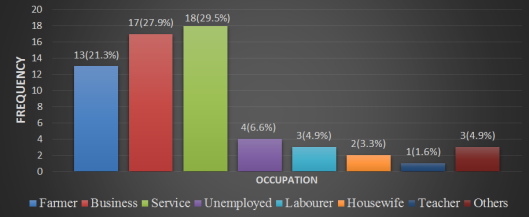
Figure 6. Distribution of patients according to Occupation (N=61).
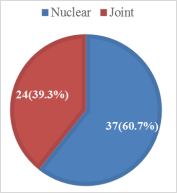
Figure 7. Distribution of patients according to type of Family (N=61).
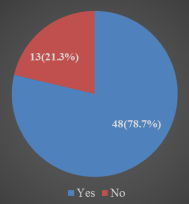
Figure 8. Distribution of patients according to the presence of Psychiatric comorbidities (N=61).
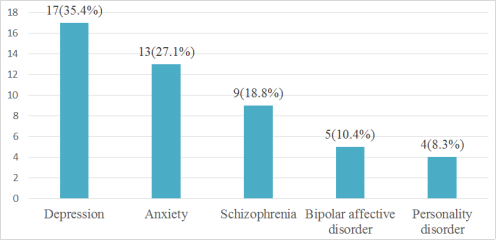
Figure 9. Distribution of Patients according to classification of Psychiatric comorbidities (N=48).
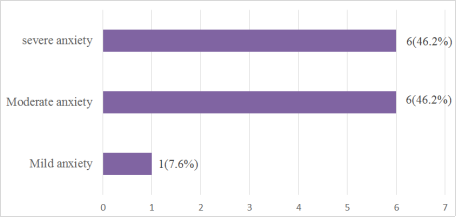
Figure 10. Distribution of patients according to the severity of anxiety (N=13).
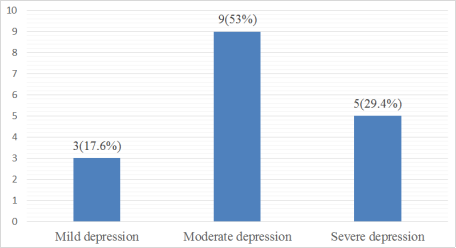
Figure 11. Distribution of patients according to severity of depression (N=17).
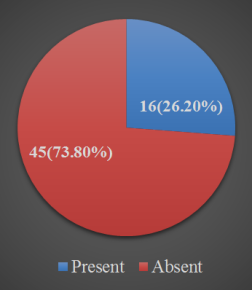
Figure 12. Distribution according to presence of anxiety in caretaker (N=61).
Information

