Accurate detection and confirmation of malaria parasites require good-quality microscopy. Low-quality microscopy can result in incorrect diagnoses and, hence, ineffective treatments. Several factors, including the skills of laboratory personnel, influence the quality of malaria microscopy, posing challenges in malaria diagnosis. The present study assessed the competence of medical laboratory practitioners in malaria microscopy and associated factors in selected health facilities in Moshi Municipality, Tanzania. A cross-sectional study was conducted from May to June 2024, where 147 laboratory practitioners from 45 health facilities in Moshi Municipality were included in the study. Six standardized External Quality Assessment malaria slides were distributed to each health facility. Individual laboratory practitioners in each facility had a choice to read only one of the slides. The competence of laboratory practitioners in malaria microscopy in this study was measured by the accuracy of detection and quantification of malaria parasites. Multiple logistic regression was performed to determine factors associated with good performance in malaria microscopy, where the odds ratio (OR) and corresponding 95% confidence interval were reported. All variables with p-values <0.05 were considered significant. A total of 147 laboratory practitioners participated, and the accuracy of malaria parasite detection and quantification was 46.2% and 36%, respectively. Malaria microscopy training showed an association with the accuracy of malaria slide reading with COR=3.437 (CI=1.681-7.031), p-value=0.001, AOR=2.669 (CI=1.217-5.855), p-value=0.014. Our study results show a low level of proficiency in malaria microscopy among laboratory practitioners in Moshi Municipality. Our study results show a low level of proficiency in malaria microscopy among laboratory practitioners in Moshi Municipality. Refresher training in malaria microscopy could improve the performance of the laboratory practitioners for the detection and quantification of malaria parasites.
| Published in | Biomedical Sciences (Volume 11, Issue 1) |
| DOI | 10.11648/j.bs.20251101.12 |
| Page(s) | 15-23 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
External Quality Assessment, Malaria, Malaria Microscopy, Competence, Laboratory Practitioners, Moshi Municipality, Tanzania
Variable | Frequency | Percentage |
|---|---|---|
Age | 30.9 (6.90) | |
18-30 years | 91 | 61.9 |
31-40 years | 38 | 25.9 |
41 years-Above | 18 | 12.2 |
Sex | ||
Male | 86 | 58.5 |
Female | 61 | 41.5 |
Facility level | ||
Dispensary | 42 | 28.6 |
Health center | 37 | 25.2 |
Polyclinic | 23 | 15.6 |
Private laboratory | 8 | 5.4 |
Hospital | 37 | 25.2 |
Education level | ||
Certificate | 31 | 21.1 |
Diploma | 83 | 56.5 |
Advanced diploma | 4 | 2.7 |
Bachelor | 29 | 19.7 |
Practitioners slide report | EQA slide stats | Total | |
|---|---|---|---|
EQA slides with parasites | EQA slides with no parasites | ||
Detected | 45 | 23 | 68 |
Not detected | 36 | 43 | 79 |
Total | 81 | 66 | 147 |
Quantified | 30 | 23 | 53 |
Not quantified | 50 | 44 | 94 |
Total | 80 | 67 | 147 |
Variable | N | Accurate n (%) | COR (95% C.I) | p-value | AOR (95% CI) | p-value |
|---|---|---|---|---|---|---|
Age | ||||||
18-30 years | 91 | 37 (40.7) | 0.475 (0.141-1.599) | 0.229 | ||
31-40 years | 38 | 21 (55.3) | 0.264 (0.087-0.802) | 0.019 | ||
41 years-Above | 18 | 23 (72.2) | 1 | |||
Sex | ||||||
Male | 86 | 42 (48.8) | 1.053 (0.546-2.031) | 0.877 | ||
Female | 61 | 29 (47.5) | 1 | |||
Facility level | ||||||
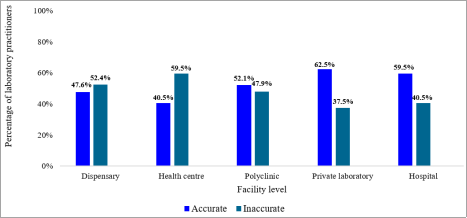
Dispensary | 42 | 20 (47.6) | 1.270 (0.264-6.117) | 0.766 | ||
Health center | 37 | 15 (40.5) | 0.990 (0.347-2.831) | 0.986 | ||
Polyclinic | 23 | 12 (52.1) | 0.413 (0.162-1.054) | 0.064 | ||
Private laboratory | 8 | 5 (62.5) | 0.629 (0.258-1.533) | 0.308 | ||
Hospital | 37 | 22 (59.5) | 1 | |||
Level of education | ||||||
Certificate | 31 | 12 (38.7) | 0.933 (0.115-7.553) | 0.948 | ||
Diploma | 83 | 42 (50.6) | 0.956 (0.410-2.228) | 0.917 | ||
Advanced diploma | 4 | 2 (50) | 0.589 (0.211-1.645) | 0.313 | ||
Bachelor | 29 | 15 (51.7) | 1 | |||
HLPC registration | ||||||
Yes | 118 | 64 (54.2) | 3.725 (1.78-9.388) | 0.005 | ||
No | 29 | 7 (24.1) | 1 | |||
Working duration | ||||||
1 to 5 years | 105 | 45 (42.9) | 0.181 (0.020-1.636) | 0.128 | ||
5 to 10 years | 34 | 19 (55.9) | 0.107 (0.013-0.902) | 0.04 | ||
10-More | 8 | 7 (87.5) | 1 | |||
Malaria microscopy training | ||||||
Yes | 93 | 55 (59.1) | 3.437 (1.681-7.031) | 0.001 | 2.669 (1.217-5.855) | 0.014 |
No | 84 | 16 (29.6) | 1 | |||
EQA enrolment | ||||||
Yes | 66 | 39 (59.1) | 2.212 (1.140-4.291) | 0.019 | ||
No | 81 | 32 (39.5) | 1 | |||
IQC programme | ||||||
Yes | 78 | 41 (52.6) | 1.441 (0.751-2.763) | 0.272 | ||
No | 69 | 30 (43.5) | 1 | |||
Awareness of national guidelines for malaria diagnosis | ||||||
Yes | 118 | 66 (55.6) | 6.092 (2.175-17.061) | 0.001 | ||
No | 29 | 5 (17.2) | 1 | |||
AIDS | Acquired Immunodeficiency Syndrome |
AOR | Adjusted Odds Ratio |
COR | Crude Odds Ratio |
DLT | District Laboratory Technician |
EQA | External Quality Assessment |
HIV | Human Immunodeficiency Virus |
HLPC | Health Laboratory Practitioners Council |
IQA | Internal Quality Assessment |
KCMUCo | Kilimanjaro Christian Medical University College |
mRDT | malaria Rapid Diagnostic Test |
NMCP | National Malaria Control Program |
QA | Quality Assessment |
SPSS | Statistical Package for the Social Sciences |
WHO | World Health Organization |
| [1] |
CDC. Malaria - Diagnosis & Treatment (United States) - Diagnosis, 2023.
https://www.cdc.gov/malaria/diagnosis_treatment/diagnostic_tools.html (accessed 3.21.24). |
| [2] |
WHO. WHO consolidated Guidelines for malaria Geneva: World Health Organization; 2023 [WWW Document]. URL
https://www.who.int/teams/global-malaria-programme/guidelines-for-malaria (accessed 3.6.24). |
| [3] | World Malaria Report 2022. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO. |
| [4] | WHO World Malaria Report 2020. Geneva: World Health Organization; 2020. Licence: CC BY-NC-SA 3.0 IGO. |
| [5] | National guidelines for malaria diagnosis, treatment and preventive therapies, 2020. |
| [6] | WHO. Malaria Light Microscopy. Creating a Culture of Quality. Report of WHO SEARO/WPRO workshop on quality assurance for malaria microscopy, Kuala Lumpur, Malaysia. 2005. |
| [7] | Maguire, J. D., Lederman, E. R., Barcus, M. J., O'Meara, W., Jordon, R. G., Duong, S., Muth, S., Sismadi, P., Bangs, M. J, Prescott, W. R, Baird, J. K., and Wongsrichanalai, C. Production and validation of durable, high quality standardized malaria microscopy slides for teaching, testing and quality assurance during an era of declining diagnostic proficiency. Malaria Journal. 2006; 5: 92. |
| [8] | Mukadi, P., Gillet, P., Lukuka, A., Atua, B., Kahodi, S., Lokombe, J., Muyembe, J., and Jacobs. J. External quality assessment of malaria microscopy in the Democratic Republic of the Congo. Malaria Journal. 2011, 10, 308. |
| [9] | Khan, M. A., Walley, J. D., Munir, M. A., Khan, M. A., Khokar, N. G., Tahir, Z., Nazir, A., and Nazia Shams N. District level external quality assurance (EQA) of malaria microscopy in Pakistan: pilot implementation and feasibility. Malaria Journal. 2011, 10, 45. |
| [10] | Zeleke, B., Admasu, G., Getachew, T., Kebede, E., Goshu Belay, G., Abraha, A., Yihdego D., Hailemariam, M., Birhaneselassie, M. External Quality Assessment of Malaria Microscopy in Hawassa Health Facilities, Southern Ethiopia. Clinical Medicine Ressearch. 2015, 4, 63. |
| [11] | Sori, G., Zewdieb, O., Tadele, G., and Samuel, A. External quality assessment of malaria microscopy diagnosis in selected health facilities in Western Oromia, Ethiopia. Malaria Journal. 2018 17: 233, |
| [12] | Kalinga, A., Mgata, S., Kavishe, R. A, Mahikwano, L., Temu, L., Mswanya, C., Mwanziva, C., Amoo, G., Kamau, E., Vesely, B., and Ishengoma, D. Implementation of external quality assessment of microscopy for improved parasite detection and confirmatory diagnosis of malaria in Tanzanian Military health facilities BMC Research Notes., 2020, 13: 447. |
| [13] | Yigezu, E., Wondale, B., Abebe, D., Tamiru, G., Eligo, N., Lindtjørn, B., Gadisa, E., Tadesse, F. G., and Fekadu Massebo, F. Malaria misdiagnosis in the routine health system in Arba Minch area district in southwest Ethiopia: an implication for malaria control and elimination. Malaria Journal. 2023, 22, 273. |
| [14] | Allen, K., Hatfield, J. M., Manyama, M. J. Reducing microscopy-based malaria misdiagnosis in a low-resource area of Tanzania Journal of Health Research, 2013, 15. |
| [15] | Harchut, K., Standley, C., Dobson, A., Klaassen, B., Rambaud-Althaus, C., Althaus, F., and Nowak, K. Over-diagnosis of malaria by microscopy in the Kilombero Valley, Southern Tanzania: an evaluation of the utility and cost-effectiveness of rapid diagnostic tests. Malaria Journal. 2013 12, 159. |
| [16] | Nankabirwa, J., Zurovac, D., Njogu, J. N., Rwakimari, J. B, Counihan, H., Snow, R. W., and Tibenderana, J. K. Malaria misdiagnosis in Uganda--implications for policy change. Malaria. Journal. 2009, 8, 66. |
| [17] | Reyburn, H., Mbatia, R., Drakeley, C., Mwerinde, O., Saganda, S., JShao, J., Kitua, A., Olomi, R., Greenwood, B. M., and Whitty, C. J. M. Over diagnosis of malaria in patients with severe febrile illness in Tanzania: a prospective study. BMJ, 2004, 329, 1212. |
| [18] | D’Acremont, V., Lengeler, C., Mshinda, H., Mtasiwa, D., Tanner, M., and Blaise Genton, B. Time to move from presumptive malaria treatment to laboratory-confirmed diagnosis and treatment in African children with fever. PLoS Medicine. 2009, 6, e252. |
| [19] | Mideo, N., Savill, N. J., Chadwick, W., Schneider P., Read A. F., Day, T., and Reece, S. E. Causes of Variation in Malaria Infection Dynamics: Insights from Theory and Data. American Naturalist. 2011, 178(6). |
| [20] | Wang, R., Tang, S., Jun Yang, J., Shao, T., Shao, P., Liu, C., Feng, D., Fu, H., Chen, X., Hu, T., and Feng, Z. Improving local health workers’ knowledge of malaria in the elimination phase-determinants and strategies: a cross-sectional study in rural China. Malaria Journal. 2017, 16. |
| [21] | Wongsrichanalai, C., Barcus, M. J., Muth, S., Sutamihardja, A., Wernsdorfer, W. H. A Review of Malaria Diagnostic Tools: Microscopy and Rapid Diagnostic Test (RDT) American Journal of Tropical Medicine and Hygiene, 2007, 77(Suppl 6), 2007, pp. 119–127. |
| [22] | WHO Malaria microscopy quality assurance manual, version 2.ed. World Health Organization, Geneva, 2016. |
| [23] | Mbakilwa, H., Manga, C., Kibona, S., Mtei, F., Meta, J., Shoo, A., Ben Amos, B., and Hugh Reyburn, H. Quality of malaria microscopy in 12 district hospital laboratories in Tanzania. Pathogens and Global Health., 2012, 106, 330–334. |
| [24] | Kahama-Maro, J., D’Acremont, V., Mtasiwa, D., Genton, B., Lengeler, C. Low quality of routine microscopy for malaria at different levels of the health system in Dar es Salaam. Malaria Journal. 2011, 10, 332. |
| [25] | Odhiambo, F., Buf, A. M., Moranga, C., Moseti, C. M., Wesongah, J. O., Lowther, S. A., Arvelo, W., Galgalo, T., Achia, O., Roka, Z. G., Boru, W., Chepkurui, L., Ogutu, B., and Elizabeth Wanja. Factors associated with malaria microscopy diagnostic performance following a pilot quality-assurance programme in health facilities in malaria low-transmission areas of Kenya, 2014. Malaria Journal. 2017 16, 371. |
| [26] | Biadglegne, F., Belyhun, Y. Fisha Walle, F., Gudeta, N., Kassu, A., and Mulu, A. Does the practice of blood film microscopy for detection and quantification of malaria parasites in northwest Ethiopia fit the standard? BMC Health Services Research. 2014 14, 529. |
| [27] | Mutabazi, T., Arinaitwe, E., Ndyabakira, A., Sendaula, E., Kakeeto, A, Okimat, P., Orishaba, P., Katongole, S. P., Mpimbaza, A., Byakika-Kibwika, P, Karamagi, C., Kalyango J. N., Moses R. Kamya. M. R., Dorsey, G., and Nankabirwa, J. I. Assessment of the accuracy of malaria microscopy in private health facilities in Entebbe Municipality, Uganda: a cross-sectional study. Malaria Journal. 2021, 250. |
| [28] | Ngasala, B., Mubi, M., Warsame, M., Petzold, M. G., Massele, A. Y., Gustafsson, L. L., Goran Tomson, G., Premji, Z., and Bjorkman, A. Impact of training in clinical and microscopy diagnosis of childhood malaria on antimalarial drug prescription and health outcome at primary health care level in Tanzania: A randomized controlled trial. Malaria Journal. 7: 199. |
APA Style
Macha, E., Mayemba, D., Ngowi, C., Rutunda, H., Kamwamwa, I., et al. (2025). Competence of Laboratory Practitioners on Malaria Microscopy and Associated Factors in Moshi Municipality, North-eastern Tanzania. Biomedical Sciences, 11(1), 15-23. https://doi.org/10.11648/j.bs.20251101.12
ACS Style
Macha, E.; Mayemba, D.; Ngowi, C.; Rutunda, H.; Kamwamwa, I., et al. Competence of Laboratory Practitioners on Malaria Microscopy and Associated Factors in Moshi Municipality, North-eastern Tanzania. Biomed. Sci. 2025, 11(1), 15-23. doi: 10.11648/j.bs.20251101.12
@article{10.11648/j.bs.20251101.12,
author = {Emmanuel Macha and Doreen Mayemba and Calvin Ngowi and Happiness Rutunda and Innocent Kamwamwa and Balthazar Nyombi and Johnson Matowo},
title = {Competence of Laboratory Practitioners on Malaria Microscopy and Associated Factors in Moshi Municipality, North-eastern Tanzania
},
journal = {Biomedical Sciences},
volume = {11},
number = {1},
pages = {15-23},
doi = {10.11648/j.bs.20251101.12},
url = {https://doi.org/10.11648/j.bs.20251101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.bs.20251101.12},
abstract = {Accurate detection and confirmation of malaria parasites require good-quality microscopy. Low-quality microscopy can result in incorrect diagnoses and, hence, ineffective treatments. Several factors, including the skills of laboratory personnel, influence the quality of malaria microscopy, posing challenges in malaria diagnosis. The present study assessed the competence of medical laboratory practitioners in malaria microscopy and associated factors in selected health facilities in Moshi Municipality, Tanzania. A cross-sectional study was conducted from May to June 2024, where 147 laboratory practitioners from 45 health facilities in Moshi Municipality were included in the study. Six standardized External Quality Assessment malaria slides were distributed to each health facility. Individual laboratory practitioners in each facility had a choice to read only one of the slides. The competence of laboratory practitioners in malaria microscopy in this study was measured by the accuracy of detection and quantification of malaria parasites. Multiple logistic regression was performed to determine factors associated with good performance in malaria microscopy, where the odds ratio (OR) and corresponding 95% confidence interval were reported. All variables with p-values <0.05 were considered significant. A total of 147 laboratory practitioners participated, and the accuracy of malaria parasite detection and quantification was 46.2% and 36%, respectively. Malaria microscopy training showed an association with the accuracy of malaria slide reading with COR=3.437 (CI=1.681-7.031), p-value=0.001, AOR=2.669 (CI=1.217-5.855), p-value=0.014. Our study results show a low level of proficiency in malaria microscopy among laboratory practitioners in Moshi Municipality. Our study results show a low level of proficiency in malaria microscopy among laboratory practitioners in Moshi Municipality. Refresher training in malaria microscopy could improve the performance of the laboratory practitioners for the detection and quantification of malaria parasites.},
year = {2025}
}
TY - JOUR T1 - Competence of Laboratory Practitioners on Malaria Microscopy and Associated Factors in Moshi Municipality, North-eastern Tanzania AU - Emmanuel Macha AU - Doreen Mayemba AU - Calvin Ngowi AU - Happiness Rutunda AU - Innocent Kamwamwa AU - Balthazar Nyombi AU - Johnson Matowo Y1 - 2025/07/30 PY - 2025 N1 - https://doi.org/10.11648/j.bs.20251101.12 DO - 10.11648/j.bs.20251101.12 T2 - Biomedical Sciences JF - Biomedical Sciences JO - Biomedical Sciences SP - 15 EP - 23 PB - Science Publishing Group SN - 2575-3932 UR - https://doi.org/10.11648/j.bs.20251101.12 AB - Accurate detection and confirmation of malaria parasites require good-quality microscopy. Low-quality microscopy can result in incorrect diagnoses and, hence, ineffective treatments. Several factors, including the skills of laboratory personnel, influence the quality of malaria microscopy, posing challenges in malaria diagnosis. The present study assessed the competence of medical laboratory practitioners in malaria microscopy and associated factors in selected health facilities in Moshi Municipality, Tanzania. A cross-sectional study was conducted from May to June 2024, where 147 laboratory practitioners from 45 health facilities in Moshi Municipality were included in the study. Six standardized External Quality Assessment malaria slides were distributed to each health facility. Individual laboratory practitioners in each facility had a choice to read only one of the slides. The competence of laboratory practitioners in malaria microscopy in this study was measured by the accuracy of detection and quantification of malaria parasites. Multiple logistic regression was performed to determine factors associated with good performance in malaria microscopy, where the odds ratio (OR) and corresponding 95% confidence interval were reported. All variables with p-values <0.05 were considered significant. A total of 147 laboratory practitioners participated, and the accuracy of malaria parasite detection and quantification was 46.2% and 36%, respectively. Malaria microscopy training showed an association with the accuracy of malaria slide reading with COR=3.437 (CI=1.681-7.031), p-value=0.001, AOR=2.669 (CI=1.217-5.855), p-value=0.014. Our study results show a low level of proficiency in malaria microscopy among laboratory practitioners in Moshi Municipality. Our study results show a low level of proficiency in malaria microscopy among laboratory practitioners in Moshi Municipality. Refresher training in malaria microscopy could improve the performance of the laboratory practitioners for the detection and quantification of malaria parasites. VL - 11 IS - 1 ER -
Department of Medical Parasitology and Entomology, Kilimanjaro Christian Medical University College, Moshi, Tanzania
Department of Medical Parasitology and Entomology, Kilimanjaro Christian Medical University College, Moshi, Tanzania
Department of Medical Parasitology and Entomology, Kilimanjaro Christian Medical University College, Moshi, Tanzania
Department of Medical Parasitology and Entomology, Kilimanjaro Christian Medical University College, Moshi, Tanzania
Quality Improvement Unit, Kilimanjaro Christian Medical Centre (KCMC), Moshi, Tanzania
Department of Medical Parasitology and Entomology, Kilimanjaro Christian Medical University College, Moshi, Tanzania
Department of Medical Parasitology and Entomology, Kilimanjaro Christian Medical University College, Moshi, Tanzania. Pan African Malaria Vector Research Consortium (PAMVERC), Moshi, Tanzania
Information