Abstract
Context: The COVID-19 pandemic has highlighted critical weaknesses in global health systems, underscoring the need to strengthen emergency preparedness capacities. Abidjan, the rapidly growing capital of Côte d'Ivoire, faces unprecedented threats to health and livelihoods due to deadly annual floods and the resulting waterborne diseases such as cholera, dengue fever, and leptospirosis. It must be noted that, to date, the health districts of Abidjan, although basic units of the health system, do not have a regional PHEOC, which raises concerns about their level of preparedness. The National PHEOC, under the supervision of the National Institute of Public Health (NIPH), coordinates preparedness and response to health emergencies. It develops contingency plans and improves its capabilities through simulation exercises. The health districts (HDs) of Abidjan, grouped into two health regions: Abidjan 1 Grands Ponts and Abidjan 2 Lagunes, are not members of the national PHEOC. This observation raises concerns about the capacity of this operational unit to respond quickly to health emergencies in its area of intervention. Consequently, questions arise: how is the coordination and planning of interventions in the event of public health emergencies structured within this specific regional hub that is Abidjan? How prepared are Abidjan's health districts to respond to health risks in the city? Objective: To assess organizational capacities for health emergency preparedness in the two health regions of Abidjan (Côte d’Ivoire) in 2024. Methods: A descriptive cross-sectional study conducted from May 1 to June 8, 2024, among 31 key stakeholders in the ten health districts of Abidjan. A structured questionnaire, based on the 2021 WHO preparedness framework, was administered. Data were entered into SPSS and analyzed. Results: The median age of participants was 47 years, and the male-to-female ratio was 1.4. Sixty-eight percent were general practitioners or pharmacists, and 61% had a specialization in public health. Seventy-seven percent of districts had a Rapid Response Team (RRT), and 13% had conducted simulation exercises. However, 68% reported a lack of funds dedicated to emergencies, and 35% reported a lack of effective alert and awareness mechanisms. Conclusion: This study highlights the crucial importance of preparedness and management of health emergencies in Côte d'Ivoire, particularly in the city of Abidjan. In the health regions of Abidjan, organizational capacities for health emergency preparedness remain insufficient despite increasing vulnerability to epidemics. Consolidate surveillance and alert systems to improve the resilience of the health system.
|
Published in
|
Central African Journal of Public Health (Volume 11, Issue 5)
|
|
DOI
|
10.11648/j.cajph.20251105.13
|
|
Page(s)
|
249-260 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Organizational Capacity, Emergency Preparedness, Health Emergency, Abidjan, Côte d'Ivoire
1. Introduction
The COVID-19 pandemic has revealed major weaknesses in healthcare systems, particularly in terms of preparedness for health emergencies
| [1] | Assembl ME., Sant Mdela, Director L. WHO action in health emergencies Strengthening preparedness for health emergencies: 2021; 19(2005): 1–82. |
[1]
.
Indeed, emergencies typically lead to the displacement of populations to crowded areas where access to basic needs such as water, food, shelter, and other social services is limited. These conditions increase the risk of death from common epidemic and endemic diseases
| [2] | Fan VY, Jamison T, Summers LH, Fan VY. Pandemic risk: how large are the expected losses? 2018; (December): 129-34. |
[2]
.
Abidjan, the rapidly growing capital of Côte d'Ivoire, faces unprecedented threats to health and livelihoods due to deadly annual floods and their corollary waterborne diseases such as cholera, dengue fever, and leptospirosis
| [3] | Kra F, Schmidt-sane M. Africa against epidemics: Key considerations for epidemic preparedness and response in Côte d'Ivoire. 2022. |
| [4] | Official Portal of the Government of Côte d'Ivoire. Posted online on 09/21/2023. 2023. Prevention, preparation, and response to epidemics: Minister Pierre Dimba presents Côte d'Ivoire's response plan at the 78th UN General Assembly. Available at: https://www.gouv.ci/_actualite-article.php?recordID=15716 |
[3, 4]
.
In 2016, Côte d'Ivoire conducted a national assessment using the Strategic Tool for Assessing Risks (STAR) and established a risk register and risk matrix that classifies the level of risk based on associated probability and impact. The method was based on the identification of risks, their history in the country, and the national epidemiological situation. As a result, a total of 53 threats and hazards were identified and prioritized as priority hazards
| [5] | Public Health Emergency Operations Center (COUSP). Mission to identify regional COUSP sites and warehouses: rehabilitation and equipment needs report, March 26 to April 4, 2023. 2023. |
[5]
.
It must be noted that, to date, the health districts of Abidjan, although basic units of the health system, do not have a regional PHEOC, which raises concerns about their level of preparedness
| [6] | MHPHUHC. National Health Development Plan 2021-2025. Report. 2021. |
[6]
. The National PHEOC, under the supervision of the National Institute of Public Health (NIPH), coordinates preparedness and response to health emergencies
| [6] | MHPHUHC. National Health Development Plan 2021-2025. Report. 2021. |
| [7] | World Health Organization. Framework for Action on Health Security in Asia-Pacific: 7-89. |
[6, 7]
. It develops contingency plans and improves its capabilities through simulation exercises. The health districts (HDs) of Abidjan, grouped into two health regions: Abidjan 1 Grands Ponts and Abidjan 2 Lagunes, are not members of the national PHEOC
| [6] | MHPHUHC. National Health Development Plan 2021-2025. Report. 2021. |
[6]
. This observation raises concerns about the capacity of this operational unit to respond quickly to health emergencies in its area of intervention. Consequently, questions arise: how is the coordination and planning of interventions in the event of public health emergencies structured within this specific regional hub that is Abidjan? How prepared are the health districts of Abidjan to respond to health risks in the city?
It is in this context that we deemed it appropriate to conduct this study, which has two main objectives:
1) On the one hand, the literature review found no research that examined the preparedness capacities of districts in Côte d’Ivoire.
2) On the other hand, given the lessons learned from the COVID-19 pandemic, it was imperative to conduct a thorough assessment of the various levels of intervention in health emergency management.
The aim of this research was to contribute to the resilience of the regional health system in Abidjan in the face of health emergencies.
2. General Objective
To assess the compliance of the organizational preparedness capacities of the health regions of Abidjan with a view to responding to health emergencies.
3. Materials and Methods
I. Study Framework
We conducted our study in the city of Abidjan, the political capital of Côte d'Ivoire. Abidjan is the most populous city in Côte d'Ivoire. Since 2001, it has become an “autonomous district” covering 2,119 km
2, comprising the ten municipalities of the former city of Abidjan (422 km
2) and four outlying sub-prefectures that were once rural but have now been swallowed up by Abidjan's urban sprawl. The economic capital of Côte d'Ivoire, the city has a population of 6,321,017 in the 2,119km
2 of the autonomous district of Abidjan, according to the 2021 census, representing 21.5% of the country's population and 60% of its gross domestic product
| [8] | Ané-Kpahé AJ. Management of COVID-19 by local authorities in Côte d'Ivoire: the case of the commune of Yopougon. Georeview. 2023; 33(2): 29-40. |
[8]
. Abidjan is the most populous city in French-speaking West Africa and the second largest city and third largest metropolitan area in the French-speaking world. It comprises ten metropolitan municipalities: Abobo, Yopougon, Adjamé, Plateau, Attécoubé, Cocody, Koumassi, Port-Bouët, Treichville, and Marcory. The activities and tasks of the minimum package of activities in the regional health and public hygiene directorates are defined in Decree 401 of December 18, 2007. Regarding resource mobilization and partnership coordination, the RHD is responsible for organizing and coordinating the implementation of measures to combat epidemics at the regional level. while the departmental directorate is responsible for organizing the management of epidemics and health disasters at the departmental level (investigation and response).
| [9] | MSHP. Decree No. mshp/cab of December 18, 2007, amending the minimum package of activities of regional and departmental directorates of health and public hygiene. 2007. |
[9]
.
II. Type of study
This was a normative evaluation study of the organization of the regional health system in terms of health emergencies.
III. Study location and period
Our study was conducted in the two health regions of the city of Abidjan, as well as in the ten health districts that depend on them. This study took place during the period from May 1 to June 8, 2024.
IV. Study population
The study population consisted of the heads of administrative health structures operating at different levels of the regional health system. We targeted the ten departmental directors, the heads of the Health Action Service (HHAS) and the epidemiological surveillance officers (ESO) of the two health regions of Abidjan.
V. Sampling
A reasoned sampling was carried out, bringing together 34 actors involved in the fight against epidemics. It included the ten departmental directors, the twelve chief medical officers of the Health Action Service (HAS) and the twelve epidemiological surveillance officers (ESO) from the two health regions of Abidjan.
VI. Inclusion/exclusion criteria
(a) Inclusion criteria
Only staff who gave their consent were included in the study.
(b) Exclusion criteria
Trainees present at the time of the evaluation and staff who were unavailable or absent at the time of the evaluation were not included.
VII. Research data collection
A. Data collection tools
a. Reference framework for data collection
The variables examined in this study are derived from the ten (10) components and functions listed in the 2021 WHO document on managing risks associated with emergencies and disasters in the health sector. This World Health Organization report was written to help member countries improve their preparedness and response to various health emergencies.
b. Wording of variables used
Related to:
1) the description of the organizational and functional framework for managing health emergencies.
2) knowledge or existence of a political, strategic, and legislative framework for health emergency management.
3) structural, logistical, and pre-positioning capacities for emergency kits.
4) early warning and surveillance mechanisms.
5) funding for health emergency management activitie.
c. Evaluation criteria used
The assessment criteria are as follows:
1) Proportion ≥ 80%: Satisfactory
2) Proportion: [50%-80%]: Moderate or average
3) Proportion ≤ 50% Unsatisfactory
B. Data collection techniques
The data required for this study were collected using a structured survey questionnaire that had been tested beforehand. We interviewed the departmental director, the head of the Health Action Service (HHAS), and the epidemiological surveillance officer in succession.
VIII. Data processing and analysis
The data were recorded using the Kobocollect app on tablets after setting up individual accounts, then transferred to IBM SPSS 27 software for statistical analysis. Information from interviews with stakeholders was transcribed and examined according to the content of the six thematic areas. Quantitative variables such as age were summarized using measures of central tendency and dispersion (mean with standard deviation, median, interquartile range, and range). Other numerical variables were discretized into categorical variables. Qualitative variables were represented in terms of percentages. Tables and figures (including histograms and diagrams) were created in Excel and then imported into Word for formatting.
IX. Ethical considerations
Authorization was granted by the regional directors in Abidjan to allow us to conduct the interviews. We sought and obtained the consent of the interviewee after clearly explaining the purpose and objectives of the study before administering the questionnaire. We made sure to inform all participants of the voluntary nature of our study, emphasizing that they could interrupt the interview at any time and were not required to answer all questions. The confidentiality of respondents was ensured to prevent any inappropriate use of personal information, and the questionnaires were administered anonymously.
4. Results
I. Socio-demographic characteristics
Of the thirty-four targeted actors, thirty-one were interviewed, 28 from health districts and three from regional directorates.
Responders
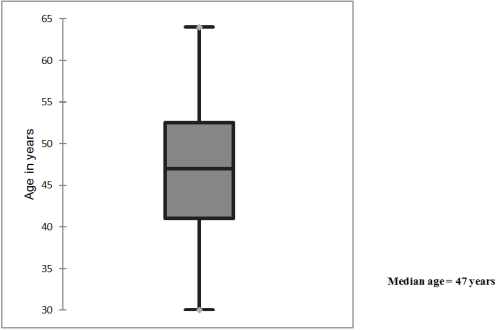
The age of the participants in our study ranged from 30 to 64, with a median age of 47. 75% of participants were under the age of 53.
Table 1. Socio-professional characteristics of respondents.
Variables studied | Sample size n=31 (%) |
Gender of respondent |
Male | 18 (58) |
Female | 13 (42) |
Age of respondent | |
[25-34] | 3 (10) |
[35-44] | 11 (35) |
[45-54] | 13 (42) |
[55-65] | 4 (13) |
Professional experience |
| 20 (65) |
5 years | 11 (35) |
Position |
DD | 7 (23) |
HHAS | 13 (42) |
ESO | 11 (35) |
Level of education |
Doctorate in medicine or general pharmacy | 21 (68) |
Degree in nursing | 6 (19) |
Degree in social sciences and health technology | 4 (13) |
Figure 1. Box plot Age of emergency management.
Most respondents were male (52%). The male-to-female ratio was 1.4. The dominant age group was 45 to 54 years old (42%). One-third (35%) of respondents had more than five years of professional experience in their positions, and doctors and pharmacists accounted for 68% of respondents. Seventy percent of departmental directors were interviewed.
Table 1: Socio-professional characteristics of respondents.
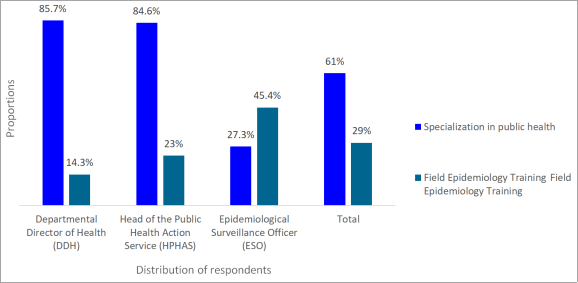
Figure 2. Emergency management responders by type of training, Abidjan, 2024.
61% of respondents had a specialty in public health, and only 29% had received training from the Field Epidemiology Training Program (FETP). HHAS trained in field epidemiology accounted for 23% of the HHAS surveyed.
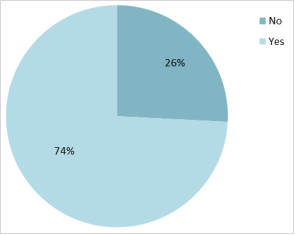
Figure 3. Distribution of respondents according to their experience in managing public health emergencies, 2024.
Respondents who had participated in health emergency management accounted for 76%.
II. Results in key areas of preparedness and response (WHO)
A. Organizational and functional framework for health emergency management
a. Coordination of health emergency management activities
The coordination of activities involves the existence of a coordination team, the holding of coordination meetings even outside of crises, and is responsible for this coordination.
Table 2. Coordination of health emergency management activities.
Variables studied | Number (n=31 (%)) |
Existence of a coordination team |
Yes | 21 (68) |
No | 10 (32) |
Coordination meetings held even outside of crises |
Yes | 24 (77) |
No | 7 (23) |
Manager responsible for coordination during emergencies | n =24 |
DD | 19 (79) |
Administrative authority | 3 (13) |
DR | 2 (8) |
Participation of the community and non-health sectors in coordination meetings |
Yes | 15 (62) |
No | 9 (38) |
The majority of respondents from districts and regional directorates (68%) indicated that their structures had established a team to coordinate activities related to health emergency management, while 32% did not confirm this information. However, 77% of participants said they held coordination meetings even outside of crisis situations. In 79% of cases, the departmental director (DD) was responsible for organizing these meetings, while in 13% of cases, an administrative authority was responsible. The presence of the community and non-health sectors at coordination meetings was ensured for 62% of participants.
b. The existence of a Rapid Response Team
Table 3. The existence of a Rapid Response Team.
Variables studied | Number (%) |
Current existence of a rapid response team (RRT) | n=31 |
Yes | 24 (77) |
No | 7 (23) |
Number of people comprising the EIR | n =24 |
Minimum | 3 |
Maximum | 16 |
Average number | 5,4 ± 3,05 |
Training of this EIR in risk management, emergencies, and health disasters |
Yes | 19 (61) |
No | 12 (39) |
Simulation exercise program for the EIR |
Yes | 4 (13) |
No | 27 (87) |
Regarding the presence of a Rapid Response Team (RRT), participants from all ten districts reported having benefited from its services during the COVID-19 pandemic. However, seven respondents (23%) questioned the sustainability of the team's current functionality. Among the 77% of participants who confirmed its existence, 61% indicated that this team had undergone training, but only 13% of the team had actually benefited from simulation exercises. On average, the number of teammates in the district was 5.4 ± 3.05 per team. Most participants did not specify the One Health skills of their teams.
c. Emergency Planning
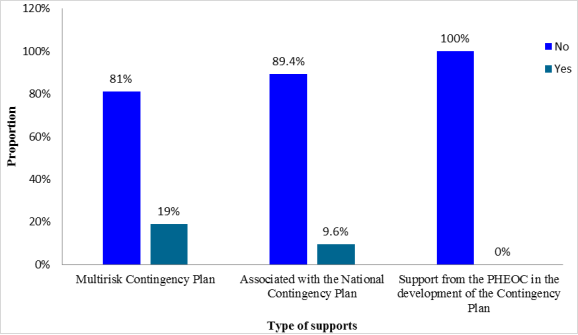
Figure 4. Process for developing contingency plans and support from higher levels.
This figure shows that only 19% of participants say they have a multi-risk contingency plan. Three respondents, or 9.6%, have already participated in the development of national response strategies. Regarding coaching for the design of district-level response plans, none of the participants mentioned having received this specific assistance.
d. The organization of communication in health emergency management
Table 4. The organization of communication in health emergency management.
Variables studied | Number (%)) |
Number of respondents | (n=31) |
Existence of a communication plan |
Yes | 19 (61) |
No | 12 (39) |
Training of the Risk Communication and Community Engagement (RCCE) manager |
Yes | 6 (19) |
No | 25 (81) |
Community awareness activities on the risks associated with health emergencies |
Yes | 20 (65) |
No | 11 (35) |
Means (media) of communication used by the health district during emergencies | N=57 |
Mass campaign | 21 (37) |
Community radio | 15 (26) |
Social media | 2 (4) |
Megaphone | 11 (19) |
Telephone (call center or messaging) | 8 (14) |
According to 61% of participants, a communication plan for health emergencies is in place in the district. Despite the low rate of participants trained in RCCE, 65% of them reported having organized awareness-raising activities concerning at least one health emergency risk. The most frequently used means of communication include mass campaigns (37%) and community radio stations (26%). Only 4% of individuals use social media as a modern communication channel (4%).
B. Political, strategic, or legal framework for health emergency management
a. Awareness of the existence of a policy, strategy, or law that clearly defines the various aspects of health emergency management.
Table 5. Awareness of the existence of a policy, strategy, or law that clearly defines the various aspects of public health emergency management.
Variables studied | Number (%)) |
Number of respondents | (n=31) |
Clear policy on health emergency management |
Yes | 10 (32) |
No | 21 (68) |
International frameworks for emergency and disaster management |
International Health Regulations | 18 (38) |
Sendai Framework | 0 (0) |
WHO Framework for Health Emergency and Disaster Risk Management | 2 (6) |
National frameworks for emergency and disaster management |
NOCP OCSR plans | 6 (19) |
The One Health platform | 10 (32) |
The Public Health Emergency Operations Center housed at the NIPH | 18 (58) |
Only 3% of participants reported being familiar with government policy on health emergency management in Côte d'Ivoire, representing less than half of respondents. Most respondents do not have a thorough understanding of international management frameworks other than the IHR, which is recognized by 58% of respondents. The national PHEOC is known by 58% of respondents, while the NOCP’s OCSR plans and the One Health platform are less familiar, with respective proportions of 19% and 32%.
b. Structural, logistical, and pre-positioning capacities for emergency kits
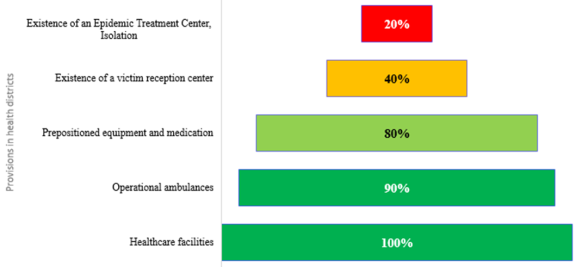
Figure 5. Structural, material, and logistical provisions in health districts.
All health districts (100%) have a designated health facility that is ready to receive patients in the event of a medical emergency. Most districts (90%) have ambulances suitable for emergency patient transport, while 80% of supplies, personal protective equipment, and medicines are pre-positioned. Only 20% of districts have an isolation and treatment center for cases during epidemics.
c. Emergency Alert and Surveillance Mechanism
Table 6. Organization of the monitoring and emergency alert system.
Variables studied | Response modalities | Number (%) N=31 |
Identification and analysis of risks associated with a health emergency |
Yes | 19 (61) |
No | 12 (39) |
Existence of an emergency information (alert) system |
Yes | 28 (90) |
No | 3 (10) |
Type of surveillance used to monitor the risk of a health emergency occurring |
Mixed | 20 (65) |
Passive | 1 (3) |
Active | 10 (32) |
Different sources of emergency alerts |
NHIS/DHIS2/MAGPI | 23 (29) |
Phone | 16 (21) |
Mail | 11 (14) |
Social media/Internet | 28 (36) |
Training in surveillance and early warning systems for emergencies |
Yes | 13 (42) |
No | 18 (58) |
Community participation in monitoring health emergency risks |
Yes | 15 (48) |
No | 16 (52) |
Sixty-one percent (61%) of respondents said they had knowledge of information related to identifying and assessing risks associated with emergencies and disasters in their district. The majority of participants, 90%, said they had an established protocol for circulating emergency information or alerts. Mixed monitoring is used in 65% of cases, combining the formal NHIS/DIHS2/MAGPI circuit (29%) with the use of an informal system based on the WhatsApp social network for information transmission in 36% of situations. In 58% of cases, participants did not receive adequate training in Integrated Response Surveillance and Early Warning (IRSEW), and in 48% of situations, they called on the community to monitor public health emergencies. The average score for this area was 2.
d. Funding for the management of health emergencies
Table 7. Financial organization during the management of health emergencies.
Variables studied | Response modalities | Number (%) N=31 |
Existence of a budget line for emergencies in the Action Plan |
Yes | 8 (26) |
No | 20 (64) |
Don't know | 3 (10) |
Existence of a fund available to deal with emergencies |
Yes | 6 (19) |
No | 21 (68) |
Don't know | 4 (13) |
Most respondents acknowledged the existence of a clear budget line in their Operational Action Plan (64%), but indicated that they did not have funds specifically allocated to respond to potential health emergencies (68%). The average score for this area was 1.
5. Discussion
The discussions will focus on comparing the results obtained in our study with those presented in various reports and studies in the scientific literature. However, certain elements relevant to the objectives of this study have been selected to inform readers. To assess organizational capacities for health emergency management in the health regions of Abidjan, an in-depth analysis of several areas was undertaken to provide an accurate picture of the situation in the health districts that constitute the operational units in this specific context.
1. Socio-demographic characteristics
It is necessary to have dedicated professionals at various levels (national, regional, and local) who are competent in managing emergency strategies and operations. It is essential to have qualified personnel. This study revealed that only 35% of district health officials had more than five years of professional experience, which is less than half. An average of 61% had completed a master's degree in public health, and a small proportion (29%) had completed training in the Field Epidemiology Training Program (FETP). There are significant gaps in the skills of departmental directors, HHAS, and ESO in the city of Abidjan. This skills gap contrasts with the MHPHUHC training initiative, which has been collaborating with the US Centers for Disease Control and Prevention since 2016. This collaboration aims to train leading health professionals and managers to improve surveillance systems and build the capacity needed to respond to emerging and endemic health threats. In the DRC, the joint external evaluation report highlighted the presence of multidisciplinary human resources, mainly located in the capital, but ready to be mobilized quickly to ensure essential capacities in the event of a public health emergency
| [10] | WHO. Joint external evaluation of key RSI capacities in the Democratic Republic of Congo. 2018; 12–6. |
[10]
.
2. Results in key areas of preparedness and response (WHO)
A. Organizational and functional framework
a. Human resources
The health districts of Abidjan have rapid response teams that are trained informally, without standardized documents describing response procedures. The challenges associated with implementing RRTs were addressed in the third edition of the SIMR guide. This manual recommends planning for simulation exercises and promoting One Health collaboration to prepare the rapid response team (RRT)
| [12] | Official Journal of the Republic of Côte d'Ivoire. Decree No. 2088-60 of February 28, 2008, amending Decree No. 2000-822 of November 22, 2000, on the creation, powers, and organization of the National Office for Civil Protection. 2008. |
[12]
.
Despite this shortcoming, it should be noted that these personnel have been able to respond to numerous public health emergencies (such as the COVID-19 pandemic, Ebola, cholera, yellow fever epidemics, and other public health events) occurring in the city of Abidjan. This situation can be attributed to the leadership exercised by national-level actors, who have solid training and significant experience. These are mainly PHEOC teams at the national level.
In the DRC, the joint external evaluation report highlighted the presence of multidisciplinary human resources, mainly located in the capital, but ready to be mobilized quickly to ensure essential capacities in the event of a public health emergency. An effective organization of multidisciplinary response teams is in place to deal with epidemics without the need for external personnel. Professionals such as epidemiologists, clinicians, biostatisticians, information systems experts, veterinarians, social scientists, laboratory technicians, and other public health actors are found at all levels of the health hierarchy
| [13] | United States of America. Special session of the World Health Assembly to consider the development of a WHO convention, agreement, or other international instrument on pandemic preparedness and response. 2021; 1-2. |
[13]
.
b. Emergency planning
Planning at the city level in Abidjan is deficient in terms of preparedness for epidemics and emergencies. No support had been put in place at the national level to help districts develop contingency plans tailored to their context. Nevertheless, a few districts are making efforts to put in place multi-risk plans, although this concerns only a small proportion, namely 19%. The inadequacy of planning had already been noted at the national level during the first joint external evaluation in 2016
| [14] | PN-RRC. Mid-term evaluation report on the implementation of the SENDAI 2015-2030 framework for action in Côte d'Ivoire. 2022. |
[14]
. The score obtained was 2 out of 5 for the establishment and implementation of a national multi-hazard plan at the national level. A score of 1 out of 5 was given for the assessment of risk mapping and priority public health resources
| [14] | PN-RRC. Mid-term evaluation report on the implementation of the SENDAI 2015-2030 framework for action in Côte d'Ivoire. 2022. |
[14]
.
The lack of technical support from partners and national experts for the design of a multi-hazard plan, preparedness, and response to public health emergencies at the regional level, or more specifically at the district level, impacts planning capacities and represents a gap in preparedness.
c. Coordination and communication
It would be appropriate to establish coordination mechanisms for health emergency management, following the model for the implementation of Regional Health Plans (PRES), in order to ensure appropriate coordination at all levels of the health system, both within the health sector and with other sectors. The involvement and workload of the departmental director (DD) in supervising emergency management in Abidjan are considered moderate by 68% of his staff. In practice, coordination meetings are often considered equivalent to district management team (DMT) meetings, which may explain the respondents' opinion. Thanks to the decentralization policy launched by the MHPHUHC and the planned long-term establishment of a Regional Public Health Emergency Operations Center in each Regional Health Center of Excellence, Abidjan should have a more integrative coordination mechanism ensuring multisectoral and multidisciplinary coordination
| [5] | Public Health Emergency Operations Center (COUSP). Mission to identify regional COUSP sites and warehouses: rehabilitation and equipment needs report, March 26 to April 4, 2023. 2023. |
[5]
. Based on this collaborative principle, responsibility for coordination should lie with the regional or district administrative authority, rather than at the national level.
B. The political, strategic, and legal framework
It is essential to integrate considerations related to the management of risks associated with emergencies and disasters into appropriate policies and strategies, supported by adequate legislation.
Regarding knowledge or awareness of the existence of a government policy or law governing the various aspects of health emergency management in the country, only 32% of health officials in Abidjan reported being aware of it. This lack of awareness is surprising, given that Côte d'Ivoire has implemented and promoted, since 2019, its public health policy focused on the management of health emergencies and epidemics, in accordance with Law No. 2019-677 of July 23, 2019, which establishes priority health guidelines. This policy is also integrated into the National Health Development Plan (NHDP) 2021-2025, which is the main guide for decision-makers in the health sector. Another aspect of the legal framework is the low level of mastery of essential tools such as the IHR, the One Health platform, and OCSR plans, which are indispensable for the implementation of public health emergency preparedness and management provisions.
In Algeria, the appropriate laws and regulations are in place, but their implementation has often been delayed due to a lack of familiarity among stakeholders. Despite the publication of the policy on the Ministry of Health's website, access to it has proven problematic. Over the years, the community, including both professionals and the general population, has gradually assimilated it
| [11] | WHO. Technical guide for integrated disease surveillance and response: Section 10 – Adapting integrated disease surveillance and response (IDSR) to emergency situations or fragile health systems. Vol. 5. 2019. |
[11]
.
a. Structural, logistical, and emergency kit pre-positioning capacities
Logistical support will include the storage and pre-positioning of medicines and equipment, the establishment of efficient supply chains, and transportation systems. Due to the COVID-19 pandemic, inputs such as personal protective equipment and other supplies have been provided to districts. Referral health facilities are well mapped at the district level. In Burkina Faso, however, referral health facilities are not officially designated for each point of entry into the country
| [15] | Sawadogo B, Fall B, Ndoye B, Sonko I, Bandoh DA, Kenu E, et al. Evaluation of Burkina Faso's capacity to prepare for and respond to health emergencies. J Interv Epidemiol Public Heal. 2022; 5(4). |
[15]
. One of the main challenges in terms of logistical support for the districts of Abidjan is the capacity to have isolation facilities and laboratories equipped with adequate biosafety skills. These shortcomings are driven not only by a failure to comply with the health hierarchy regarding the deployment of level 2 infrastructure, but also by the absence of an effective biomedical logistics policy.
b. Emergency alert and surveillance mechanisms
It is essential to strengthen information management skills to support risk and needs assessment, disease surveillance, and other early warning systems. It is essential to establish mechanisms for collecting, analyzing, and disseminating information to ensure that relevant data reaches the appropriate individuals in a timely manner.
In Algeria, this alert mechanism was improved in 2019 through the updating of its epidemic emergency program and the strengthening of surveillance and alert systems in response to the threat of Ebola virus disease
| [11] | WHO. Technical guide for integrated disease surveillance and response: Section 10 – Adapting integrated disease surveillance and response (IDSR) to emergency situations or fragile health systems. Vol. 5. 2019. |
[11]
. Similarly, in the WHO European Region, countries have worked to strengthen their national surveillance systems, including early warning mechanisms and local surveillance. This surveillance focuses on the analysis and timely communication of epidemiological data
| [1] | Assembl ME., Sant Mdela, Director L. WHO action in health emergencies Strengthening preparedness for health emergencies: 2021; 19(2005): 1–82. |
[1]
.
c. Funding for the management of health emergencies
Analysis of data relating to the financing of health emergency management highlights a structural weakness in the operational preparedness of the respondents. Although nearly one-third of respondents (26%) report having a dedicated budget line for emergencies in their action plan, the majority (64%) acknowledge the absence of such a line, and a significant number (10%) are unaware of it. This finding is consistent with the observations of Maltai et al. (2022)
| [16] | S. Maltais, S. Brière, et S. Yaya, « Résilience face aux crises sanitaires : un modèle d’analyse pour mieux cerner la complexité de gestion dans les États fragiles », lsp, n 88, p. 132‑151, juill. 2022, https://doi.org/ 10.7202/1090984ar |
[16]
, who emphasize that the inclusion of a specific budget line is essential to ensuring responsiveness to health crises. The situation is even more worrying when it comes to the immediate availability of funds: only 19% of respondents report the existence of financial resources that can be mobilized quickly, while 68% indicate that they do not exist and 13% are unable to say. This shortfall can have direct consequences on the speed and effectiveness of the response in an emergency. As demonstrated by Sachs (2001)
| [17] | J. Sachs et Weltgesundheitsorganisation, Éd., Macroéconomie et santé: investir dans la santé pour le développement économique ; rapport de la Commission Macroéconomie et Santé ; le 20 décembre 2001. Genève: Organisation Mondiale de la Santé, 2002. |
[17]
, delays in mobilizing funds are often an aggravating factor, prolonging the health and socioeconomic impact of an epidemic.
6. Conclusions
This study highlights the crucial importance of preparedness and management of health emergencies in Côte d'Ivoire, particularly in the city of Abidjan.
In Abidjan's health regions, organizational capacities for health emergency preparedness remain insufficient despite growing vulnerability to epidemics (cholera, dengue fever, yellow fever) and the COVID-19 pandemic. It is imperative to strengthen staff training, develop and test multi-risk response plans, allocate dedicated financial resources, and consolidate surveillance and warning systems to improve the resilience of the health system.
Abbreviations
DD | Departmental Director |
DR | Regional Directorate |
DRC | Democratic Republic of Congo |
ESO | Epidemiological Surveillance Officer |
HHAS | Head of Health Action Services |
NHIS/DHIS2/MAGPI | National Health Information System/ District Health Information Software 2/ Mid-Atlantic GigaPOP à Philadelphie pour Internet |
MHPHUHC | Ministry of Health, Public Hygiene and Universal Health Coverage |
NOCP OCSR | National Office of Civil Protection Organization of the Civil Security Response |
PHEOC | Public Health Emergency Operations Center |
RHD | Regional Health Directorate |
Acknowledgments
We would like to thank all participants in this study.
Author Contributions
Ano Ama Kounangui Marie Noëlle: Conceptualization, Project administration, Supervision, Writing – original draft, Formal Analysis, Methodology, Visualization, Writing review and editing, Validation
Ekra Kouadio Daniel: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft, Writing – review & editing
Akani Bangaman Christian: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft
Makonga Makonga Franck: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft
Krouma Sita: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft
Douba Alfred: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft, Writing – review & editing
Issaka Tiembré: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft, Writing – review & editing
Funding
This work is not supported by any external funding.
Institutional Review Board Statement
The study was reviewed and approved by the Director of the National Institute of Public Health.
Data Availability Statement
The data supporting the outcome of this research work has been reported in this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Assembl ME., Sant Mdela, Director L. WHO action in health emergencies Strengthening preparedness for health emergencies: 2021; 19(2005): 1–82.
|
| [2] |
Fan VY, Jamison T, Summers LH, Fan VY. Pandemic risk: how large are the expected losses? 2018; (December): 129-34.
|
| [3] |
Kra F, Schmidt-sane M. Africa against epidemics: Key considerations for epidemic preparedness and response in Côte d'Ivoire. 2022.
|
| [4] |
Official Portal of the Government of Côte d'Ivoire. Posted online on 09/21/2023. 2023. Prevention, preparation, and response to epidemics: Minister Pierre Dimba presents Côte d'Ivoire's response plan at the 78th UN General Assembly. Available at:
https://www.gouv.ci/_actualite-article.php?recordID=15716
|
| [5] |
Public Health Emergency Operations Center (COUSP). Mission to identify regional COUSP sites and warehouses: rehabilitation and equipment needs report, March 26 to April 4, 2023. 2023.
|
| [6] |
MHPHUHC. National Health Development Plan 2021-2025. Report. 2021.
|
| [7] |
World Health Organization. Framework for Action on Health Security in Asia-Pacific: 7-89.
|
| [8] |
Ané-Kpahé AJ. Management of COVID-19 by local authorities in Côte d'Ivoire: the case of the commune of Yopougon. Georeview. 2023; 33(2): 29-40.
|
| [9] |
MSHP. Decree No. mshp/cab of December 18, 2007, amending the minimum package of activities of regional and departmental directorates of health and public hygiene. 2007.
|
| [10] |
WHO. Joint external evaluation of key RSI capacities in the Democratic Republic of Congo. 2018; 12–6.
|
| [11] |
WHO. Technical guide for integrated disease surveillance and response: Section 10 – Adapting integrated disease surveillance and response (IDSR) to emergency situations or fragile health systems. Vol. 5. 2019.
|
| [12] |
Official Journal of the Republic of Côte d'Ivoire. Decree No. 2088-60 of February 28, 2008, amending Decree No. 2000-822 of November 22, 2000, on the creation, powers, and organization of the National Office for Civil Protection. 2008.
|
| [13] |
United States of America. Special session of the World Health Assembly to consider the development of a WHO convention, agreement, or other international instrument on pandemic preparedness and response. 2021; 1-2.
|
| [14] |
PN-RRC. Mid-term evaluation report on the implementation of the SENDAI 2015-2030 framework for action in Côte d'Ivoire. 2022.
|
| [15] |
Sawadogo B, Fall B, Ndoye B, Sonko I, Bandoh DA, Kenu E, et al. Evaluation of Burkina Faso's capacity to prepare for and respond to health emergencies. J Interv Epidemiol Public Heal. 2022; 5(4).
|
| [16] |
S. Maltais, S. Brière, et S. Yaya, « Résilience face aux crises sanitaires : un modèle d’analyse pour mieux cerner la complexité de gestion dans les États fragiles », lsp, n 88, p. 132‑151, juill. 2022,
https://doi.org/ 10.7202/1090984ar
|
| [17] |
J. Sachs et Weltgesundheitsorganisation, Éd., Macroéconomie et santé: investir dans la santé pour le développement économique ; rapport de la Commission Macroéconomie et Santé ; le 20 décembre 2001. Genève: Organisation Mondiale de la Santé, 2002.
|
Cite This Article
-
APA Style
Noëlle, A. A. K. M., Daniel, E. K., Christian, A. B., Franck, M. M., Sita, K., et al. (2025). Assessment of the Level of Preparedness for Emergency Situations of Health Emergency Management Organizations in Abidjan, Côte d'Ivoire. Central African Journal of Public Health, 11(5), 249-260. https://doi.org/10.11648/j.cajph.20251105.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Noëlle, A. A. K. M.; Daniel, E. K.; Christian, A. B.; Franck, M. M.; Sita, K., et al. Assessment of the Level of Preparedness for Emergency Situations of Health Emergency Management Organizations in Abidjan, Côte d'Ivoire. Cent. Afr. J. Public Health 2025, 11(5), 249-260. doi: 10.11648/j.cajph.20251105.13
Copy
|
Download
AMA Style
Noëlle AAKM, Daniel EK, Christian AB, Franck MM, Sita K, et al. Assessment of the Level of Preparedness for Emergency Situations of Health Emergency Management Organizations in Abidjan, Côte d'Ivoire. Cent Afr J Public Health. 2025;11(5):249-260. doi: 10.11648/j.cajph.20251105.13
Copy
|
Download
-
@article{10.11648/j.cajph.20251105.13,
author = {Ano Ama Kounangui Marie Noëlle and Ekra Kouadio Daniel and Akani Bangaman Christian and Makonga Makonga Franck and Krouma Sita and Douba Alfred and Issaka Tiembré},
title = {Assessment of the Level of Preparedness for Emergency Situations of Health Emergency Management Organizations in Abidjan, Côte d'Ivoire
},
journal = {Central African Journal of Public Health},
volume = {11},
number = {5},
pages = {249-260},
doi = {10.11648/j.cajph.20251105.13},
url = {https://doi.org/10.11648/j.cajph.20251105.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20251105.13},
abstract = {Context: The COVID-19 pandemic has highlighted critical weaknesses in global health systems, underscoring the need to strengthen emergency preparedness capacities. Abidjan, the rapidly growing capital of Côte d'Ivoire, faces unprecedented threats to health and livelihoods due to deadly annual floods and the resulting waterborne diseases such as cholera, dengue fever, and leptospirosis. It must be noted that, to date, the health districts of Abidjan, although basic units of the health system, do not have a regional PHEOC, which raises concerns about their level of preparedness. The National PHEOC, under the supervision of the National Institute of Public Health (NIPH), coordinates preparedness and response to health emergencies. It develops contingency plans and improves its capabilities through simulation exercises. The health districts (HDs) of Abidjan, grouped into two health regions: Abidjan 1 Grands Ponts and Abidjan 2 Lagunes, are not members of the national PHEOC. This observation raises concerns about the capacity of this operational unit to respond quickly to health emergencies in its area of intervention. Consequently, questions arise: how is the coordination and planning of interventions in the event of public health emergencies structured within this specific regional hub that is Abidjan? How prepared are Abidjan's health districts to respond to health risks in the city? Objective: To assess organizational capacities for health emergency preparedness in the two health regions of Abidjan (Côte d’Ivoire) in 2024. Methods: A descriptive cross-sectional study conducted from May 1 to June 8, 2024, among 31 key stakeholders in the ten health districts of Abidjan. A structured questionnaire, based on the 2021 WHO preparedness framework, was administered. Data were entered into SPSS and analyzed. Results: The median age of participants was 47 years, and the male-to-female ratio was 1.4. Sixty-eight percent were general practitioners or pharmacists, and 61% had a specialization in public health. Seventy-seven percent of districts had a Rapid Response Team (RRT), and 13% had conducted simulation exercises. However, 68% reported a lack of funds dedicated to emergencies, and 35% reported a lack of effective alert and awareness mechanisms. Conclusion: This study highlights the crucial importance of preparedness and management of health emergencies in Côte d'Ivoire, particularly in the city of Abidjan. In the health regions of Abidjan, organizational capacities for health emergency preparedness remain insufficient despite increasing vulnerability to epidemics. Consolidate surveillance and alert systems to improve the resilience of the health system.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessment of the Level of Preparedness for Emergency Situations of Health Emergency Management Organizations in Abidjan, Côte d'Ivoire
AU - Ano Ama Kounangui Marie Noëlle
AU - Ekra Kouadio Daniel
AU - Akani Bangaman Christian
AU - Makonga Makonga Franck
AU - Krouma Sita
AU - Douba Alfred
AU - Issaka Tiembré
Y1 - 2025/09/15
PY - 2025
N1 - https://doi.org/10.11648/j.cajph.20251105.13
DO - 10.11648/j.cajph.20251105.13
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 249
EP - 260
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20251105.13
AB - Context: The COVID-19 pandemic has highlighted critical weaknesses in global health systems, underscoring the need to strengthen emergency preparedness capacities. Abidjan, the rapidly growing capital of Côte d'Ivoire, faces unprecedented threats to health and livelihoods due to deadly annual floods and the resulting waterborne diseases such as cholera, dengue fever, and leptospirosis. It must be noted that, to date, the health districts of Abidjan, although basic units of the health system, do not have a regional PHEOC, which raises concerns about their level of preparedness. The National PHEOC, under the supervision of the National Institute of Public Health (NIPH), coordinates preparedness and response to health emergencies. It develops contingency plans and improves its capabilities through simulation exercises. The health districts (HDs) of Abidjan, grouped into two health regions: Abidjan 1 Grands Ponts and Abidjan 2 Lagunes, are not members of the national PHEOC. This observation raises concerns about the capacity of this operational unit to respond quickly to health emergencies in its area of intervention. Consequently, questions arise: how is the coordination and planning of interventions in the event of public health emergencies structured within this specific regional hub that is Abidjan? How prepared are Abidjan's health districts to respond to health risks in the city? Objective: To assess organizational capacities for health emergency preparedness in the two health regions of Abidjan (Côte d’Ivoire) in 2024. Methods: A descriptive cross-sectional study conducted from May 1 to June 8, 2024, among 31 key stakeholders in the ten health districts of Abidjan. A structured questionnaire, based on the 2021 WHO preparedness framework, was administered. Data were entered into SPSS and analyzed. Results: The median age of participants was 47 years, and the male-to-female ratio was 1.4. Sixty-eight percent were general practitioners or pharmacists, and 61% had a specialization in public health. Seventy-seven percent of districts had a Rapid Response Team (RRT), and 13% had conducted simulation exercises. However, 68% reported a lack of funds dedicated to emergencies, and 35% reported a lack of effective alert and awareness mechanisms. Conclusion: This study highlights the crucial importance of preparedness and management of health emergencies in Côte d'Ivoire, particularly in the city of Abidjan. In the health regions of Abidjan, organizational capacities for health emergency preparedness remain insufficient despite increasing vulnerability to epidemics. Consolidate surveillance and alert systems to improve the resilience of the health system.
VL - 11
IS - 5
ER -
Copy
|
Download