6. Results
6.1. Political Will and Accountability
Togo has adopted various normative and regulatory documents to guide the health sector, with particular attention to reproductive health and family planning. These documents provide an essential reference framework for implementing interventions and strengthening services in these domains. The
table 1 below shows Key Policies and Legal Frameworks Related to Family Planning Financing in Togo.
Table 1. Key Policies and Legal Frameworks Related to Family Planning Financing in Togo.
Policy/Law | Year | Key Issues Related to FP Financing |
Law No. 2007-005 on Reproductive Health | 2007 | Affirms the right to reproductive health for all and establishes the State’s responsibility in providing and financing contraceptive methods. The law also allows the sale of contraceptive products under public coordination. |
Public Health Code | 2009 | Authorizes the provision of all FP methods (except abortion) and ensures their availability in public and private health facilities. Strengthens public leadership in coordinating funding. |
National Costed Implementation Plan for FP (PANB) | 2023-2026 | Stabilizes domestic financing for FP through a dedicated budget line. Encourages advocacy to increase national and local resources for FP. |
National Health Development Plan (PNDS) | 2023-2027 | Prioritizes the reduction of maternal and neonatal mortality and the strengthening of FP services. Emphasizes the integration of modern contraceptive methods into antenatal and postnatal care. |
National Health Policy Toward 2030 | 2023 | Provides a general framework aimed at universal access to quality health services, including FP. Emphasizes system resilience and participation of local stakeholders in financing. |
National FP Financing Strategy | 2022 | Sets objectives to mobilize sustainable domestic resources and reduce dependence on international partners for funding FP products and services. |
The
table 2 below shows Gaps and Strengths in the Legal and Policy Framework for Sexual and Reproductive Health and Family Planning (SR/FP) in Togo.
Table 2. Gaps and Strengths in the Legal and Policy Framework for SR/FP in Togo.
Gap/Strength | Description | Consequences |
Outdated Reproductive Health Law (2007) | The law is outdated and does not reflect WHO’s new orientations (new technologies, sexual minorities, abortion, etc.). | Mismatch between the legal framework and current needs. Obstacle to the adoption of modern SR/FP policies. |
Absence of Implementing Regulations | No regulatory texts have been adopted to govern the implementation of the SR law. | Difficulty for providers to comply with the law. Limited access to guaranteed rights for beneficiaries. |
Existence of Strategic Plans (PNDS, PANB) | Policies are accompanied by detailed strategic plans (PNDS 2023-2027, PANB 2023-2026). | Delays in disbursing allocated funds. Weak alignment between plan priorities and local realities. |
Weak Dissemination of Laws and Policies | Laws and policies, such as the SR law and the PANB, are not well known at the subnational level. | Lack of awareness of legal provisions among local staff and communities. Difficulty in engaging local actors in advocacy efforts. |
Dependence on External Funding | A large share of contraceptive product funding comes from technical and financial partners (UNFPA, USAID). | Program vulnerability in the event of reduced or withdrawn external funding. Low mobilization of domestic resources for SR/FP. |
6.2. Political and Financial Commitments to Health and Family Planning in Togo
For several years, Togo has made significant commitments to improve the health of its population, particularly in the areas of FP and sexual and reproductive health (SRH).
First, under the Abuja Declaration, the Togolese government committed, as early as 2002, to increase the national health budget allocation by at least one percentage point annually. The goal is to progressively reach the 15% target recommended by African Heads of State in the Abuja Declaration adopted in April 2001.
Additionally, as part of the FP2030 initiative and the Ouagadougou Partnership (OP), Togo has made clear and measurable commitments to strengthen access to quality FP and SRH services.
6.3. Togo’s Commitments Under FP2030
Within the FP2030 initiative, Togo has established an ambitious vision for 2030. The overarching objective is to ensure equitable access to quality sexual and reproductive health services, including family planning, for the entire population. Particular attention is given to adolescents, youth, and women including those living in emergency situations in accordance with fundamental human rights.
To achieve its vision for improved family planning, Togo has set several specific goals. Central to these is increasing the modern contraceptive prevalence rate (mCPR), aiming to raise mCPR among women in union from 23.1% in 2020 to 32% by 2026, and for all women from 20.4% to 29.5% over the same period. The country also seeks to ensure a sustainable supply of contraceptives by boosting national budget allocations; in 2022, a government subsidy was introduced to cover 50% of contraceptive needs, with national contributions expected to increase by 25% annually from 2023 to 2026. Additionally, Togo aims to expand access for adolescents and youth to accurate information and youth-friendly services to reduce unmet needs in this vulnerable group. To support consistent availability, the country plans to strengthen logistics and distribution systems, targeting an increase in the proportion of health facilities without stockouts from 36.9% in 2020 to 70% by 2026.
6.4. Togo’s Commitments Under the Ouagadougou Partnership
As a member of the Ouagadougou Partnership, Togo has made concrete commitments to strengthen the sustainability of FP financing and promote greater local ownership. These include mobilizing increased domestic resources to reduce reliance on international technical and financial partners and adopt a more autonomous and sustainable approach to SRH financing. Additionally, Togo is committed to enhancing civil society’s involvement in FP implementation by mobilizing 10% of the required financial resources through local initiatives, thereby reinforcing collaboration with CSOs and local governments.
6.5. Commitments by Political Decision-makers
In addition to technical and strategic initiatives, Togolese authorities have made strong budgetary and institutional commitments to ensure the sustainability of family planning efforts.
Since 2016, the government has established a dedicated budget line for contraceptive security. This line has been consistently maintained, demonstrating a strong political will to sustainably support access to contraceptives.
Policymakers have pledged to gradually increase domestic funding, in order to support the effective implementation of the National Costed Implementation Plans (PANB). This approach aims to achieve national strategic objectives in family planning while reducing reliance on external funding.
The government has also expressed its intent to strengthen intersectoral coordination, particularly among relevant ministries and technical and financial partners. The objective is to ensure the continuity of contraceptive supply nationwide through a coherent and integrated approach to intervention.
The
table 3 below provides an Overview of Health and Family Planning Programs in Togo.
Table 3. Overview of Health and Family Planning Programs in Togo.
Program/Regime Name | Objective | Geographic Scope | Target Population | Covered Population (Year) | Funding Sources | Governance & Covered Services |
Universal Health Insurance Scheme (AMU) | Achieve universal health coverage (UHC) to reduce financial risks related to healthcare. | National | All citizens and permanent residents. | 6.01% in 2023 | Household contributions, public subsidies, technical and financial partners (TFPs) | Governed by INAM and CNSS; covers basic medical services and hospital care. |
SR/FP Program | Secure contraceptive products and FP services. | National | Women of reproductive age, adolescents. | Data not available | Public budget, UNFPA, USAID, other TFPs | Managed by DSME and partners; includes contraceptives, awareness campaigns, and free access during open days. |
School AMU | School health insurance for students in public and private schools. | National | Primary and secondary school students. | 2 million students in 2022 | Public subsidies and TFPs | Managed by INAM and Ministry of Education; covers basic consultations and hospitalizations. |
Wezou Program | Partial coverage of healthcare costs for pregnant women and newborns. | Pilot in Kara, then national expansion | All pregnant women regardless of status. | Pilot in 2021, expansion planned | State budget (3 billion FCFA mobilized) | Managed by Ministry of Health; covers prenatal consultations, normal deliveries, cesarean sections within defined limits. |
Medical Assistance Scheme (RAM) | Support for economically vulnerable populations. | Progressive rollout | Populations living in poverty. | Data not available | Public budget and external funding | Governed by CNSS; covers essential health services. |
SWEDD (Sahel Women Empowerment and Demographic Dividend) | Empower women and girls in health, education, and the economy. | Regional (West Africa) | Girls and women of reproductive age. | Data not available | World Bank, TFPs | Led by Ministry for the Promotion of Women; includes FP awareness, economic empowerment, education, and early marriage prevention. |
6.6. Mapping the Budget Process, Key Advocacy Stakeholders, and Advocacy Opportunities
6.6.1. Mapping the Health Sector Budgeting Process
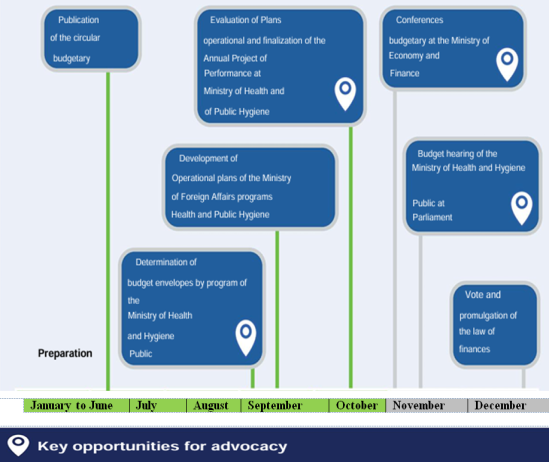
The State budget process in Togo follows an annual cycle running from January to December. Although the exact dates of budget formulation may vary from year to year, the process generally adheres to a similar timeline and level of engagement from ministries, localities, and Parliament.
The annual cycle officially begins when the Ministry of Economy and Finance issues the budget circular in July. This circular outline the timeline for each step of the budget cycle and provides guidelines for sectoral budget proposals. Throughout this process, numerous opportunities exist for civil society organizations (CSOs) to engage in advocacy, particularly to influence allocations for the health sector and, more specifically, for family planning (FP).
For the exact dates and milestones of the current year’s budgeting cycle, stakeholders are advised to consult the most recent budget circular, as well as to engage with the Ministry of Health and Public Hygiene or the National Assembly. The
figure 1 below illustrates identified advocacy opportunities
Figure 1. Advocacy opportunities.
6.6.2. Budget Preparation Phase
In July, during the budget preparation year, the Ministry of Economy and Finance (MEF) initiates the budget process by issuing a budget circular. This circular provides ministries and agencies with guidelines for drafting the upcoming fiscal year’s budget.
Following the issuance of the budget circular, the Financial Affairs Directorate (DAF) of the Ministry of Health (MOH) informs all programs under the MOH including the Directorate of Maternal and Child Health (DSME) of the budget ceilings. The DAF establishes ceilings based on the previous year’s MOH ceiling, historical allocations to each program, and needs expressed by the programs themselves.
Typically, in September, the MOH programs develop their operational plans for the upcoming year. Each plan outlines the planned activities, monitoring indicators, and requested resources. For some expenditure categories, programs may request amounts that exceed the indicative envelope set by the DAF; such envelopes are considered "indicative." However, the DAF prohibits programs from requesting more than the indicative ceilings for non-variable expenditure categories such as operating costs.
In October, the General Directorate of Budget and Finance (DGBF) of the MEF sends a budget framework letter to all ministries. This letter describes the country's macroeconomic context, fiscal policies, and budget ceilings allocated to each ministry. The MOH ceiling is based on past budget execution levels, the priorities outlined in the National Health Development Plan (PNDS), the Medium-Term Expenditure Framework (MTEF), and projected donor contributions.
Following this, the DAF assesses the MOH’s Annual Performance Plan (PAP), which summarizes each program's activities and proposed budgets. The DAF adjusts or validates financial requests from programs according to the budget framework ceiling, prior allocations, and ministry priorities. By November, the MOH submits its PAP and corresponding budget to the DGBF. Budget conferences are held where DAF must justify proposed budget lines for specific programs and expenditure categories.
After discussions with each ministry's DAF, the DGBF consolidates the approved budgets by ministry and program (including family planning) into the draft finance bill. Once finalized, the draft finance bill is submitted to the Council of Ministers by the MEF. After adoption by the Council of Ministers, the draft becomes a proposed finance bill and is submitted to the National Assembly. The budget allocation for family planning can change across the draft, proposed, and enacted finance bills; therefore, CSOs must monitor these documents carefully and engage in advocacy accordingly.
6.6.3. Approval and Execution Phases of the Budget
The approval process of Togo’s state budget in Parliament follows a structured sequence. In November, the Prime Minister submits the finance bill, accompanied by a cover letter, to the National Assembly. The Finance Committee then reviews the bill in consultation with the Ministry of Economy and Finance (MEF) and relevant technical departments from other ministries, incorporating feedback from various parliamentary committees. Each committee may delegate members to participate in the Finance Committee’s discussions. During budget debates, the Minister of Economy and Finance, along with other government representatives, presents the proposed budget. Each minister, including the Minister of Health, defends their respective budgets before the Finance Committee. Members of Parliament (MPs) analyze performance and program documents, pose questions, and advocate for budget allocations that address the health and development priorities of their constituencies. Although CSOs members attend these sessions as observers, they may influence MPs beforehand. The finance law must be adopted by Parliament before December 31, with the MEF Minister responding to critiques and presenting the government's final position, following a recommendation from the Senate. Once promulgated by the President of the Republic, the budget takes effect between December and January. During the execution phase, the MEF requires ministries and programs to submit financial documentation categorized by expenditure type prior to fund disbursement.
6.6.4. Advocacy Opportunities
The budget process presents several critical advocacy opportunities. Stakeholders aiming to align the public budget with specific health sector priorities should leverage these moments to influence key decision-makers. During budget preparation, advocates can meet with the DAF. After submission to the MEF, continued advocacy ensures health priorities are retained in the draft bill. Globally, targeted advocacy at key points of the budget cycle has proven effective in increasing health allocations. Advocates should prepare in advance, identify key decision-makers, compile evidence, and develop compelling advocacy messages.
6.6.5. CSO Advocacy Opportunities
CSOs can intervene at multiple points during the process to keep HIV and family planning funding prioritized. The infographic below (not included here) summarizes these opportunities.
Key Audiences for Advocacy
DAF of the Ministry of Health: Prepares the ministry’s budget, defends it during joint reviews, and submits documentation for Treasury disbursements. It favors programs aligned with ministry priorities and well-justified funding requests.
DGBF of the MEF: Oversees many stages of the budget process, defines ceilings, and includes MOH (especially the National AIDS Control Program) in the draft finance bill. Prefers programs with strong past budget execution and alignment with the PNDS.
Finance Committee of the National Assembly: Plays a key role in reviewing the bill and influencing final allocations. Supports interventions promoting population well-being. Other MPs advocate for programs benefiting their constituencies.
Health Sector Funding Sources
According to the 2023 Annual Performance Report, health financing in Togo is supported by multiple complementary sources with varying levels of contribution. The government budget accounts for only 8.80% of the national budget, approximately USD 230.7 million out of a total of USD 2.62 billion. Health insurance schemes, primarily the compulsory health insurance introduced in 2023, contribute 3.6%. Households remain the largest contributors, covering 66.0% of total health expenditures through out-of-pocket payments, voluntary contributions, co-payments, and service fees. External funding from bilateral and multilateral partners, grants, and other aid sources plays a significant role, representing 42.95% of the sector’s financial resources.
Proportion of the National Budget Allocated to Health (in thousands of USD)
Between 2017 and 2023, Togo’s health budget experienced a significant increase in absolute terms, reflecting the government’s growing commitment to the sector. The share of public expenditure dedicated to health rose from approximately 6.5% in 2017 to nearly 7.1% in 2023, indicating a strengthened prioritization of health in national budgetary policies.
Overall budget execution remained satisfactory, with a generally strong alignment between allocations, disbursements, and actual expenditures throughout most of the period. However, discrepancies observed in 2018, and more recently in 2021 and 2023, highlight challenges in fund management or accounting, as well as potential delays in disbursement. These fluctuations call for increased vigilance to ensure the optimal and transparent use of allocated resources.
The notable increase in funding starting in 2020 likely coincides with the exceptional mobilization of resources in response to the COVID-19 pandemic, underscoring the country’s capacity to adapt its budget to public health emergencies. Nevertheless, the upward trend observed through 2023 confirms that health remains a long-term strategic priority.
To ensure the effectiveness of these investments, it is essential to strengthen budget monitoring, evaluation, and management mechanisms, while pursuing strategies aimed at stabilizing and optimizing health financing. Such efforts will contribute to more effectively addressing the growing public health needs and enhancing the impact of expenditures in this critical sector. The analysis of
Table 4 and
figure 3, 4 and 5 below shows that 1,3% of the national health budget is allocated to family planning.
Table 4. Health Sector Budget Allocation (2017-2023).
Year | Total Health Budget (USD thousands) | Disbursed Health Budget (USD thousands) | Health Budget Expenditures (USD thousands) | % of Public Expenditures on Health |
2017 | 126,260 | 126,260 | 115,781 | 6.45% |
2018 | 161,270 | 161,270 | 148,369 | 5.49% |
2019 | 413,274 | 413,274 | 379,356 | 6.20% |
2020 | 613,510 | 613,510 | 524,715 | 8.30% |
2021 | 569,799 | 527,775 | 517,127 | 7.00% |
2022 | 676,588 | 676,588 | 585,496 | 7.10% |
2023 | 875,358 | 683,437 | 932,212 | 7.10% |
Source Annual Performance Report (2020, 2021, 2022, 2023)
6.7. Budget Process and Timeline - Health Sector
The budgeting process for the health sector follows both a top-down (national level) and bottom-up (subnational level) structure, in accordance with Organic Law No. 2014-013 of June 27, 2014, relating to public finance laws. Budget allocation is based on the needs of central directorates, programs, and decentralized services.
Table 5. Budget Preparation Process Health Sector.
Step | Period | Responsible Entity |
Needs Assessment | February to April | Regional Directorates, DPS, and Local Health Facilities |
Budget Framework Letter | September | Prime Minister and Ministry of Economy and Finance (MEF) |
Preparation of PAP/DPPD | September to October | Ministry of Health (RPROG, Action Managers) |
Arbitration and Validation | October to November | MEF, Council of Ministers |
Parliamentary Adoption | November to December | National Assembly |
PAP - Priority Action Program
The Priority Action Program (PAP) is a budget planning document that consolidates the priority actions to be implemented in the health sector to achieve established goals. It is aligned with the National Health Development Plan (PNDS) and serves as a basis for the allocation of financial resources. The PAP enables the monitoring of program implementation and the evaluation of their impact.
DPPD - Multiannual Expenditure Planning Document
The DPPD is a strategic document used to plan public expenditures over a multi-year horizon. It helps ensure the consistency and sustainability of investments and budget allocations in line with national development priorities.
6.8. Financial Flows
According to
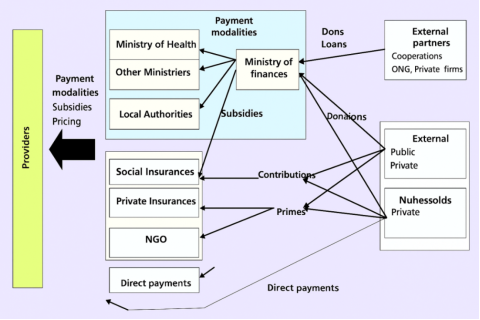
Figure 2 (below), the successful implementation of family planning and reproductive health (FP/RH) programs relies on the active engagement of a diverse set of stakeholders, each playing a distinct role in the mobilization and management of resources. Government institutions are responsible for shaping policy frameworks and allocating funding. TFPs contribute through specialized expertise and financial support. Civil society organizations advocate for human rights and equitable access to services, while communities play a crucial role in generating demand and participating in service delivery. When these actors work in concert, they foster stronger and more sustainable FP/RH systems that are responsive to the real needs of the populations they are intended to serve.
The Ministry of Finance plays a central role in fund management. It acts as a primary collection point, pooling resources from taxes, donations, and loans. These funds are then redistributed in the form of grants to support the financing of the health sector.
Households and businesses also contribute significantly to health financing. They are responsible for paying insurance contributions and premiums, thereby directly supporting the financing of healthcare services.
In addition, insurance companies and NGOs are involved in managing payments related to health services. Their role includes ensuring the effective implementation of reimbursement mechanisms, cost coverage, and financial support for beneficiaries. The
figure 2 below shows the financial flows.
Figure 2. Financial flows.
The financing of the health system relies on the coordinated contributions of several key.
Flow of Funds to Subnational Levels.
Table 6. Health Fund Disbursement and Expenditure Approval Procedures by Entity.
Entity | Health Fund Disbursement Procedure | Health Expenditure Approval Procedure |
Ministry of Health | Funds are allocated through the Revised Finance Law and disbursed following approval by the Ministry of Finance. | Expenditures are approved based on the priorities of the National Health Development Plan (PNDS) and aligned with the Priority Action Programs (PAP). |
Directorate of Financial Affairs | Manages and monitors budget execution through reports on mobilized funds and levels of implementation. | The Directorate of Financial Affairs ensures expenditure monitoring and compliance with the allocated budget. |
Technical and Financial Partners (TFPs) | TFPs disburse funds based on agreements and conventions signed with the State and beneficiary projects. | Partners follow expenditure validation procedures involving accountability mechanisms and financial audits. |
Public Health Facilities | Health facilities receive grants after validation of documentation and objectives set by the relevantities. | Health facilities submit funding requests validated based on financial reports and performance indicators. |
6.9. Family Planning Financing by Stakeholder
Since 2012, Togo has undertaken a structured process to reposition FP, particularly through the development and implementation of successive National Action Plans. These initiatives aim to strengthen access to and utilization of FP services across the country. This process has evolved with the ongoing support of several TFPs.
Evaluations conducted on the various action plans have shown that resources mobilized for the implementation of family planning interventions come from diverse sources. These include the government, technical and financial partners, the private sector, local governments, and CSOs.
However, despite this diversity in funding sources, technical and financial partners remain the primary contributors to the financing of the Budgeted National Action Plans (PANBs). This reflects a significant dependence on external partners to ensure the effective implementation of the planned family planning interventions.
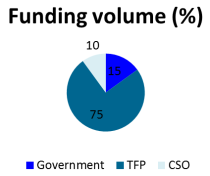
Figure 3. Funding Volume.
SRH Funding Volume and Trend Curve from
The current health financing structure in Togo reveals a strong dependence on TFPs, who account for 75% of available resources (
figure 3). This exposes the system to considerable risks related to the stability and sustainability of funding. This reliance underscores the urgency for the government to increase its investments particularly in FP through policies aimed at allocating a larger share of the national budget to health, thereby enhancing the sector’s autonomy and resilience.
Although CSOs contribute only 10% of the funding, their role is strategic in ensuring the relevance and effectiveness of interventions at the community level. It is therefore essential to provide them with greater financial and technical support to maximize their impact.
In sum, a more balanced distribution of contributions among the government, TFPs, and CSOs is crucial to ensuring sustainability, effectiveness, and broader coverage of health services in Togo.
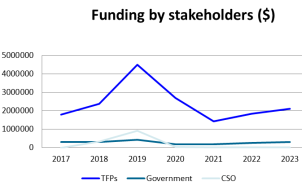
The reliance of SRH /FP on external funding exposes the sector to significant volatility, particularly during times of crisis (
figure 4). While the government’s financial commitment has remained stable, it is still insufficient to ensure long-term autonomy. At the same time, the role of CSOs remains marginal and unstable due to fluctuating resources.
Figure 4. Funding Trend Curve.
Source: Final Evaluation Report of the 2017-2022 Budgeted National Action Plan (PANB)
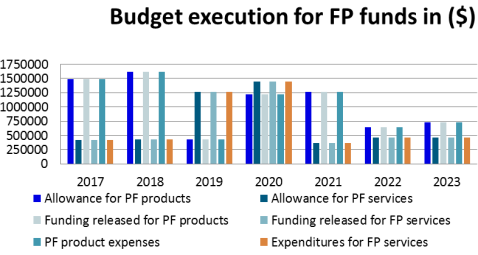
Between 2017 and 2023, investments in FP in Togo benefited from exemplary budget execution, with utilization rates approaching 100%, reflecting rigorous resource management (
figure 5). After an increase in funding for FP products and services through 2018-2020, significant variability emerged, characterized by a sharp decline in allocations for products in 2019 and for services in 2021. This instability is likely attributable to dependence on external funding, shifts in political priorities, and the impact of the COVID-19 pandemic beginning in 2021, which redirected budgets towards the health response. Despite a slight rebound in 2023, funding remains below previous levels, underscoring the need for thorough analysis and a strategy to stabilize and sustainably strengthen resources allocated to family planning.
Figure 5. Budget Execution for Family Planning Funds.
6.10. Progress and Challenges in Access to Family Planning Services in Togo
Over the years, Togo has made notable advances in reproductive health and family planning. However, these achievements are accompanied by persistent structural and institutional challenges that require tailored responses to ensure equity and sustainability of services.
During the past decade, Togo has experienced significant progress in reproductive health, reflecting a gradual improvement in access to family planning and maternal health services.
Moreover, the rate of births attended by skilled personnel has markedly increased, rising from 61.5% in 2014 to 75.1% in 2023. This improvement indicates better medical supervision during childbirth and a reduction in associated risks.
Furthermore, coverage of emergency obstetric and neonatal care (EmONC) has dramatically expanded, increasing from 7.1% in 2014 to 59.4% in 2023. This major advancement in the management of obstetric emergencies contributes to reducing maternal and neonatal morbidity and mortality.
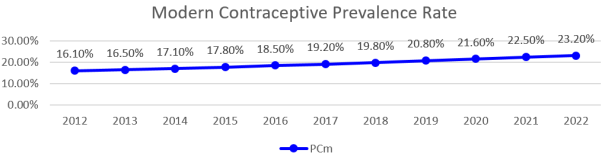
First, the modern contraceptive prevalence rate (mCPR) has significantly progressed, increasing from 17.1% in 2014 to 23.2% in 2023 (
Figure 6). This trend reflects growing adoption of modern contraceptive methods, indicating improved public awareness and increased availability of services.
Although the progression curve has not always been linear, it has shown steady growth since 2015. Nevertheless, there remains a need to accelerate or intensify interventions to meet demand effectively.
Figure 6. Modern Contraceptive Prevalence Rate.
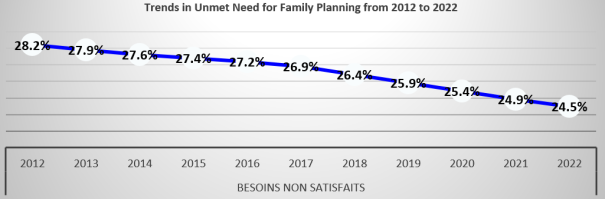
Unmet need for contraception refers to fecund women who are not using any contraceptive method but wish to delay their next birth (spacing) or who desire to have no more children at all (limiting).
Interventions carried out within the framework of the implementation of the 2017-2022 Budgeted National Action Plan (PANB) have contributed to improving the indicator related to unmet need for contraception.
According to data from the FP2030 indicator monitoring report, from 2016 to 2021, the unmet need steadily declined year after year, decreasing from 27.2% in 2016 to 24.5% in 2022, representing a reduction of nearly 3 percentage points, as illustrated in the
figure 7 below.
Figure 7. Unmet Need for FP.
7. Discussions
7.1. Study Limitations
This study presents several methodological and structural limitations. First, the sample, composed exclusively of institutional actors involved in the budgeting process (ministries of Health, Planning, Economy and Finance, NGOs), may not fully capture the breadth of perspectives, particularly those of field actors, civil society, or family planning service beneficiaries. Furthermore, data derived from semi-structured interviews may be influenced by respondents’ subjectivity or their institutional positions. Restricted access to certain sensitive or unpublished financial information also limits the scope of analysis, especially regarding financial flows and budget execution. Moreover, the quality of the analysis heavily depends on the reliability and currency of the documents reviewed during the documentary analysis. The variability of the political and economic context, which may shift budget priorities from year to year, also poses a constraint on the generalizability of results.
Another significant limitation lies in the exclusion of community participation, notably through Health Management Committees (COGES). Indeed, budgets stemming from self-financing at health centers, managed locally by COGES, represent a significant contribution to service operations, including family planning activities. The omission of these community resources in the budgetary analysis constitutes a blind spot that limits comprehensive understanding of actual grassroots financing. This also reduces the study’s ability to assess local engagement and co-financing dynamics that may strengthen service sustainability. For a more exhaustive analysis, future studies should incorporate community financial flows to more accurately reflect multisectoral efforts in family planning.
7.2. Innovation Points
The establishment of a dedicated budget line for FP in Togo represents a significant advancement in prioritizing reproductive health at the national level. This specific budget allocation serves as a strategic lever to enhance the visibility and traceability of funds earmarked for FP, thereby facilitating monitoring and advocacy efforts directed at policymakers. Moreover, this budgeting mechanism can serve as a model for other West African countries facing similar challenges in sustainable FP financing. Comparisons with countries such as Kenya and Ethiopia, which have implemented dedicated budget lines and have recorded notable improvements in modern contraceptive prevalence rates, underscore the potential of this Togolese innovation policymakers
. These countries have also demonstrated how targeted resource management fosters increased mobilization of domestic funds and optimizes expenditure efficiency.
7.3. Analysis of Family Planning Financing Trends
According to funding volume, data indicate that FP financing in Togo is largely dominated by TFPs, who provide 75% of the budget, followed by the Togolese government at only 15%, and CSOs at 10%. This funding structure reflects a strong dependence on external aid, which, although common in many sub-Saharan African countries, raises concerns regarding sustainability and financial autonomy.
Similar dependence is observed in several countries in the region. For example, according to UNFPA, most francophone West African countries rely on donor funding for over 70% of their FP programs. Burkina Faso, despite establishing a dedicated FP budget, still depends on TFPs for nearly 80% of contraceptive supplies. Nigeria, a more populous country with oil resources, shows slightly higher state commitment (approximately 25%) but remains reliant on external funding
| [16] | Gmakouba, W., Azianu, K. A., Kpakpassoko, N., Bini, M., Bantakpa, S. (2025). Evaluation of Pregnant Women's Satisfaction with Antenatal Care at Haho Health Zone Hospital Using the Erin Multi-attribute Model. Central African Journal of Public Health, 11(2), 62-69. https://doi.org/10.11648/j.cajph.20251102.13 |
[16]
.
This situation undermines long-term efforts, as TFP funds are often conditional, unstable, or project-cycle dependent. It also limits multiannual budget planning and complicates rapid responses to emerging needs, especially for adolescents and youth. Conversely, countries like Ethiopia and Kenya have progressively increased their domestic financing share (30-40%), enabling them to ensure more equitable and stable access to FP services even amid donor withdrawal or reallocation.
Therefore, to strengthen the resilience of its reproductive health system, Togo would benefit from gradually increasing state financing particularly by integrating FP into the health benefit package covered under universal health coverage mechanisms and mobilizing local resources, including through the COGES and local governments. This would not only enhance national ownership but also improve predictability and sustainability of FP interventions.
Regarding funding by actor, FP financing from 2017 to 2021 reveals strong reliance on technical and financial partners, who provide the majority of resources with a notable peak in 2019 followed by a significant decline in 2020 and 2021, likely due to the COVID-19 pandemic’s impact
. The government’s contribution remains low and relatively stable, with a slight peak in 2019, illustrating limited national financial ownership and marked dependence on external funding a common phenomenon in sub-Saharan countries
. Meanwhile, CSO funding is variable, with an increase in 2018-2019 followed by a sharp drop, often reflecting intermittent project-based support
. This financial structure, characterized by predominance of external funds, limited state participation, and unstable CSO support, is typical of the region and raises concerns about the sustainability of FP programs. The overall decline in funding in 2020-2021 highlights the sector’s vulnerability to global health crises, underscoring the need for governments to increase financial commitment, develop innovative mechanisms to diversify funding sources, and strengthen CSO involvement to ensure greater resilience and sustainability of family planning services
.
Regarding family planning budget execution, analysis of funding data from 2017 to 2021 shows a pattern of initial stability followed by significant year-to-year fluctuations. In 2017 and 2018, allocations, disbursements, and expenditures for FP products and services were perfectly aligned, reflecting consistent political commitment and budget management
| [4] | Direction de la Santé de la Mère et de l’Enfant et de la Planification Familiale (DSMIPF). (2023). Rapport annuel d’activités. |
| [7] | Ministère de la Santé du Togo. (2023). Rapport annuel de performance sectorielle. |
[4, 7]
. In 2019, a shift occurred with a significant reduction in product funding while allocations for services increased, possibly indicating strategic adjustment or financial constraints. The year 2020 marked a notable rebound (+57% compared to 2019), potentially influenced by increased needs related to the COVID-19 pandemic
. However, this increase was not sustained: in 2021, allocations dropped sharply, particularly for services, calling into question medium-term funding sustainability.
Compared to other sub-Saharan countries such as Kenya, Burkina Faso, or Senegal, Togo presents the particularity of institutionalizing a dedicated FP budget line, a significant progress
. However, absolute amounts allocated remain modest, and their instability reveals structural fragility. Countries like Kenya have secured FP financing through durable partnerships with international donors
| [21] | UNFPA. (2022). Etat des lieux du financement de la planification familiale en Afrique de l’Ouest francophone. Fonds des Nations Unies pour la Population. |
| [22] | United States Agency for International Development (USAID). (2023). Rapport de partenariat pour la planification familiale au Togo. |
[21, 22]
, improving service access and strengthening health systems
| [22] | United States Agency for International Development (USAID). (2023). Rapport de partenariat pour la planification familiale au Togo. |
[22]
. Conversely, Togo appears to rely more on its domestic budget, which, while indicative of some autonomy, makes funding more vulnerable to economic fluctuations. This dependence is compounded by the absence of sustainable financing mechanisms, recurring low political prioritization, and budget planning that does not always account for growing needs, especially of adolescents and youth
| [21] | UNFPA. (2022). Etat des lieux du financement de la planification familiale en Afrique de l’Ouest francophone. Fonds des Nations Unies pour la Population. |
[21]
. Moreover, the share of the national health budget dedicated to FP remains below 1%, a trend similar to the regional average and far below recommendations needed to achieve universal health coverage goals
.
Another point to highlight is the exclusion of community financing from the analysis, particularly funds mobilized by the COGES. These resources, though not budgeted at the subnational level, play a non-negligible role in the availability of FP products and services at health centers, especially in rural areas. Their absence from the analytical framework constitutes a limitation.
In conclusion, despite undeniable progress, Togo’s financial outcomes in family planning require strengthening multiannual planning, creating a dedicated national fund, and mobilizing local resources more effectively. It is also crucial to integrate monitoring and evaluation mechanisms for spending effectiveness and to encourage active community participation to ensure a lasting impact on reproductive health indicators and the reduction of maternal mortality.
7.4. Significant Dependence on External Funding
FP financing in Togo remains heavily reliant on TFPs, which fund approximately 82.3% of reproductive health programs. This dependence on international funding is primarily supported by organizations such as UNFPA, USAID, KfW, and WHO
| [22] | United States Agency for International Development (USAID). (2023). Rapport de partenariat pour la planification familiale au Togo. |
| [23] | United Nations Population Fund (UNFPA). (2021). State of World Population Report 2021: My Body is My Own. New York: UNFPA. |
| [24] | Kreditanstalt für Wiederaufbau. (2023). Appui à la santé reproductive et la planification familiale au Togo. |
[22-24]
. This funding model exposes the country to considerable risks, particularly due to possible shifts in priorities by these international partners, making program continuity vulnerable.
Only 1.3% of funding comes directly from the Togolese government’s budget, raising concerns about the sustainability of FP. This low level of domestic financing implies that any reduction or withdrawal of external aid could seriously compromise the country’s ongoing FP efforts.
However, it is important to note that the Togolese government has made a significant step by maintaining a dedicated budget line for FP since 2016, demonstrating political commitment to this cause. Nevertheless, although this commitment is essential, the allocated amount remains relatively insufficient, limiting the reach and impact of programs. Addressing this shortfall in domestic funding is crucial to ensure long-term stability of reproductive health initiatives.
7.5. Budget Allocation for Health Below International Commitments
Despite continuous efforts to improve financing in this critical sector, the health budget allocation in Togo remains inadequate. Indeed, the share of the national budget dedicated to health falls well short of the commitment made by African countries at the Abuja Declaration, which stipulates that 15% of national budgets should be allocated to health. Between 2019 and 2023, this share fluctuated between 6.2% in 2019 and 8.8% in 2023, remaining far below the target
| [8] | Ministère de la santé. (2023). Plan National de Développement Sanitaire 2023-2027. |
[8]
.
Furthermore, when compared to the WHO recommendations, Togo faces a significant gap. The WHO guidelines recommend spending at least USD 86 per capita to provide adequate basic health services. However, in 2023, per capita health expenditure remains well below this threshold
. Although the overall health budget doubled between 2019 and 2023, it is clear that funding needs greatly exceed current allocations, especially as Togo’s population continues to grow, thereby increasing demand for basic health services.
Thus, while progress is evident, the current budgetary situation does not satisfactorily meet the growing health sector needs in Togo. Increasing budget allocations and adopting more efficient fund management mechanisms are key challenges for improving health outcomes in the country.
The comparative analysis of FP budgets across the region reveals significant disparities. For instance, Kenya allocates approximately 3.5% of the national health budget to FP, whereas Togo, despite having a dedicated budget line, allocates a relatively modest share
. These figures highlight the urgent need to increase allocated resources and improve budget execution. Furthermore, stakeholder perspectives reveal major barriers particularly for youth including stigma, lack of tailored information, and limited access to services
| [26] | Chandra-Mouli, V., Camacho, A. V., & Michaud, P. A. (2013). WHO guidelines on preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. Journal of adolescent health, 52(5), 517-522. |
[26]
. These obtacles directly affect contraceptive demand and hinder coverage expansion. In response, it is critical to develop clear strategies, such as integrating family planning into universal health coverage schemes, to ensure sustainable financing and enhanced accessibility
| [20] | World Health Organization. (2022). Family planning/ Contraception. WHO. https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception |
| [27] | Gmakouba, W., Azianu, K. A., Bini, M., Bantakpa, S., Deabalo, P., et al. (2025). Progress and Prospects for the Institutionalization and Scale-Up of Postpartum Family Planning in Togo. American Journal of Health Research, 13(4), 210-225. https://doi.org/10.11648/j.ajhr.20251304.12 |
| [28] | World Health Organization (WHO). (2021). Domestic resource mobilization for sustainable family planning. WHO. |
[20, 27, 28]
. Integration within UHC would reduce out-of-pocket costs for users and promote more inclusive and equitable service delivery.
7.6. Persistent Challenges
Despite significant advances in family planning, persistent challenges hinder universal and equitable access to sexual and reproductive health services. These barriers undermine not only the effectiveness of interventions but also their long-term sustainability.
Firstly, adolescents and youth remain largely underserved, particularly regarding family planning. Due to their specific vulnerabilities, young people face difficulties accessing services tailored to their needs. This lack of access is exacerbated by social, cultural, and institutional barriers. In many contexts, youth experience stigma, misinformation about contraceptive methods, and lack of support from social and political actors, greatly limiting their ability to exercise reproductive health rights
| [21] | UNFPA. (2022). Etat des lieux du financement de la planification familiale en Afrique de l’Ouest francophone. Fonds des Nations Unies pour la Population. |
[21]
.
Moreover, rural areas continue to present major challenges for family planning access. In these regions, access to reproductive health services is severely limited. Health infrastructure is often inadequate, and the lack of qualified medical personnel remains a significant obstacle to delivering appropriate services. Additionally, the absence of proximity-based facilities such as mobile clinics or community health centers further hampers rural population coverage
.
Finally, stockouts of contraceptives remain a recurring problem. Although commitments have been made by the government and technical and financial partners to ensure continuous supply, these interruptions continue to weaken service continuity. Frequent contraceptive supply disruptions erode users’ trust in the health system, leading to reduced adherence to contraceptive methods and a return to riskier practices. This situation prevents comprehensive and reliable FP coverage
| [21] | UNFPA. (2022). Etat des lieux du financement de la planification familiale en Afrique de l’Ouest francophone. Fonds des Nations Unies pour la Population. |
[21]
.
Hence, despite progress, these challenges highlight the need for a holistic and coordinated approach involving improved infrastructure, targeted training for medical personnel, and strengthened contraceptive stock management to guarantee reliable family planning access for all.
7.7. Structural and Institutional Constraints
The challenges facing FP in Togo are largely exacerbated by structural and institutional constraints that hinder the effectiveness and sustainability of interventions. These barriers must be addressed in a targeted manner to ensure better reproductive health system performance over the long term.
On one hand, weak coordination between public and private actors remains a major obstacle. This lack of collaboration prevents the creation of effective synergies and limits complementary efforts in implementing interventions. The absence of coordination results not only in duplication of activities but also gaps in coverage of essential services. Indeed, private and public interventions often operate in isolation, leading to inefficient management of financial and human resources, negatively impacting service quality
| [21] | UNFPA. (2022). Etat des lieux du financement de la planification familiale en Afrique de l’Ouest francophone. Fonds des Nations Unies pour la Population. |
[21]
.
On the other hand, the lack of sustainable financing mechanisms poses a significant barrier to developing a resilient reproductive health system. Togo remains dependent on external funding, often irregular and unpredictable, which compromises medium- and long-term continuity of actions. This lack of stable internal resources impedes long-term planning and jeopardizes the sustainability of reproductive health programs. Without robust and predictable national financial mechanisms, the sustainability of FP interventions remains in question
| [1] | Organisation mondiale de la Santé (OMS). (2022). Investir dans la planification familiale: analyse des besoins en Afrique. Genève: OMS. |
[1]
.
7.8. Opportunities for Improvement
Despite the challenges and constraints, several opportunities exist to enhance the performance of the FP system in Togo. The country’s commitment to global initiatives such as FP2030 and the Ouagadougou Partnership represents a major opportunity for mobilizing both national and international resources. These partnerships help strengthen the coordination of efforts, promote the exchange of best practices, and support family planning in a more sustainable manner. Moreover, these initiatives are critical for ensuring effective monitoring of financial and technical commitments
| [16] | Gmakouba, W., Azianu, K. A., Kpakpassoko, N., Bini, M., Bantakpa, S. (2025). Evaluation of Pregnant Women's Satisfaction with Antenatal Care at Haho Health Zone Hospital Using the Erin Multi-attribute Model. Central African Journal of Public Health, 11(2), 62-69. https://doi.org/10.11648/j.cajph.20251102.13 |
[16]
.
Another opportunity lies in the development of innovative financing mechanisms. For instance, integrating family planning into existing health insurance schemes, such as Universal Health Insurance (AMU) and School AMU for School-Aged Children, could ensure broader and more equitable coverage of family planning services. This approach would not only diversify funding sources but also make reproductive health services more accessible to a wider population especially those in rural and marginalized areas
.
In addition, strengthening governance and accountability constitutes a strategic path to improve the management of resources allocated to FP. Engaging CSOs in the monitoring of public expenditures and health programs could serve as a powerful lever to ensure transparency and efficiency in the use of funds. Participatory governance and enhanced accountability in the management of human and financial resources could also reinforce citizens’ trust in public policies related to SRH
| [16] | Gmakouba, W., Azianu, K. A., Kpakpassoko, N., Bini, M., Bantakpa, S. (2025). Evaluation of Pregnant Women's Satisfaction with Antenatal Care at Haho Health Zone Hospital Using the Erin Multi-attribute Model. Central African Journal of Public Health, 11(2), 62-69. https://doi.org/10.11648/j.cajph.20251102.13 |
[16]
.
Finally, modernizing the legal framework is essential to ensure the sustainability of family planning efforts. Revising the 2007 Reproductive Health Law could create a robust and flexible legal foundation to facilitate resource allocation, funding management, and expansion of FP services. Legislative updates would also help ensure better coordination among public and private actors and adapt interventions to the country’s current demographic and social realities
.