Abstract
Introduction: This study evaluated the management of health and safety for Early Childhood Development (ECD) learners in Mufakose District, Zimbabwe. Ensuring the well-being of young learners is critical for their development, yet limited data exist on how effectively these standards are upheld in local educational settings. Methods: A descriptive survey design was employed, utilizing both qualitative and quantitative data collection methods. Data were gathered through interview guides and an observation checklist. Three primary schools—two government and one private—were randomly selected. From these schools, a purposive sample of 3 ECD teachers, 3 Teachers-in-Charge (TICs), and 3 school heads participated in the study. Results: Findings indicated that the health and safety practices in the sampled schools generally met the minimum operational standards. However, gaps were identified in areas such as staff training, infrastructure adequacy, and availability of safety resources. Factors influencing effective health and safety management included teacher qualifications and experience, teacher attitudes, resource constraints, and class size. Conclusion: The study concluded that while foundational health and safety measures are in place, significant improvements are needed to meet optimal standards. Recommendations include enhanced parental involvement, continuous professional development for ECD teachers and administrators on health and safety practices, and the implementation of robust performance monitoring frameworks.
Keywords
Early Childhood Development, Health and Safety Management, ECD Centres, Teacher Capacity, Mufakose District, School Infrastructure, Child Well-being
1. Introduction
Early childhood development (ECD) centers play a critical role in shaping children's health, safety, and long-term developmental outcomes
. However, in urban poor settings, many ECD centers struggle to meet minimum health and safety standards, leading to preventable diseases, injuries, and suboptimal learning environments
| [2] | Nziramasanga, C. T. (1999). Report of the presidential commission of inquiry into education and training. Harare: Government Printers. |
[2]
. In Zimbabwe, only 39% of ECD centers comply with basic health and safety requirements, exacerbating risks for young children
| [2] | Nziramasanga, C. T. (1999). Report of the presidential commission of inquiry into education and training. Harare: Government Printers. |
[2]
. Despite the introduction of Statutory Instrument 106 in 2005 to regulate ECD health and safety, enforcement remains weak due to inadequate monitoring, resource constraints, and poor infrastructure
. This study examines health and safety management in ECD centers within Mufakose District, Zimbabwe, assessing current practices, support systems, influencing factors, and potential improvement strategies.
1.1. Health and Safety Challenges in ECD Centers
Globally, significant progress has been made in improving primary education access
| [4] | Raikes, A., Rao, N., Yoshikawa, H., Cohrssen, C., Behrman, J., Cappa, C., Devercelli, A., Lopez Boo, F., McCoy, D., Richter, L.; (2023). Harnessing the power of global data to support young children’s learning and development research group. Global tracking of access and quality in early childhood care and education. Int J Child Care Educ Policy. 17(1): 14. https://doi.org/10.1186/s40723-023-00116-5 |
[4]
, yet health and safety in ECD settings—particularly in urban poor areas—remain underprioritized. Many centers lack adequate water, sanitation, and hygiene (WASH) facilities, with pupil-to-toilet ratios far below the recommended standard of one squat hole per 12 children [
. Poor sanitation increases diarrheal diseases, while inadequate infrastructure raises injury risks
| [5] | UNICEF. (2008). Evaluation of the national early childhood development programme. Harare: Ministry of Education |
[5]
. Girls face additional vulnerabilities due to insufficient gender-sensitive facilities, further compromising their safety and attendance
| [4] | Raikes, A., Rao, N., Yoshikawa, H., Cohrssen, C., Behrman, J., Cappa, C., Devercelli, A., Lopez Boo, F., McCoy, D., Richter, L.; (2023). Harnessing the power of global data to support young children’s learning and development research group. Global tracking of access and quality in early childhood care and education. Int J Child Care Educ Policy. 17(1): 14. https://doi.org/10.1186/s40723-023-00116-5 |
[4]
.
Urbanization has intensified pressure on ECD centers, with overcrowded classrooms and insufficient resources failing to meet growing demand
| [6] | Barnett, C., Schulman, D. & Shore, M. (2014). Health and safety issues in education. Dublin Harper. |
[6]
. Rural ECD programs have received more attention, leaving urban poor settings understudied despite their unique challenges
| [7] | Runyowa, J. Podzo, B. Z., Kanyume, P. (2014). An Assessment of Nutritional Patterns in Early Childhood Centres in Zimbabwe: A Quest for Dietary Quality. Journal of Education and e-Learning Research. http://asianonlinejournals.com/index.php/JEELR |
[7]
. In Mufakose District, resource limitations, weak policy implementation, and fragmented monitoring systems hinder effective health and safety management
| [8] | Pelletier, D., Neuman, M. J., Ann, N. Y. (2013). Advancing the nutrition and early childhood development agenda: indicators and guidance. Acad Sci. 232-44. https://doi.org/10.1111/nyas.12288 |
[8]
.
1.2. Theoretical Framework: The Donabedian Model
This study employs the Donabedian model
to evaluate health and safety management through three pillars: structure, process, and outcome.
1) Structure refers to institutional resources, including infrastructure, staffing, and policies
. In ECD centers, this encompasses classroom safety, WASH facilities, and teacher-to-child ratios.
2) Process examines how health and safety measures are implemented, including teacher training, hygiene practices, and emergency preparedness
| [10] | Majoko, T. (2018). Teachers’ Concerns about Inclusion in Mainstream Early Childhood Development in Zimbabwe. International Journal of Special Education. Vol.33, No.2. |
[10]
.
3) Outcome assesses the impact on child health, such as reduced injury rates and disease prevalence
| [11] | Ministry of Primary and Secondary Education, Zimbabwe. (2015). Curriculum Framework for Primary and Secondary Education 2015-2022. Harare, Government printers. |
[11]
.
Effective structures and processes should yield positive outcomes, yet many ECD centers in Zimbabwe lack this alignment due to systemic gaps
| [12] | UNICEF. (2011). Defining quality in education. A paper presented by UNICEF at the meeting of The International Working Group on Education. Florence, Italy/New York: UNICEF. |
[12]
.
1.3. Current Health and Safety Practices
ECD centers globally are expected to adhere to safety standards, including first-aid availability, safe play areas, and fire evacuation plans
| [5] | UNICEF. (2008). Evaluation of the national early childhood development programme. Harare: Ministry of Education |
[5]
. However, in Mufakose, many centers lack child-friendly furniture, clean water, and proper ventilation
| [12] | UNICEF. (2011). Defining quality in education. A paper presented by UNICEF at the meeting of The International Working Group on Education. Florence, Italy/New York: UNICEF. |
[12]
. Nutrition is another critical yet neglected area, with many urban poor children lacking access to balanced meals, increasing malnutrition risks
| [7] | Runyowa, J. Podzo, B. Z., Kanyume, P. (2014). An Assessment of Nutritional Patterns in Early Childhood Centres in Zimbabwe: A Quest for Dietary Quality. Journal of Education and e-Learning Research. http://asianonlinejournals.com/index.php/JEELR |
[7]
.
Teacher training in health and safety is inconsistent, with many educators unaware of universal precautions for disease prevention
| [13] | Dyanda, C., Makoni, R., Mudukuti, A., & Kuyanana, A. (2005). Evaluation of the National Early Childhood Development Programme. Harare, Government Printers. |
[13]
. Outdoor safety measures—such as fencing and helmet use—are rarely enforced, increasing injury risks
| [14] | Dhlomo, T. (2011). Integrating early childhood development education into mainstream primary school education in Zimbabwe: Implications to water, sanitation and hygiene delivery. Journal of African Studies, 3(7). |
[14]
. Contaminated water sources further exacerbate health threats, contributing to absenteeism
| [15] | Magnuson, K. A., Waldfogel, J. (2005) Early childhood care and education: effects on ethnic and racial gaps in school readiness. Future Child. Spring;15(1): 169-96. https://doi.org/10.1353/foc.2005.0005 |
[15]
.
1.4. Support Systems and Barriers
Effective health and safety management requires robust support systems, including policy enforcement, funding, and supervision
| [8] | Pelletier, D., Neuman, M. J., Ann, N. Y. (2013). Advancing the nutrition and early childhood development agenda: indicators and guidance. Acad Sci. 232-44. https://doi.org/10.1111/nyas.12288 |
[8]
. However, Zimbabwe’s economic challenges have strained education budgets, leaving ECD centers under-resourced
| [6] | Barnett, C., Schulman, D. & Shore, M. (2014). Health and safety issues in education. Dublin Harper. |
[6]
. Monitoring frameworks are weak, and many school administrators lack ECD-specific training, reducing compliance with safety standards
| [16] | Ayasi, R. A. (2003). Put Children First: for Every Child Health, Education, Equity, protection: Advance Humanity. Harare: UNICEF |
[16]
.
Teacher attitudes and knowledge significantly influence safety practices
| [17] | Vartuli, S., Rohs, J. (2009). Early Childhood Prospective Teacher Pedagogical Belief Shifts Over Time. Journal of Early Childhood Teacher Education 30(4): 310-327. https://doi.org/10.1080/10901020903320262 |
[17]
. Negative attitudes toward health protocols and overcrowded classrooms further hinder effective management
| [18] | Burton, D., & Bartlett, S. (2009). Key issues for Educational Researchers. Los Angeles, Sage Publications, Inc. |
[18]
.
1.5. Strategies for Improvement
To enhance health and safety, ECD centers should adopt integrated approaches such as:
1) The SABER-ECD Framework: A systems-based tool for evaluating and improving ECD policies
| [8] | Pelletier, D., Neuman, M. J., Ann, N. Y. (2013). Advancing the nutrition and early childhood development agenda: indicators and guidance. Acad Sci. 232-44. https://doi.org/10.1111/nyas.12288 |
[8]
.
2) Complex Adaptive Systems: A model for understanding school-level challenges and tailoring interventions
| [10] | Majoko, T. (2018). Teachers’ Concerns about Inclusion in Mainstream Early Childhood Development in Zimbabwe. International Journal of Special Education. Vol.33, No.2. |
[10]
.
3) Community and Stakeholder Engagement: Involving parents and local authorities in safety initiatives
| [11] | Ministry of Primary and Secondary Education, Zimbabwe. (2015). Curriculum Framework for Primary and Secondary Education 2015-2022. Harare, Government printers. |
[11]
.
This study addresses a critical gap in understanding health and safety management in urban poor ECD centers. By evaluating current practices, systemic barriers, and improvement strategies, it aims to inform policies that enhance child well-being in Mufakose District and similar settings.
2. Methods
2.1. Study Setting
This study was conducted in Mufakose District, a high-density urban suburb located in Harare, Zimbabwe. Mufakose is characterized by socioeconomic challenges, including overcrowding, inadequate infrastructure, and limited access to basic services such as clean water and sanitation
| [19] | Statutory Instrument 106 of (2015). [CAP 25: 04]. Education (Early Childhood Development Centres) Regulations. Harare: Government Printers. |
[19]
. The district’s ECD landscape consists of 14 primary schools (10 public and 4 private), all of which offer ECD programs.
The total ECD enrollment across these schools averages 950 learners, supported by 30 ECD teachers and 14 school heads. Class sizes often exceed recommended teacher-to-pupil ratios due to resource constraints, with some classrooms accommodating 40–50 children
| [20] | Chikwature, W., & Oyedele, V. (2016). ‘The Effectiveness of Guidance and Counseling in Teaching Learning Process at Gomorefu High School in Mutare District’. International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 5, |
[20]
. Many schools lack sufficient WASH (Water, Sanitation, and Hygiene) facilities, with some failing to meet the national standard of one toilet per 12 learners
| [20] | Chikwature, W., & Oyedele, V. (2016). ‘The Effectiveness of Guidance and Counseling in Teaching Learning Process at Gomorefu High School in Mutare District’. International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 5, |
[20]
. Additionally, infrastructure challenges—such as poorly maintained buildings, inadequate ventilation, and unsafe play areas—further compromise health and safety standards
| [12] | UNICEF. (2011). Defining quality in education. A paper presented by UNICEF at the meeting of The International Working Group on Education. Florence, Italy/New York: UNICEF. |
[12]
.
Mufakose’s urban poor setting presents unique challenges, including food insecurity, limited healthcare access, and high disease prevalence
| [7] | Runyowa, J. Podzo, B. Z., Kanyume, P. (2014). An Assessment of Nutritional Patterns in Early Childhood Centres in Zimbabwe: A Quest for Dietary Quality. Journal of Education and e-Learning Research. http://asianonlinejournals.com/index.php/JEELR |
[7]
. These factors make it an important case study for assessing health and safety management in resource-constrained ECD environments.
2.2. Research Design
A descriptive survey design employing both qualitative and quantitative approaches was adopted to gain comprehensive insights into health and safety management in ECD centres. This mixed-methods approach enabled triangulation of data, capturing both numerical trends and rich narratives. Descriptive surveys are suitable for exploring opinions, practices, and contextual realities, making them appropriate for evaluating school-level safety management
| [21] | Chireshe, R. (2013). The state of inclusive Education in Zimbabwe: Bachelor of Education (SNE) students` Perception. Journal of Social Science, 34(3). pp22. |
[21]
.
Three schools (two public, one private) were randomly selected to represent institutional diversity. Data collection involved open- and closed-ended interview questions and structured observation tools. This facilitated an in-depth evaluation of perceptions, support systems, and infrastructure in ECD centres.
2.3. Study Population
The study population comprised ECD teachers, Teachers-in-Charge (TICs), and school heads in Mufakose District.
2.4. Sampling and Sample Size
A total of three schools (Mutiunokura primary, Budiriro1 primary school and Rainbow primary school) were randomly selected to ensure proportional representation and reduce selection bias. From these, nine participants were purposively sampled (3 school heads, 3 TICs, and 3 ECD teachers). This small yet diverse sample aligns with qualitative research expectations where depth is prioritized over breadth. Inclusion criteria were willingness to participate, relevant professional roles, and availability. Ill or non-consenting individuals were excluded.
2.5. Research Instruments
2.5.1. Interview Guide
Semi-structured interviews were used and allowed participants to express nuanced views while ensuring consistency across interviews. The guide included six questions derived from study objectives focusing on effectiveness of support systems, influencing factors, and improvement strategies. Interviews were audio-recorded and conducted individually to maintain response integrity.
2.5.2. Observation Guide
Structured observations assessed compliance with national and international health and safety standards in ECD settings. Key indicators—such as sanitation, classroom safety, and playfield condition—were rated using a 4-point Likert scale. A score of 80% was considered the benchmark for compliance. The same observer (the researcher) conducted all assessments to ensure consistency and reduce inter-rater bias.
2.6. Validity, Reliability, and Trustworthiness
Instrument validity was ensured through expert review and alignment with study objectives. Reliability was enhanced via pre-testing in a non-participating school to refine question clarity and consistency. For qualitative data, trustworthiness was addressed through triangulation, peer debriefing, and an audit trail.
Credibility was established by using multiple data sources and ensuring consistency in procedures. Transferability was facilitated by selecting diverse schools. Dependability and confirmability were ensured through transparent documentation of data collection and analysis processes, with audio recordings enhancing data accuracy.
2.7. Data Collection Procedure
Data were collected over scheduled visits between 10:00 a.m. and 12:00 p.m. at each school. Individual interviews with ECD teachers, TICs, and school heads were conducted in private settings to encourage openness. Observation checklists were used to assess indoor and outdoor safety features, and findings were recorded in real-time.
2.8. Data Analysis
Quantitative data from closed-ended questions were analyzed using descriptive statistics (frequencies and percentages). Cross-tabulations explored relationships between variables. Qualitative data from interviews and open-ended responses were analyzed thematically. Thematic analysis followed Braun and Clarke’s phases: familiarization, coding, theme development, and interpretation
| [22] | Clarke, V. & Braun, V. (2013) Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. The Psychologist, 26(2), 120-123 |
[22]
.
2.9. Ethical Considerations
The study adhered to ethical standards based on beneficence, respect, and justice. Institutional permission was obtained, and written informed consent was secured from participants. Participation was voluntary, and respondents were informed of their right to withdraw at any time. Confidentiality and anonymity were maintained using coded identifiers. Interview recordings and transcripts were securely stored. Participants received detailed information sheets and signed consent forms. The researcher also presented official letters of permission from the Ministry of Primary and Secondary Education (MoPSE) and the Zimbabwe Open University. To ensure privacy, participants were not required to disclose identifying information. Anonymity was maintained through coding, and confidentiality was protected by securing data in a locked location accessible only to the researcher. No sensitive or intrusive questions were asked, and participants were not exposed to any physical or emotional risk. Ethical protocols ensured that data collection was respectful and non-disruptive.
3. Results
Data was gathered from school heads, ECD teachers and TICs of three selected schools in Mufakose district. Data were presented, analysed focusing on the extent to which safety and health is provided in ECD learning environment in Mufakose district.
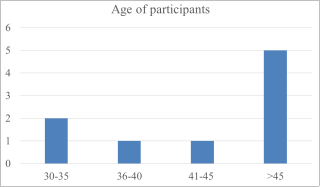
Figure 1. Age of participants.
3.1. Biographic Data of Participants
The participants’ ages ranged from 32 to 61 years, with a mean age of 46 years. Two participants (22.2%) were within the 30–35 age range, one participant (11.1%) was between 36–40 years, and another (11.1%) was aged 41–45 years. The majority of participants (5; 55.6%) were above 45 years (
Figure 1).
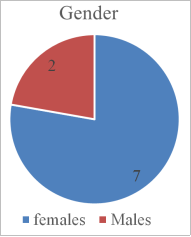
Study participants were predominantly females 7(77.8%) and only 2 (22.2%) of the participants were male (
Figure 2).
Figure 2. Gender of participants.
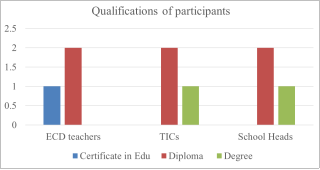
The qualifications of the participants ranged from Certificate in Education to Degree in Education. The majority of the participants 6(66.7%) had a Diploma in Education as their highest qualification whereas 1(11.1%) had a certificate in education and 2(22.2%) were degreed educators (
Figure 3).
Figure 3. Qualification of participants.
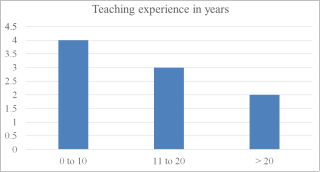
Experience in education ranged from 4 -25 years with a mean of 13 years. Of the three categories of participants that is ECD teachers, TICs, and School heads, the ECD teachers were on average the least experienced in the education fraternity. The least experience ECD teachers had an experience of 4 years and the most experienced ECD teacher had 12 years in the teaching field. Similarly, the least experience TIC had 10 years of experience whereas the most experienced TIC had 22 years in the teaching field. For school heads, the least experience head had 10 years in the field of teaching whereas the most experience head had 25 years of teaching experience.
Figure 4 below is an outline of the findings on the experience of the participants in teaching (
Figure 4).
Figure 4. Participants’ teaching experience.
3.2. Health and Safety Practices in ECD Schools in Mufakose District
Health and safety practices in ECD were assessed at three schools namely Mutiunokura primary, Budiriro1 primary school and Rainbow primary school respectively on the current health and safety All the three schools, reached the minimum threshold of health and safety in ECD centres as highlighted by overall school of 86.7%, 80.5% and 93.7% respectively practices (
Table 1).
Table 1. Scores on Health and safety practices in ECD schools.
Variable | School A | School B | School C |
Health and safety practices |
Phone numbers to report child abuse and neglect (Child Protective Services) are clearly posted where any adult can easily see them | 4 | 4 | 4 |
A Fire extinguisher are inspected annually. Check date on fire extinguisher tag | 4 | 4 | 4 |
Existence of fire exits and fire assembly places | 4 | 4 | 4 |
First aid supplies are well-stocked in each location where children spend time | 4 | 3 | 4 |
First aid supplies are kept in a closed container, cabinet or drawer that is labeled. They are stored out of children’s reach and within easy reach of staff | 3 | 3 | 4 |
There is fresh air provided by windows or a ventilation system. | 4 | 4 | 4 |
All electrical outlets within children’s reach are tamper resistant or have safety covers | 4 | 4 | 4 |
Plastic bags, matches, candles and lighters are stored out of children’s reach. | 4 | 4 | 4 |
Children do not play in areas where there is a body of water unless a caregiver/teacher is within an arm’s length providing “touch supervision”. Bodies of water include tubs, pails, sinks, toilets, swimming pools, ponds, irrigation ditches, and built-in wading pools. | 2 | 2 | 3 |
Equipment and play areas (including water play areas) do not have the following: sharp points or corners; splinters; glass; protrusions that may catch a child’s clothing | 2 | 2 | 3 |
Equipment and furnishings are sturdy and in good repair. There are no tip-over or tripping hazards. | 3 | 3 | 3 |
Outdoor play areas are enclosed with a fence or natural barriers that allow caregivers/teachers to see children. Openings in fences and gates are no larger than 9 cm | 4 | 4 | 4 |
Each gate has a latch that cannot be opened by children. Outdoor exit gates are equipped with self-closing, positive latching closure mechanisms that cannot be opened by children | 3 | 3 | 4 |
Shade is provided outside (for example, trees, tarps, umbrellas). Children wear hats or caps with a brim to protect their faces from the sun if they are not in a shaded area. | 3 | 3 | 4 |
SUPERVISION, INTERACTION and ACTIVITY [support systems] | | | |
Caregivers/Teachers directly supervise children by sight and hearing at all times. This includes indoors, outdoors and when children are sleeping, going to sleep or waking up | 3 | 3 | 4 |
Caregivers/Teachers encourage positive behavior and guide children to develop self-control. Caregivers/Teachers model desired behavior. “Time out” is only used for persistent, unacceptable behavior. | 4 | 3 | 4 |
There is no physical or emotional abuse or maltreatment of a child. There is no physical punishment or threat of physical punishment of a child | 4 | 4 | 4 |
Caregivers/Teachers do not use threats or humiliation (public or private). There is no profane or sarcastic language. There are no derogatory remarks made about a child or a child’s family | 4 | 4 | 4 |
Nutrition practices | | | |
Drinking water is available, indoors and outdoors, throughout the day for children over 6 months of age | 4 | 3 | 4 |
A variety of nourishing foods is served at meals and snacks. Nourishing foods include fruits, vegetables, whole and enriched grains, protein and dairy | 4 | 2 | 3 |
Children are always seated while eating | 3 | 3 | 4 |
The food preparation area of the kitchen is separate from eating, play, laundry, toilet, bathroom, and diapering areas. No animals are allowed in the food preparation area | 3 | 3 | 4 |
The food preparation area is separated from child care areas by a door, gate, counter, or room divider. | 4 | 3 | 4 |
Kitchen equipment is clean and in working order. Food surfaces are in good repair and free of cracks and crevices. Food surfaces are made of non-porous, smooth material and are kept clean and sanitized | 4 | 3 | 4 |
All fruits and vegetables are washed thoroughly with water prior to use | 4 | 4 | 4 |
SANITATION: Personal Hygiene, Environmental Health | | | |
Notices for moments or situations for hand washing are displayed in strategic places | 4 | 4 | 4 |
Caregivers/Teachers help children wash their hands when children can stand but cannot wash their hands by themselves. Children’s hands hang freely under the running water either at a child level sink or at a sink with a safety step | 3 | 3 | 4 |
Adults and children only use alcohol-based sanitizers as an alternative to handwashing with soap and water, if hands are not visibly soiled. Hand sanitizers are only used for children over 24 months with adult supervision | 3 | 4 | 3 |
There are enough squat holes for both boys and girls in the toilets according to the universal minimum standards | 2 | 2 | 3 |
There are enough sanitary facilities and portable clean water for both boys and girls for drinking and for washing hands | 3 | 2 | 3 |
There are no cracks or holes in walls, ceilings, floors or screens | 3 | 3 | 4 |
Infectious waste (for example soiled diapers, blood) and toxic waste (for example, used batteries, fluorescent light bulbs) are stored separately from other waste | 4 | 3 | 3 |
Overall score (out of 128) | 111 (86.7%) | 103 (80.5%) | 120 (93.8%) |
TIC from one school, “The school is promoting clean environment and repairing all damaged material and furniture.
3.3. Effectiveness of the Support Systems for Health and Safety in ECD Centres
All the 9 respondents responded to the question on the effectiveness of the support systems for health and safety in ECD centres.
A T. I. C in school B which was a government school said:
“The education system suffers from lack of financial resources and human capital for effective monitoring of health and safety in ECD programmes”.
An ECD teacher from school A had this to say:
“Some ECD teachers in the urban setting, feel they are not fully supported for effective implementation of health and safety as they working environment is often poorly lighted with inadequate sanitary facilities to obtain optimal health and safety for both learners and teachers”
The school head of Mutiunokura Primary School highlighted economic instability, inflation, and limited resources as major challenges affecting the provision of effective support for compliance with health and safety requirements in ECD programmes within urban poor settings. At School B, ECD teachers cited a high teacher–pupil ratio, with classes averaging 50 learners, as a key challenge in monitoring the health practices of each child and supervising their play activities. This high ratio was linked to the occurrence of contagious skin conditions and injuries, often resulting from unsupervised or unsafe play. Additionally, due to financial constraints, schools reported difficulties in consistently supporting medical check-ups for ECD teachers, which are essential for ruling out chronic infections. The TIC for school C had this to say with regards to the monitoring systems:
“To date the education system has not provided clear monitoring and evaluation frameworks specifically for health and safety in ECD centres resulting in fragmented approaches to supportive supervision and evaluation of health and safety in our schools”.
When asked on the state of supportive supervision at the school one of the head said:
“We are often overwhelmed with work to effectively supervise the teachers. Our schools are not adequately resources to always meet the minimum standards of cleanliness and safety in the ablution facilities and safety of learners in indoors and out-door learning activities.”
3.4. Factors That Influence the Management of Health and Safety in ECD Centres
This study also sought to answer the following research question: What are the factors that influence the management of health and safety in ECD centres in Mufakose District?
Headmasters, TICs and teachers were asked on the factors that the perceive influence, health and safety in ECD centres. ECD knowledge base which constitute of professional competencies, abilities and specific teaching skills were cited as influencing factors to effective management of health and safety in ECD centres.
The headmistress for school C had this to say:
“Teacher’s level of knowledge and experience is directly linked with the level of health and safety that the ECD learners experience in indoor and out-door learning environments. Also ECD teachers, young and old portray different attitudes towards learners and that is likely going to affect how they respond to health and safety matters in ECD centres”.
The TIC for school B cited the lack of continual training for both teachers and school administrators on health and safety as a big challenge in effective health and safety management in primary schools in Zimbabwe and related negative attitudes to poor understanding of health and safety matters in ECD centres.
The TIC for school A mentioned classroom size coupled with limited space indoors and outdoors as key factors in the management of health and safety of ECD learners in ECD centres.
3.5. Possible Strategies to Improve Health and Safety Management in ECD Centres in Mufakose District
This study sought to determine the possible strategies that can be employed to improve health and safety management in ECD centres in Mufakose District. The participants suggested a couple of strategies to improve health and safety in ECD centres in Mufakose District. Parental involvement was cited as a critical component for effective health and safety in ECD centres. This recommendation was consistent across the three schools. Active and meaningful involvement of parents was reported to the critical for buy-in and resource mobilisation.
The TICs and school heads made a recommendation that the Ministry of Primary and Secondary education invest and fully support the monitoring and evaluation frameworks for ECD education to improve quality of service delivery. This can be done through the use of supportive supervision teams at different levels that receive continual training of effective supportive supervision and evaluation of health and safety indicators in ECD centres. Such support could also continually provided to school administrators as recommended in other studies in the region
| [11] | Ministry of Primary and Secondary Education, Zimbabwe. (2015). Curriculum Framework for Primary and Secondary Education 2015-2022. Harare, Government printers. |
[11]
.
There was a general consensus among the interviewed educators that innovative ways of enhancing the school support systems should be employed by schools to fund health and safety activities. This include effective use of parents’ days to mobilize parents and raise awareness of their need to full fund health and safety matters.
Similarly, a gap was reported by all participants in fostering inclusivity due to several factors including issues of resources and lack of competencies among ECD educators and administrators.
4. Discussion
This study was motivated by the researcher’s observations during teaching practice, which revealed that health and safety standards in ECD learning environments were generally below the minimum requirements set for ECD centres in Zimbabwe. The research sought to contribute to the effective implementation of ECD programmes. However, it was constrained by limited time and financial resources, which hindered the researcher from collecting additional information that could have strengthened the study. The COVID-19 pandemic further exacerbated these constraints by restricting travel and in-person engagement with educators. Additional costs were incurred to facilitate virtual follow-ups, including the provision of data bundles to interviewees.
Findings revealed that ECD educators and supervisors are predominantly older adults. School heads were the oldest, with the youngest aged 53 years, followed by TICs (youngest 38 years), and ECD teachers (youngest 32 years). This indicates a need to attract and motivate younger educators into the field, especially given the demands of Zimbabwe's new curriculum, which emphasizes energy, innovation, and adaptability. These findings align with a similar study
| [23] | Bruce, T., Meggit, C. & Greiner, J. (2013). Child care and education. London: Hodder Education |
[23]
.
A significant gender disparity was also noted: all ECD teachers and TICs were female, while two of the three school heads (66.7%) were male. This reflects entrenched gender stereotypes that associate caregiving roles with women and leadership roles with men. As Myers suggests, societal perceptions continue to influence leadership representation in early childhood education
| [24] | Myers, R. G. (2004). In search of quality in programmes of Early Childhood Care and Education (ECCE). A paper prepared for the 2005 EFA Global Monitoring Report 2005. Paris: UNESCO. |
[24]
. The advancement of feminist leadership principles may encourage more women to aspire to and occupy leadership roles.
Regarding qualifications, ECD teachers were the least qualified, followed by TICs and school heads. Only one school head held a Master’s degree. The study emphasizes the importance of continued professional development for all categories of educators. As Walters notes, teacher qualifications and experience are critical for the effective integration of health and safety practices in early learning environments
| [25] | Walters, D. (2003). Workplace Arrangements for Occupational Health and Safety in the 21st Century, School of Social Sciences, Cardiff University, United Kingdom. |
[25]
.
All participants demonstrated a good understanding of health and safety principles in ECD contexts. School heads were particularly knowledgeable about relevant government policies. These findings support a similar assertion that experience in ECD enhances the adoption of developmentally appropriate health and safety practices
| [23] | Bruce, T., Meggit, C. & Greiner, J. (2013). Child care and education. London: Hodder Education |
[23]
.
Despite this awareness, the study found significant weaknesses in the management of children’s outdoor activities and personal hygiene. Inadequate indoor and outdoor space was cited as a major barrier to safety. According to UNICEF, ECD classrooms should allow for free movement, be equipped with safe, well-maintained furniture, and have proper fire exits and ventilation
| [5] | UNICEF. (2008). Evaluation of the national early childhood development programme. Harare: Ministry of Education |
[5]
. Only one of the three sampled schools had a health and safety policy and manual, despite global standards requiring such documents for effective risk management
| [13] | Dyanda, C., Makoni, R., Mudukuti, A., & Kuyanana, A. (2005). Evaluation of the National Early Childhood Development Programme. Harare, Government Printers. |
[13]
.
The private school in the study had sound nutrition policies and provided adequate meals to learners. Teachers in all schools understood the nutritional needs of preschoolers and created a relaxed, supportive feeding environment, in line with UNICEF recommendations. However, the lack of supplementary feeding programmes in public schools poses a serious risk of malnutrition, especially in urban poor settings like Mufakose. Malnutrition, both chronic and acute, weakens children's immunity and impedes growth and development
| [19] | Statutory Instrument 106 of (2015). [CAP 25: 04]. Education (Early Childhood Development Centres) Regulations. Harare: Government Printers. |
[19]
.
While the general school environments were relatively clean and safe, they were not adequately disability-friendly. None of the schools had appropriate toilet facilities or infrastructure to support learners with multiple disabilities. Effective support systems are vital for ensuring the health and well-being of all ECD learners, particularly those with special needs.
Interviews with participants revealed weak policy coordination and fragmented data and monitoring systems as major challenges in managing ECD health and safety. The comfort of the learning environment, which significantly influences teacher attitudes and practices, was used as a proxy measure of school support system effectiveness
| [19] | Statutory Instrument 106 of (2015). [CAP 25: 04]. Education (Early Childhood Development Centres) Regulations. Harare: Government Printers. |
[19]
.
Robust administrative oversight is essential for monitoring school compliance and establishing operational standards for health and safety
| [13] | Dyanda, C., Makoni, R., Mudukuti, A., & Kuyanana, A. (2005). Evaluation of the National Early Childhood Development Programme. Harare, Government Printers. |
[13]
. Economic hardships, inflation, and limited resources were cited as major hindrances. Despite these challenges, schools must adopt innovative strategies to ensure safe learning environments. Ayasi recommends introducing infrastructure levies and other funding mechanisms to support health and safety initiatives
| [16] | Ayasi, R. A. (2003). Put Children First: for Every Child Health, Education, Equity, protection: Advance Humanity. Harare: UNICEF |
[16]
.
The lack of monitoring and evaluation frameworks with clear health and safety indicators was evident across the sampled schools. Effective support systems require adequate policy frameworks, continuous capacity-building, and resource allocation to meet the minimum standards for quality service delivery.
Participants also highlighted the lack of continuous training as a barrier to effective health and safety management. Armstrong identifies training as a critical pillar of preventive health and safety programming
| [26] | Armstrong, M. (2010). Armstrong’s Essential Human Resource Management Practice, a Guide to People Management, 12th edition. London: Kogan Page. |
[26]
. Ongoing professional development raises awareness and ensures that teachers stay up to date with best practices.
Another significant issue was overcrowded classrooms. With an average of 50 pupils per class, teachers struggled to monitor individual learners effectively. Health and safety can only be assured when teacher-to-pupil ratios are optimal and classroom space allows for proper supervision.
Inadequate infrastructure and skills gaps hindered full compliance with expected health and safety standards. Factors such as teacher qualifications, experience, attitudes, and class size were found to significantly influence effective management. These must be systematically monitored to ensure improvement across ECD centres in Mufakose District.
Finally, multiple studies affirm that creating disability-friendly environments is a cornerstone of health and safety in ECD centres. Armstrong underscores the importance of regular health and safety training as part of a school’s preventive strategy
| [26] | Armstrong, M. (2010). Armstrong’s Essential Human Resource Management Practice, a Guide to People Management, 12th edition. London: Kogan Page. |
[26]
. Training helps identify risks, reinforce rules, and reduce hazards in learning environments.
In line with Zimbabwe Statutory Instrument 106 instituted in 2005, which prescribes minimum standards for pupil-to-toilet and pupil-to-handwashing basin ratios, school heads and TICs acknowledged being overwhelmed by the current pupil numbers
| [20] | Chikwature, W., & Oyedele, V. (2016). ‘The Effectiveness of Guidance and Counseling in Teaching Learning Process at Gomorefu High School in Mutare District’. International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 5, |
[20]
. This makes it difficult to maintain hygiene and safety in both indoor and outdoor learning spaces. The participants called for a policy review by the Ministry of Primary and Secondary Education to address these challenges.
Study Limitations
The study faced the following limitations:
1) The sample size was relatively small and may not fully represent all ECD schools in urban poor settings across Zimbabwe. However, the primary aim of the study was not to generalize the findings, but rather to provide insight into the current status of a selected sample of schools in Harare.
2) Some participants were not available at the initially agreed times, leading to delays in data collection. To address this, the researchers scheduled follow-up appointments at the earliest possible convenience.
3) A few respondents appeared reluctant, hesitant, or shy to provide meaningful data. In such cases, the researcher exercised patience, maintained a respectful and encouraging tone, and explained the importance of their participation while assuring them of confidentiality and respect for their privacy.
4.1. Recommended Strategies to Improve Health and Safety in ECD Centres
1) Parental involvement was identified across all schools as a critical factor in promoting effective health and safety in ECD centres.
2) School heads should develop and implement comprehensive health and safety policies, accompanied by robust monitoring and evaluation frameworks to regularly assess the levels of health and safety management in ECD settings.
3) Teachers and school administrators should receive ongoing training on health and safety to enhance their awareness and responsiveness to emerging risks in ECD environments.
4) School heads and parent representatives should collaborate to explore innovative ways of strengthening school support systems, including mobilizing resources to fund health and safety activities.
5) The Ministry of Primary and Secondary Education, along with curriculum planners, should ensure that ECD centres are inclusive and disability-friendly to mitigate environmental risks for children with multiple disabilities.
6) Further research on health and safety in ECD centres is needed to build a more robust body of evidence to inform policy and practice.
4.2. Conclusion
This study assessed the effectiveness of health and safety management in ECD centres in Mufakose District, revealing that while minimum standards are generally met, significant gaps remain in areas such as sanitation, infrastructure, and outdoor supervision. Support systems were found to be weak, largely due to financial and human resource constraints. Strengthening collaboration between schools, the Ministry of Primary and Secondary Education, parents, NGOs, and other stakeholders is essential. Key influencing factors included educators’ qualifications, experience, knowledge, and ongoing training. The study recommends adopting clear monitoring and evaluation frameworks, promoting peer learning through exchange visits, and prioritizing health and safety in teacher training and school budgeting to enhance the overall wellbeing and development of children in ECD centres.
Abbreviations
DSI | District Schools Inspector |
ECD | Early Childhood Development |
FAO | Food and Agricultural Organisation |
MoPSE | Ministry of Primary and Secondary Education |
NGO | Non- Governmental Organisation |
TIC | Teacher In Charge |
UNICEF | United Nations International Children Emergency |
Author Contributions
Jane Mhlanga: Conceptualization, Investigation, Methodology, Writing – original draft
Maxwell Mhlanga: Formal Analysis, Methodology, Writing – review & editing
Sophie Hlatywayo: Supervision, Validation, Writing – review & editing
Funding
The study was not funded.
Conflict of Interest
The authors declare no conflicts of interest.
References
| [1] |
Likhar, A., Baghel, P., Patil, M. (2022). Early Childhood Development and Social Determinants. Cureus. 2022 Sep 23;14(9): e29500.
https://doi.org/10.7759/cureus.29500
|
| [2] |
Nziramasanga, C. T. (1999). Report of the presidential commission of inquiry into education and training. Harare: Government Printers.
|
| [3] |
Matjokana, T. N. M. (2021). Strengthening the implementation of Early Childhood Development policies to improve quality.
https://repository.up.ac.za/server/api/core/bitstreams/85e41d0e-85da-4a6d-8e5f-4091ea4750a9/content
|
| [4] |
Raikes, A., Rao, N., Yoshikawa, H., Cohrssen, C., Behrman, J., Cappa, C., Devercelli, A., Lopez Boo, F., McCoy, D., Richter, L.; (2023). Harnessing the power of global data to support young children’s learning and development research group. Global tracking of access and quality in early childhood care and education. Int J Child Care Educ Policy. 17(1): 14.
https://doi.org/10.1186/s40723-023-00116-5
|
| [5] |
UNICEF. (2008). Evaluation of the national early childhood development programme. Harare: Ministry of Education
|
| [6] |
Barnett, C., Schulman, D. & Shore, M. (2014). Health and safety issues in education. Dublin Harper.
|
| [7] |
Runyowa, J. Podzo, B. Z., Kanyume, P. (2014). An Assessment of Nutritional Patterns in Early Childhood Centres in Zimbabwe: A Quest for Dietary Quality. Journal of Education and e-Learning Research.
http://asianonlinejournals.com/index.php/JEELR
|
| [8] |
Pelletier, D., Neuman, M. J., Ann, N. Y. (2013). Advancing the nutrition and early childhood development agenda: indicators and guidance. Acad Sci. 232-44.
https://doi.org/10.1111/nyas.12288
|
| [9] |
Donabedian, A. (2005). Evaluating the Quality of Medical Care. The Milbank Quarterly Volume 83, Issue 4 pp. 691-729
https://doi.org/10.1111/j.1468-0009.2005.00397.x
|
| [10] |
Majoko, T. (2018). Teachers’ Concerns about Inclusion in Mainstream Early Childhood Development in Zimbabwe. International Journal of Special Education. Vol.33, No.2.
|
| [11] |
Ministry of Primary and Secondary Education, Zimbabwe. (2015). Curriculum Framework for Primary and Secondary Education 2015-2022. Harare, Government printers.
|
| [12] |
UNICEF. (2011). Defining quality in education. A paper presented by UNICEF at the meeting of The International Working Group on Education. Florence, Italy/New York: UNICEF.
|
| [13] |
Dyanda, C., Makoni, R., Mudukuti, A., & Kuyanana, A. (2005). Evaluation of the National Early Childhood Development Programme. Harare, Government Printers.
|
| [14] |
Dhlomo, T. (2011). Integrating early childhood development education into mainstream primary school education in Zimbabwe: Implications to water, sanitation and hygiene delivery. Journal of African Studies, 3(7).
|
| [15] |
Magnuson, K. A., Waldfogel, J. (2005) Early childhood care and education: effects on ethnic and racial gaps in school readiness. Future Child. Spring;15(1): 169-96.
https://doi.org/10.1353/foc.2005.0005
|
| [16] |
Ayasi, R. A. (2003). Put Children First: for Every Child Health, Education, Equity, protection: Advance Humanity. Harare: UNICEF
|
| [17] |
Vartuli, S., Rohs, J. (2009). Early Childhood Prospective Teacher Pedagogical Belief Shifts Over Time. Journal of Early Childhood Teacher Education 30(4): 310-327.
https://doi.org/10.1080/10901020903320262
|
| [18] |
Burton, D., & Bartlett, S. (2009). Key issues for Educational Researchers. Los Angeles, Sage Publications, Inc.
|
| [19] |
Statutory Instrument 106 of (2015). [CAP 25: 04]. Education (Early Childhood Development Centres) Regulations. Harare: Government Printers.
|
| [20] |
Chikwature, W., & Oyedele, V. (2016). ‘The Effectiveness of Guidance and Counseling in Teaching Learning Process at Gomorefu High School in Mutare District’. International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 5,
|
| [21] |
Chireshe, R. (2013). The state of inclusive Education in Zimbabwe: Bachelor of Education (SNE) students` Perception. Journal of Social Science, 34(3). pp22.
|
| [22] |
Clarke, V. & Braun, V. (2013) Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. The Psychologist, 26(2), 120-123
|
| [23] |
Bruce, T., Meggit, C. & Greiner, J. (2013). Child care and education. London: Hodder Education
|
| [24] |
Myers, R. G. (2004). In search of quality in programmes of Early Childhood Care and Education (ECCE). A paper prepared for the 2005 EFA Global Monitoring Report 2005. Paris: UNESCO.
|
| [25] |
Walters, D. (2003). Workplace Arrangements for Occupational Health and Safety in the 21st Century, School of Social Sciences, Cardiff University, United Kingdom.
|
| [26] |
Armstrong, M. (2010). Armstrong’s Essential Human Resource Management Practice, a Guide to People Management, 12th edition. London: Kogan Page.
|
Cite This Article
-
APA Style
Mhlanga, J., Mhlanga, M., Hlatywayo, S. (2025). Assessing Health and Safety Management in Early Childhood Development Centres: Evidence from Mufakose District, Zimbabwe. International Journal of Elementary Education, 14(3), 68-77. https://doi.org/10.11648/j.ijeedu.20251403.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Mhlanga, J.; Mhlanga, M.; Hlatywayo, S. Assessing Health and Safety Management in Early Childhood Development Centres: Evidence from Mufakose District, Zimbabwe. Int. J. Elem. Educ. 2025, 14(3), 68-77. doi: 10.11648/j.ijeedu.20251403.13
Copy
|
Download
AMA Style
Mhlanga J, Mhlanga M, Hlatywayo S. Assessing Health and Safety Management in Early Childhood Development Centres: Evidence from Mufakose District, Zimbabwe. Int J Elem Educ. 2025;14(3):68-77. doi: 10.11648/j.ijeedu.20251403.13
Copy
|
Download
-
@article{10.11648/j.ijeedu.20251403.13,
author = {Jane Mhlanga and Maxwell Mhlanga and Sophie Hlatywayo},
title = {Assessing Health and Safety Management in Early Childhood Development Centres: Evidence from Mufakose District, Zimbabwe
},
journal = {International Journal of Elementary Education},
volume = {14},
number = {3},
pages = {68-77},
doi = {10.11648/j.ijeedu.20251403.13},
url = {https://doi.org/10.11648/j.ijeedu.20251403.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijeedu.20251403.13},
abstract = {Introduction: This study evaluated the management of health and safety for Early Childhood Development (ECD) learners in Mufakose District, Zimbabwe. Ensuring the well-being of young learners is critical for their development, yet limited data exist on how effectively these standards are upheld in local educational settings. Methods: A descriptive survey design was employed, utilizing both qualitative and quantitative data collection methods. Data were gathered through interview guides and an observation checklist. Three primary schools—two government and one private—were randomly selected. From these schools, a purposive sample of 3 ECD teachers, 3 Teachers-in-Charge (TICs), and 3 school heads participated in the study. Results: Findings indicated that the health and safety practices in the sampled schools generally met the minimum operational standards. However, gaps were identified in areas such as staff training, infrastructure adequacy, and availability of safety resources. Factors influencing effective health and safety management included teacher qualifications and experience, teacher attitudes, resource constraints, and class size. Conclusion: The study concluded that while foundational health and safety measures are in place, significant improvements are needed to meet optimal standards. Recommendations include enhanced parental involvement, continuous professional development for ECD teachers and administrators on health and safety practices, and the implementation of robust performance monitoring frameworks.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessing Health and Safety Management in Early Childhood Development Centres: Evidence from Mufakose District, Zimbabwe
AU - Jane Mhlanga
AU - Maxwell Mhlanga
AU - Sophie Hlatywayo
Y1 - 2025/08/18
PY - 2025
N1 - https://doi.org/10.11648/j.ijeedu.20251403.13
DO - 10.11648/j.ijeedu.20251403.13
T2 - International Journal of Elementary Education
JF - International Journal of Elementary Education
JO - International Journal of Elementary Education
SP - 68
EP - 77
PB - Science Publishing Group
SN - 2328-7640
UR - https://doi.org/10.11648/j.ijeedu.20251403.13
AB - Introduction: This study evaluated the management of health and safety for Early Childhood Development (ECD) learners in Mufakose District, Zimbabwe. Ensuring the well-being of young learners is critical for their development, yet limited data exist on how effectively these standards are upheld in local educational settings. Methods: A descriptive survey design was employed, utilizing both qualitative and quantitative data collection methods. Data were gathered through interview guides and an observation checklist. Three primary schools—two government and one private—were randomly selected. From these schools, a purposive sample of 3 ECD teachers, 3 Teachers-in-Charge (TICs), and 3 school heads participated in the study. Results: Findings indicated that the health and safety practices in the sampled schools generally met the minimum operational standards. However, gaps were identified in areas such as staff training, infrastructure adequacy, and availability of safety resources. Factors influencing effective health and safety management included teacher qualifications and experience, teacher attitudes, resource constraints, and class size. Conclusion: The study concluded that while foundational health and safety measures are in place, significant improvements are needed to meet optimal standards. Recommendations include enhanced parental involvement, continuous professional development for ECD teachers and administrators on health and safety practices, and the implementation of robust performance monitoring frameworks.
VL - 14
IS - 3
ER -
Copy
|
Download