Duodenal vascular ectasia (DVE) is a rare but important cause of upper gastrointestinal bleeding, particularly in patients with chronic liver disease. Gastric antral vascular ectasia (GAVE) is a more commonly recognized vascular lesion associated with cirrhosis; however, vascular ectasia involving the duodenum is infrequently reported and may pose diagnostic and therapeutic challenges. We report a case of a cirrhotic patient presenting with recurrent upper gastrointestinal bleeding manifested as melena and progressive anemia. Initial evaluation suggested variceal bleeding; however, endoscopic examination revealed the presence of GAVE along with vascular ectasia involving the duodenal bulb and extending into the third part of the duodenum. Histopathological examination of duodenal biopsies demonstrated dilated vascular channels within the lamina propria, consistent with duodenal vascular ectasia. Endoscopic management was initially directed toward GAVE using argon plasma coagulation (APC). Due to persistent anemia and recurrent bleeding, APC therapy was subsequently applied to the duodenal vascular lesions with careful technique to minimize the risk of perforation. Hemostasis was successfully achieved without complications, and the patient showed sustained clinical improvement with stabilization of hemoglobin levels and no further transfusion requirement during follow-up. This case highlights duodenal vascular ectasia as a potential source of gastrointestinal bleeding in cirrhotic patients and demonstrates that argon plasma coagulation can be a safe and effective therapeutic modality when applied cautiously.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Tai DI, Chou FF, Lee TY, Lin CC. Vascular ectasia of the duodenum detected by duodenoscopy. Am J Gastroenterol. 1987; 82: 1071-1073.
[1]
and an uncommon cause of upper gastrointestinal bleeding. It has been associated with chronic systemic diseases such as aortic valve pathology and end-stage renal disease in patients undergoing long-term hemodialysis (2-4). Gallagher et al.
[5]
Gallagher C, Bonar F, Dempsey J, Crowe J. Small bowel capillary dilatation in portal hypertension. Postgrad Med J. 1985; 61: 541-543.
described a case of small bowel capillary dilatation in a cirrhotic patient, suggesting that such vascular changes may be specific to portal hypertension and could contribute to gastrointestinal hemorrhage. However, only a limited number of cases of duodenal vascular ectasia have been documented in patients with cirrhosis (5-7). Here, we report a case of upper gastrointestinal bleeding due to duodenal vascular ectasia in a cirrhotic patient, effectively treated with argon plasma coagulation (APC). It has been previously described in association with systemic disorders including aortic valve disease and renal failure
[2]
Weaver GA, Alpern HD, Davis JS, Ramsey WH, Reichelderfer M. Gastrointestinal angiodysplasia associated with aortic valve disease: part of a spectrum of angiodysplasia of the gut. Gastroenterology. 1979; 77: 1-11.
[4]
Cappell MS, Lebwohl O. Cessation of recurrent bleeding from gastrointestinal angiodysplasias after aortic valve replacement. Ann Intern Med. 1986; 105: 54-57.
An elderly male in early 60 was admitted with history of black colored stool, abdominal distension, bilateral feet swelling and generalized weakness since last 3 months. He visited the emergency room one year ago because of hematemesis, and an endoscopic examination revealed esophageal varices with bleeding, which were treated with endoscopic band ligation.
Physical examination revealed a distended abdomen with prominent shifting dullness.
The results of initial laboratory tests were as follows: white blood count (WBC) = 3900/mm3, hemoglobin = 7.1 g/dL, platelets = 54 000/mm3, prothrombin time =21.8 s, international normalized ratio = 1.8, total bilirubin= 1.9 mg/dL, direct bilirubin = 1 mg/dL, protein = 5.13 g/dL, albumin =2.73 g/dL, alanine aminotransferase = 58 IU/L, aspartate aminotransferase = 52 IU/L, gamma-glucuronyl transferase = 40 IU/L, alkaline phosphatase = 93 IU/L, glucose = 98 mg/dL and Na/K/Cl = 122/3.9/89 mEq/mL. Paracentesis revealed clear yellow-colored ascitic fluid, which on analysis showed 230/mm3 WBC, 400/mm3 red blood cells, 200 mg/dL glucose, and 210 mg/dL protein. The serum α-fetoprotein concentration was 4.2 ng/mL.
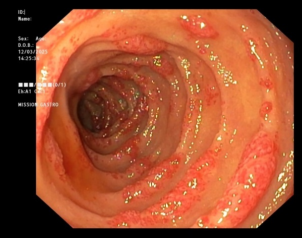
Bleeding from the esophageal varices was suspected and urgent endoscopic examination was performed. However, the endoscopy showed no esophageal varices. It showed GAVE, Mild portal hypertensive gastropathy (PHG) and vascular ectasia was found on the duodenal bulb and in duodenum till deep in third part (Figure 1). Endoscopic biopsy was performed from the vascular ecstatic mucosa and histological examination revealed patchy mild chronic active duodenitis with patchy mild villous blunting with mild Brunner's gland hyperplasia and lamina propria shows mild fibrosis and dilated vascular channels filled with blood and few shows thrombus suggestive of Duodenal vascular ectasia (Figure 2). We went ahead initially with APC for the GAVE and did not perform APC of duodenum in view of high risk of perforation in duodenum with APC. Patient still had complaints of black stool and drop in HB even after 2 more sessions of APC for GAVE in follow up with repeated iron and blood transfusion requirements. In view of persistent drop in HB, APC for duodenal vascular ectasia was performed twice at the interval of 1 month (Figure 3). After endoscopic treatment, his hemoglobin concentration stabilized and his anemic symptoms improved, and the patient was off iron and blood transfusion in follow-up visit. To minimize the risk of bowel perforation, we applied APC for 4–6 seconds at a power setting of 50 W, successfully controlling the bleeding without any complications.
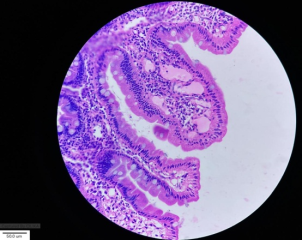
Figure 2. Histological image showing patchy mild chronic active duodenitis with patchy mild villous blunting with mild Brunner's gland hyperplasia and lamina propria shows mild fibrosis and dilated vascular channels filled with blood and few shows thrombus within suggestive of Duodenal vascular ectasia (DVE).
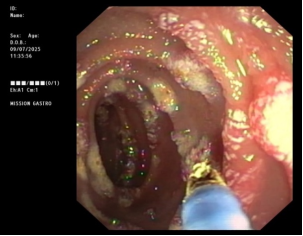
Figure 3. Endoscopic image showing Argon plasma coagulation (APC) of the duodenal vascular ectasia (DVE).
3. Discussion
Upper gastrointestinal bleeding is a common and serious complication in the clinical course of liver cirrhosis, contributing significantly to morbidity and mortality.
[8]
Franco D, Durandy Y, Deporte A, Bismuth H. Upper gastrointestinal haemorrhage in hepatic cirrhosis: causes and relation to hepatic failure and stress. Lancet. 1977; 1: 218-220.
[8]
Gastroesophageal varices are the most frequent source of bleeding in cirrhotic patients, accounting for 59.1% of cases in a recent study.
[9]
Lecleire S, Di Fiore F, Merle V, Hervé S, Duhamel C, Rudelli A, et al. Acute upper gastrointestinal bleeding in patients with liver cirrhosis and in noncirrhotic patients: epidemiology and predictive factors of mortality. J Clin Gastroenterol. 2005; 39: 321-327.
Similar rates have been reported in other studies, with esophageal variceal bleeding occurring in 49% to 72% of patients.
[10]
Gatta A, Merkel C, Amodio P, Bellon S, Bellumat A, Bolognesi M, et al. Development and validation of a prognostic index predicting death after upper gastrointestinal bleeding in cirrhosis. Am J Gastroenterol. 1994; 89: 1528-1536.
Peptic ulcer bleeding ranks as the second most common cause, responsible for 15.7% of bleeding episodes.
[9]
Lecleire S, Di Fiore F, Merle V, Hervé S, Duhamel C, Rudelli A, et al. Acute upper gastrointestinal bleeding in patients with liver cirrhosis and in noncirrhotic patients: epidemiology and predictive factors of mortality. J Clin Gastroenterol. 2005; 39: 321-327.
Upper gastrointestinal vascular ectasia is increasingly recognized as a significant source of gastrointestinal bleeding, presenting either as overt bleeding or as a cause of obscure gastrointestinal blood loss.
[3]
Clouse RE, Costigan DJ, Mills BA, Zuckerman GR. Angiodysplasia as a cause of upper gastrointestinal bleeding. Arch Intern Med. 1985; 145: 458-461.
Gastric antral vascular ectasia (GAVE) is a distinct form of vascular abnormality predominantly affecting the gastric antrum, characterized endoscopically by linear, friable red streaks radiating from the pylorus. In contrast, angiodysplastic lesions typically appear as discrete, flat or slightly elevated, bright-red spots measuring 2–10 mm, often with fern-like borders and a pale surrounding halo.
[14]
Pavey DA, Craig PI. Endoscopic therapy for upper-GI vascular ectasia. Gastrointest Endosc. 2004; 59: 233-238.
Clinically, these lesions may manifest as chronic low-grade bleeding, frequently resulting in iron-deficiency anemia, or as acute bleeding with hematemesis or melena. Patients often experience recurrent bleeding episodes, necessitating multiple blood transfusions and potentially leading to transfusion dependency.
[14]
Pavey DA, Craig PI. Endoscopic therapy for upper-GI vascular ectasia. Gastrointest Endosc. 2004; 59: 233-238.
Arendse MP, Jaskiewicz K, Funnell I. Massive gastrointestinal haemorrhage due to vascular ectasia of the duodenum. S Afr J Surg. 1992; 30: 111-113.
[7]
Calès P, Voigt JJ, Payen JL, Bloom E, Berg P, Vinel JP, et al. Diffuse vascular ectasia of the antrum, duodenum, and jejunum in a patient with nodular regenerative hyperplasia. Gut. 1993; 34: 558-561.
Arendse MP, Jaskiewicz K, Funnell I. Massive gastrointestinal haemorrhage due to vascular ectasia of the duodenum. S Afr J Surg. 1992; 30: 111-113.
[6]
described a fatal case of duodenal vascular ectasia in a cirrhotic patient, diagnosed postmortem. To our knowledge, the present case is the first to document successful hemostasis of duodenal vascular ectasia in a cirrhotic patient using argon plasma coagulation (APC).
Prior to the widespread adoption of therapeutic endoscopy, vascular ectasia was managed primarily through surgical resection.
[15]
Moore JD, Thompson NW, Appelman HD, Foley D. Arteriovenous malformations of the gastrointestinal tract. Arch Surg. 1976; 111: 381-389.
This technique offers several advantages, such as the ease of treating broad mucosal areas, controlled depth of coagulation, and faster healing of treated regions, allowing for a more efficient achievement of therapeutic goals.
[17]
Johanns W, Luis W, Janssen J, Kahl S, Greiner L. Argon plasma coagulation (APC) in gastroenterology: experimental and clinical experiences. Eur J Gastroenterol Hepatol. 1997; 9: 581-587.
In conclusion, duodenal vascular ectasia should be considered a potential source of upper gastrointestinal bleeding in patients with cirrhosis. Argon plasma coagulation appears to be a safe and effective therapeutic modality for achieving hemostasis in such cases.
Chirag Shah: Investigation, Writing – original draft
Vidish Sheth: Formal Analysis, Investigation
Vishal Modi: Investigation
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Tai DI, Chou FF, Lee TY, Lin CC. Vascular ectasia of the duodenum detected by duodenoscopy. Am J Gastroenterol. 1987; 82: 1071-1073.
[2]
Weaver GA, Alpern HD, Davis JS, Ramsey WH, Reichelderfer M. Gastrointestinal angiodysplasia associated with aortic valve disease: part of a spectrum of angiodysplasia of the gut. Gastroenterology. 1979; 77: 1-11.
[3]
Clouse RE, Costigan DJ, Mills BA, Zuckerman GR. Angiodysplasia as a cause of upper gastrointestinal bleeding. Arch Intern Med. 1985; 145: 458-461.
Cappell MS, Lebwohl O. Cessation of recurrent bleeding from gastrointestinal angiodysplasias after aortic valve replacement. Ann Intern Med. 1986; 105: 54-57.
Arendse MP, Jaskiewicz K, Funnell I. Massive gastrointestinal haemorrhage due to vascular ectasia of the duodenum. S Afr J Surg. 1992; 30: 111-113.
[7]
Calès P, Voigt JJ, Payen JL, Bloom E, Berg P, Vinel JP, et al. Diffuse vascular ectasia of the antrum, duodenum, and jejunum in a patient with nodular regenerative hyperplasia. Gut. 1993; 34: 558-561.
Franco D, Durandy Y, Deporte A, Bismuth H. Upper gastrointestinal haemorrhage in hepatic cirrhosis: causes and relation to hepatic failure and stress. Lancet. 1977; 1: 218-220.
[9]
Lecleire S, Di Fiore F, Merle V, Hervé S, Duhamel C, Rudelli A, et al. Acute upper gastrointestinal bleeding in patients with liver cirrhosis and in noncirrhotic patients: epidemiology and predictive factors of mortality. J Clin Gastroenterol. 2005; 39: 321-327.
Gatta A, Merkel C, Amodio P, Bellon S, Bellumat A, Bolognesi M, et al. Development and validation of a prognostic index predicting death after upper gastrointestinal bleeding in cirrhosis. Am J Gastroenterol. 1994; 89: 1528-1536.
Gupta, D., Patel, S., Kapadiya, M., Bhatt, P., Shah, C., et al. (2026). Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding. International Journal of Gastroenterology, 10(1), 39-42. https://doi.org/10.11648/j.ijg.20261001.17
Gupta D, Patel S, Kapadiya M, Bhatt P, Shah C, et al. Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding. Int J Gastroenterol. 2026;10(1):39-42. doi: 10.11648/j.ijg.20261001.17
@article{10.11648/j.ijg.20261001.17,
author = {Dhaval Gupta and Sachin Patel and Maulik Kapadiya and Pratin Bhatt and Chirag Shah and Vidish Sheth and Vishal Modi},
title = {Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {39-42},
doi = {10.11648/j.ijg.20261001.17},
url = {https://doi.org/10.11648/j.ijg.20261001.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.17},
abstract = {Duodenal vascular ectasia (DVE) is a rare but important cause of upper gastrointestinal bleeding, particularly in patients with chronic liver disease. Gastric antral vascular ectasia (GAVE) is a more commonly recognized vascular lesion associated with cirrhosis; however, vascular ectasia involving the duodenum is infrequently reported and may pose diagnostic and therapeutic challenges. We report a case of a cirrhotic patient presenting with recurrent upper gastrointestinal bleeding manifested as melena and progressive anemia. Initial evaluation suggested variceal bleeding; however, endoscopic examination revealed the presence of GAVE along with vascular ectasia involving the duodenal bulb and extending into the third part of the duodenum. Histopathological examination of duodenal biopsies demonstrated dilated vascular channels within the lamina propria, consistent with duodenal vascular ectasia. Endoscopic management was initially directed toward GAVE using argon plasma coagulation (APC). Due to persistent anemia and recurrent bleeding, APC therapy was subsequently applied to the duodenal vascular lesions with careful technique to minimize the risk of perforation. Hemostasis was successfully achieved without complications, and the patient showed sustained clinical improvement with stabilization of hemoglobin levels and no further transfusion requirement during follow-up. This case highlights duodenal vascular ectasia as a potential source of gastrointestinal bleeding in cirrhotic patients and demonstrates that argon plasma coagulation can be a safe and effective therapeutic modality when applied cautiously.},
year = {2026}
}
TY - JOUR
T1 - Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding
AU - Dhaval Gupta
AU - Sachin Patel
AU - Maulik Kapadiya
AU - Pratin Bhatt
AU - Chirag Shah
AU - Vidish Sheth
AU - Vishal Modi
Y1 - 2026/05/13
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.17
DO - 10.11648/j.ijg.20261001.17
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 39
EP - 42
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.17
AB - Duodenal vascular ectasia (DVE) is a rare but important cause of upper gastrointestinal bleeding, particularly in patients with chronic liver disease. Gastric antral vascular ectasia (GAVE) is a more commonly recognized vascular lesion associated with cirrhosis; however, vascular ectasia involving the duodenum is infrequently reported and may pose diagnostic and therapeutic challenges. We report a case of a cirrhotic patient presenting with recurrent upper gastrointestinal bleeding manifested as melena and progressive anemia. Initial evaluation suggested variceal bleeding; however, endoscopic examination revealed the presence of GAVE along with vascular ectasia involving the duodenal bulb and extending into the third part of the duodenum. Histopathological examination of duodenal biopsies demonstrated dilated vascular channels within the lamina propria, consistent with duodenal vascular ectasia. Endoscopic management was initially directed toward GAVE using argon plasma coagulation (APC). Due to persistent anemia and recurrent bleeding, APC therapy was subsequently applied to the duodenal vascular lesions with careful technique to minimize the risk of perforation. Hemostasis was successfully achieved without complications, and the patient showed sustained clinical improvement with stabilization of hemoglobin levels and no further transfusion requirement during follow-up. This case highlights duodenal vascular ectasia as a potential source of gastrointestinal bleeding in cirrhotic patients and demonstrates that argon plasma coagulation can be a safe and effective therapeutic modality when applied cautiously.
VL - 10
IS - 1
ER -
Department of Gastroenterology, Gujarat Cancer Society Medical College (GCSMC), Hospital & Research Centre, Ahmedabad, India; Department of Gastroenterology, Mission Gastro Hospital, Ahmedabad, India
Gupta, D., Patel, S., Kapadiya, M., Bhatt, P., Shah, C., et al. (2026). Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding. International Journal of Gastroenterology, 10(1), 39-42. https://doi.org/10.11648/j.ijg.20261001.17
Gupta D, Patel S, Kapadiya M, Bhatt P, Shah C, et al. Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding. Int J Gastroenterol. 2026;10(1):39-42. doi: 10.11648/j.ijg.20261001.17
@article{10.11648/j.ijg.20261001.17,
author = {Dhaval Gupta and Sachin Patel and Maulik Kapadiya and Pratin Bhatt and Chirag Shah and Vidish Sheth and Vishal Modi},
title = {Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {39-42},
doi = {10.11648/j.ijg.20261001.17},
url = {https://doi.org/10.11648/j.ijg.20261001.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.17},
abstract = {Duodenal vascular ectasia (DVE) is a rare but important cause of upper gastrointestinal bleeding, particularly in patients with chronic liver disease. Gastric antral vascular ectasia (GAVE) is a more commonly recognized vascular lesion associated with cirrhosis; however, vascular ectasia involving the duodenum is infrequently reported and may pose diagnostic and therapeutic challenges. We report a case of a cirrhotic patient presenting with recurrent upper gastrointestinal bleeding manifested as melena and progressive anemia. Initial evaluation suggested variceal bleeding; however, endoscopic examination revealed the presence of GAVE along with vascular ectasia involving the duodenal bulb and extending into the third part of the duodenum. Histopathological examination of duodenal biopsies demonstrated dilated vascular channels within the lamina propria, consistent with duodenal vascular ectasia. Endoscopic management was initially directed toward GAVE using argon plasma coagulation (APC). Due to persistent anemia and recurrent bleeding, APC therapy was subsequently applied to the duodenal vascular lesions with careful technique to minimize the risk of perforation. Hemostasis was successfully achieved without complications, and the patient showed sustained clinical improvement with stabilization of hemoglobin levels and no further transfusion requirement during follow-up. This case highlights duodenal vascular ectasia as a potential source of gastrointestinal bleeding in cirrhotic patients and demonstrates that argon plasma coagulation can be a safe and effective therapeutic modality when applied cautiously.},
year = {2026}
}
TY - JOUR
T1 - Duodenal Vascular Ectasia: Rare Cause of Gastrointestinal Bleeding
AU - Dhaval Gupta
AU - Sachin Patel
AU - Maulik Kapadiya
AU - Pratin Bhatt
AU - Chirag Shah
AU - Vidish Sheth
AU - Vishal Modi
Y1 - 2026/05/13
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.17
DO - 10.11648/j.ijg.20261001.17
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 39
EP - 42
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.17
AB - Duodenal vascular ectasia (DVE) is a rare but important cause of upper gastrointestinal bleeding, particularly in patients with chronic liver disease. Gastric antral vascular ectasia (GAVE) is a more commonly recognized vascular lesion associated with cirrhosis; however, vascular ectasia involving the duodenum is infrequently reported and may pose diagnostic and therapeutic challenges. We report a case of a cirrhotic patient presenting with recurrent upper gastrointestinal bleeding manifested as melena and progressive anemia. Initial evaluation suggested variceal bleeding; however, endoscopic examination revealed the presence of GAVE along with vascular ectasia involving the duodenal bulb and extending into the third part of the duodenum. Histopathological examination of duodenal biopsies demonstrated dilated vascular channels within the lamina propria, consistent with duodenal vascular ectasia. Endoscopic management was initially directed toward GAVE using argon plasma coagulation (APC). Due to persistent anemia and recurrent bleeding, APC therapy was subsequently applied to the duodenal vascular lesions with careful technique to minimize the risk of perforation. Hemostasis was successfully achieved without complications, and the patient showed sustained clinical improvement with stabilization of hemoglobin levels and no further transfusion requirement during follow-up. This case highlights duodenal vascular ectasia as a potential source of gastrointestinal bleeding in cirrhotic patients and demonstrates that argon plasma coagulation can be a safe and effective therapeutic modality when applied cautiously.
VL - 10
IS - 1
ER -