Abstract
Introduction Cervical cancer screening is used to find changes in the cells of the cervix that could lead to cancer. Despite, screening is one of the secondary preventive strategies, the case is still growing. Therefore, the study aimed to assess the uptake of cervical cancer screening services and associated factors among Women living with human immunodeficiency virus at public health Facility in Waliso Town, Ethiopia, 2024. Methods and materials: A facility- based cross=sectional study done among 396 women was conducted from April 1-June 25, 2024 Systematic random sampling was used to select women for face-to-face interviews. The bivariable and multivariable logistic regression analyses were done. The data were collected through the face-to-face interview by a structured questionnaire. For analysis, the data were entered into Epi data version 4.6 and exported to Statistical Package for the Social Sciences version 26 software. Bivariate analysis for candidate variables selection (p< 0.25) was used. Multivariable analysis for p-value < 0.05 and 95% confidence level were considered as significantly associated. Results: The proportion of cervical cancer screening uptake among HIV-positive women was 12.1%, 95% confidence interval of 9%- 15%. Variables like an age between 40-49 years [AOR = 3.65; 95%CI=1.20, 11.07], having college above educational level [AOR = 3.04; 95% CI: 1.05, 8.80], Urban residents [AOR = 3.49; 95%CI=1.64, 7.44], and having good knowledge [AOR 3.9; 95%CI: 1.70, 8.83] were significantly associated with uptake of cervical cancer screening service. Service interruption, poor awareness, and rumor were barrier of uptake of cervical cancer screening among HIV-positive women. Conclusion and recommendation: The finding of this study showed that only one in ten HIV-positive women was screened. We recommend that increasing women’s knowledge about cervical cancer screening, particularly targeting the younger ones, is crucial to enhance the uptake of screening and promote health education among rural women so that recommended cervical cancer screening can be utilized more effectively.
Keywords
Uptake, Cervical Cancer, HIV-Positive Women, Waliso Town, Ethiopia
1. Introduction
Cervical cancer is a heterogeneous group of diseases characterized by autonomous and uncontrolled growth of cells originating from the uterine cervix, an anatomical structure connecting the lower uterus to the vagina
| [1] | WHO, WHO framework for strengthening and scaling- up of services for the management of invasive cervical cancer. 2020. |
[1]
. It begins with aberrant cell alterations known as pre-cancerous (dysplasia), which can either regress or progress into cancer over time and differs from other cancers because it grows slowly
| [2] | R. C. Christina, What Every Woman Should Know about Cervical Cancer. 2018. |
[2]
.
The problem is worse for women living with HIV who are at a six-fold greater risk of developing cervix cancer than non-HIV-positive women. This elevated risk manifests itself during a person's lifetime, beginning with a greater risk of acquiring the human papillomavirus, especially HPV 16 and 18 types which handle 70% of cervical carcinomas
| [3] | WHO, “New WHO recommendations on screening and treatment to prevent cervical cancer among women living with HIV Policy brief,” vol. 2020, pp. 1-6, 2020, https://doi.org/10.3322/caac.21660.3 |
| [4] | ACOG, “Cervical Cancer Screening,” no. May, p. 20024, 2021. |
[3, 4]
.
Cervical cancer screening is a secondary prevention type used to find changes in the cells of the cervix that could lead to cancer
| [4] | ACOG, “Cervical Cancer Screening,” no. May, p. 20024, 2021. |
[4]
. Its efforts aim to reduce cervical cancer incidence and mortality by identifying and treating precancerous lesions in women
| [1] | WHO, WHO framework for strengthening and scaling- up of services for the management of invasive cervical cancer. 2020. |
[1]
. The most frequent method for cervical cancer screening is cytology, and there are alternative methods, such as HPV DNA tests and visual inspection with acetic acid (VIA). In resource-limited countries, VIA is the preferred approach
| [5] | World Health Organization, Global strategy to accelerate the elimination of cervical cancer as a public health problem and its associated goals and targets for the period 2020 - 2030, vol. 2, no. 1. 2021. |
[5]
.
About 7,445 new cervical cancer cases are reported annually in Ethiopia, with 5,338 cervical-cancer deaths
| [3] | WHO, “New WHO recommendations on screening and treatment to prevent cervical cancer among women living with HIV Policy brief,” vol. 2020, pp. 1-6, 2020, https://doi.org/10.3322/caac.21660.3 |
| [6] | WHO, Global strategy to accelerate the elimination of cervical cancer as a public health problem. 2020. |
| [7] | Fmoh, “National Cervical Cancer Prevention Training Package Participant Manual,” 2015. |
| [8] | ETHIOPIA ICO/IARC on HPV report, “Human Papillomavirus and Related Diseases Report,” no. October, 2021. |
[3, 6-8]
. Despite gains in life expectancy associated with access to HIV care and treatment in the countries the hardest hit by the epidemic, cervical-cancer in HIV-positive women has not gotten the attention or resources it deserves for prevention and treatment, and screening coverage is often low
| [9] | UNAIDS, “Data 2017,” Program. HIV/AIDS, pp. 1-248, 2017. |
[9]
. To reach vulnerable women at high risk of cervical-cancer and HIV infection, integrated human papillomavirus (HPV) vaccination, screening, and treatment services for both diseases must be prioritized to optimize efficiency and maximum effect
| [6] | WHO, Global strategy to accelerate the elimination of cervical cancer as a public health problem. 2020. |
[6]
.
In 2020, an estimated 604 000 women were diagnosed with cervical cancer and about 342 000 women died from the disease. Of the 604 000 new cases of cervical cancer in 2020, 5% were attributable to HIV infection
| [5] | World Health Organization, Global strategy to accelerate the elimination of cervical cancer as a public health problem and its associated goals and targets for the period 2020 - 2030, vol. 2, no. 1. 2021. |
[5]
. Its burdens vary greatly between countries, approximately 85% of women living with HIV occur in Africa Region, 7% in South-East Asia and 4% in the Americas
| [9] | UNAIDS, “Data 2017,” Program. HIV/AIDS, pp. 1-248, 2017. |
| [10] | D. Stelzle et al., “Estimates of the global burden of cervical cancer associated with HIV,” Lancet Glob. Heal., vol. 9, no. 2, pp. e161-e169, 2021, https://doi.org/10.1016/S2214-109X(20)30459-9 |
| [11] | S. Menon et al., “Associations between highly active antiretroviral therapy and the presence of HPV, premalignant and malignant cervical lesions in sub-Saharan Africa, a systematic review: Current evidence and directions for future research,” BMJ Open, vol. 7, no. 8, 2017, https://doi.org/10.1136/bmjopen-2016-015123 |
[9-11]
. In Ethiopia, it is the second most frequent and primary cause of cancer-related death in 2015 with an estimated 4648 new cases and 3,235 dying from it
| [7] | Fmoh, “National Cervical Cancer Prevention Training Package Participant Manual,” 2015. |
[7]
.
Regarding medical, nonmedical, and human terms, the worldwide cost of cancer as the primary cause of long-term mortality reflects a colossal waste of resources. E.g., inside the United States, the estimated cost management has risen from $124 billion in 2010 to $157 billion in 2020
| [12] | L. G. Bona et al., “Economic Burden of Cancer on Cancer Patients Treated at Hawassa University Comprehensive Specialized Hospital,” Cancer Control, vol. 28, pp. 1-8, 2021, https://doi.org/10.1177/10732748211009252 |
[12]
.
Cervical cancer and HIV are intrinsically interlinked. Women living with HIV have higher rates of HPV infection and precancerous lesions, with a six-times higher risk of invasive cervical cancer compared to women without HIV
| [3] | WHO, “New WHO recommendations on screening and treatment to prevent cervical cancer among women living with HIV Policy brief,” vol. 2020, pp. 1-6, 2020, https://doi.org/10.3322/caac.21660.3 |
[3]
. The higher risk is manifested throughout the life cycle, starting with an increased risk of acquiring HPV infection, more rapid progression to cancer, and developing cervical cancer at a younger age
| [13] | R. S. Chambuso, E. Kaambo, and S. Stephan, “Observed Age Difference and Clinical Characteristics of Invasive Cervical Cancer Patients in Tanzania; A Comparison between HIV-Positive and HIV-Negative Women,” J. Neoplasm, vol. 02, no. 03, 2017, https://doi.org/10.21767/2576-3903.100025 |
[13]
.
As women living with HIV have a higher risk of cervical cancer, they require regular screening to ensure timely detection and successful treatment of precancerous lesions to prevent them from developing invasive cervical cancer
| [9] | UNAIDS, “Data 2017,” Program. HIV/AIDS, pp. 1-248, 2017. |
[9]
. Currently, coverage for cervical cancer screening is inadequate in LMICs
. In Ethiopia, the planned goal was to achieve 80 percent coverage for cervical cancer screening in 2016-2020
| [14] | N. Cancer and C. Plan, “FEDERAL MINISTRY OF HEALTH,” no. October 2015, 2020. |
[14]
. Despite this, less than 10% of women had been screened in the last 5 years in 2021
| [15] | WHO, “Cervical cancer profile,” no. 2020, p. 2021, 2021. |
[15]
.
Even previously many researchers tried to rule out factors like socio-demographic characteristics
| [16] | Woldetsadik et al., “Socio-demographic characteristics and associated factors influencing cervical cancer screening among women attending in St. Paul’ s Teaching and Referral Hospital,” pp. 1-9, 2020. |
[16]
, area of residence
| [17] | L. R. B. Locklar and D. P. Do, “Rural-urban differences in HPV testing for cervical cancer screening.,” J. Rural Heal. Off. J. Am. Rural Heal. Assoc. Natl. Rural Heal. Care Assoc., Sep. 2021, https://doi.org/10.1111/jrh.12615 |
[17]
, the flow of information
| [18] | A. M. Mugassa and G. Frumence, “Factors influencing the uptake of cervical cancer screening services in Tanzania: A health system perspective from national and district levels,” Nurs. Open, vol. 7, no. 1, pp. 345-354, 2020, https://doi.org/10.1002/nop2.395 |
[18]
, and knowledge about the disease
| [19] | D. Mrema and J. Ngocho, “Uptake of Cervical Cancer Screening and the Associated Factors Among Women Living With HIV in Northern Tanzania,” 2021. |
[19]
were contributed to low rates of screening uptake in the populations. Despite these efforts has done still uptake of cervical cancer was low. To date, insufficient attention has been given to the links between cervical cancer and HIV-positive women
| [9] | UNAIDS, “Data 2017,” Program. HIV/AIDS, pp. 1-248, 2017. |
[9]
.
This prompted an investigation into why so few women follow recommended practices for cervical cancer screening. Consequently, the aim of this study was to assess cervical cancer screening service uptake and associated factors among HIV-positive women of public health Facility in Waliso Town, Ethiopia.
2. Methods and Materials
2.1. Study Area and Period
The study was conducted in Waliso Town which is the administrative center of the South West Shewa Zone, Oromia Regional State. It is located to 114 km southwest of Addis Ababa were women. 146,758 lived in urban and 1,284,547 were rural. There are five public hospitals, but only four of them have ART-clinic. Six months total population ART women report was 1816. There is one government hospital and two Health Centers. The study was conducted from April 1-June 25, 2024.
Study Design: A facility-based, cross-sectional study design was conducted.
Sources of population: All HIV-positive women attending ART-clinic at public health Facility in Waliso Town, Ethiopia. Study population is all sampled HIV-positive women presented during data collection and who full fill inclusion criteria at public hospitals with ART-clinic in public health Facility in Waliso Town.
2.2. Eligible Criteria
Inclusion criteria: all HIV-positive women who had a current follow-up at the ART clinic presented during data collection. Women who were unable to communicate due to any illness were excluded from the study.
2.3. Sample Size Determination
A single population proportion was used to estimate the sample size and the following assumptions were made.
Where n = sample size
Z = standard normal distribution curve value for the 95% confidence interval (1.96)
d = the margin of error or accepted error (0.03)
P is the estimated uptake of cancer cervix screening among HIV-positive women was 8.7% from a study that was done at Ambo town, Ethiopia (20).
Substitution of the figures above into the formula gives a sample size of
By adding a 10% non-response rate the final sample size was 339+34=373.
For the second objective, the sample size is calculated by using Epi-info version 7.25 and different variables with a strong correlation with the dependent variable from various types of literature were used to establish the sample size for specific objectives by using double population proportion, 80% power, 95% CI using identified associated factors with uptake of cervical cancer screening such as education Status
| [20] | Assefa et al., “Cervical cancer screening service utilization and associated factors among HIV positive women attending adult ART clinic in public health facilities, Hawassa town, Ethiopia : a cross-sectional study,” vol. 5, pp. 1-11, 2019. |
[20]
, Information from health profession
| [21] | S. Getachew, E. Getachew, M. Gizaw, W. Ayele, A. Addissie, and E. J. Kantelhardt, “Cervical cancer screening knowledge and barriers among women in Addis Ababa, Ethiopia,” PLoS One, vol. 14, no. 5, pp. 1-13, 2019, https://doi.org/10.1371/journal.pone.0216522 |
[21]
and area of residence
| [22] | Nega et al., “Low uptake of cervical cancer screening among HIV positive women in Gondar University referral hospital, Northwest Ethiopia : cross-sectional study design,” pp. 1-7, 2018. |
[22]
.
Since the sample size for specific objective one (373) is smaller than the sample size for specific objective two, Hence the specific 2 objective sample size (396) was used.
2.4. Sampling Technique and Procedure
A systematic random sampling method was used to select 396 women. First, all four public hospitals with ATR-clinic found in the Waliso Town: To select study participants from each hospital the total sample size was allocated proportionally to size as the following. Finally, for each facility, systematic random sampling was conducted at every constant interval (Kth=N/n). K=1816÷396=4.6 ~4. We selected the first participant via lottery.
2.5. Study Variables
Dependent variable: Uptake of cervical cancer screening service.
Independent variables: Age, marital status, residence, occupation, educational status, knowledge status.
2.6. Operational Definitions
Cervical cancer screening uptake: Participants who had screened at least once in in the past five years were considered to have used cervical cancer screening". It was assessed by asking “Have you ever had cervical cancer screening in the past five years?”, if the respondents answered, “yes” it is considered as use cervical screening and labeled as “1” for analysis, while if the respondents answered “no”, it is taken as didn’t use cervical screening service and labeled as “0”
| [20] | Assefa et al., “Cervical cancer screening service utilization and associated factors among HIV positive women attending adult ART clinic in public health facilities, Hawassa town, Ethiopia : a cross-sectional study,” vol. 5, pp. 1-11, 2019. |
[20]
.
Knowledge: Seven items composite score of knowledge to measure the knowledge level of respondents regarding vulnerable groups, risk factors, signs, symptoms, and prevention methods of cervical cancer. We estimated the cumulative mean score of knowledge of participants about cervical cancer using a mean score. Based on this, those who had a score less than the mean were considered to have poor knowledge and those who had a score greater than or equal to the mean value were considered to have good knowledge
.
2.7. Method of Data Collection (Instruments and Procedure)
The principal investigator adapted the structured questionnaire in the English-language version after reviewing different literature. Then, it is translated into Afan Oromo by a language expert.
A pretested structured questionnaire on 5% of the total sample size was used to collect data by four BSc nurses with face-to-face interviews and one supervisor who do not work in the service ward. The data collectors were oriented for one day by the principal investigator about the purpose of the study, how to interview and fill out the questionnaire properly. Orientation was given by the local language on how to ask and fill the questions, selection criteria of participants, keeping privacy and how to approach the respondents. We collected data during hospital visits.
The data collector was informed of the selected participants, as she was selected to take part in the study. From the selected participant, verbal consent was got, and the data were collected. One data collector was assigned to one hospital and supervised by the supervisor.
2.8. Data Quality Control
Data were controlled through the orienting of data collectors and supervisors on objectives and questionnaires. Data collectors were supervised by the supervisor and the principal investigator received a report daily. Before the actual data collection pretest was performed by taking 5% of the study of the population at a Holeta Health Center. After analysis of the pre-test result, minor modification like typing error was corrected.
Also, Cronbach's alpha was computed by SPSS version 26 to assess the internal consistency and reliability of the questionnaires. A construct is reliable if the alpha value is greater than 0.7
. The result revealed that the knowledge level was assessed consisting of seven items and the value for Cronbach’s Alpha for the knowledge level was α =0.91.
During data collection, all data were checked for completeness and consistency. After being collected, the data was cleaned manually, coded, and entered into Epi data version 4.6. Double data entry was done by one data clerk and the consistency of the entered data were cross-checked by comparing the two separately entered data then exported to SPSS version 26 software for further analysis. To ensure the consistency of the questionnaire, the English version was translated into Afan Oromo.
2.9. Data Processing and Analysis
Collected data were cleaned and coded for completeness and accuracy, and then entered Epi data version 4.6 and exported to SPSS version 26 software was used for further analysis. Descriptive statistics were used to calculate the result in proportion, frequencies, cross-tabulation, and measures of central tendency.
A binary logistic regression was used to show factors associated with cervical cancer screening service uptake. Bivariate analysis for candidate variables selection (p< 0.25) and then, multivariable analysis for showing the independent associated factors was employed using a p-value of < 0.05 and a 95% confidence level. The enter method was used for controlling the confounder to have a final model and the Adjusted Odds Ratio was employed to calculate the strength of association. Hosmer and Lermeshows tests were employed to test model goodness of fit and using a p-value of > 0.05.
Consequently, these results revealed Hosmer and Lermeshows test statistic indicates that the model adequately good fit since chi-square=6.07, df=8. P-value=.69. Hence there is no difference between the observed and predicted models.
3. Results
A total of 391 women living with HIV took part in this study and completed the questionnaire with a 98.7% response rate. The 5 questionnaires were incomplete and excluded from the analysis.
3.1. Sociodemographic Characteristics
The mean age of the study participants was 41 years, SD±7 and more than one-third of women n=131 (34%) fell in the 30-39 years age rang. More than half of the study participants 215 (55%) were married. One hundred thirty-four (34%) of women had attended primary education level (see
Table 1).
Table 1. Sociodemographic characteristics of the respondents among HIV-positive women in public health Facility in Waliso Town, Oromia, Ethiopia, 2022.
Variables | Categories | Frequencies (n=391) | Percent |
Age in years | ≤29 | 68 | 17 |
30-39 | 131 | 34 |
40-49 | 94 | 24 |
≥50 | 98 | 25 |
Marital status | Married | 215 | 55 |
Divorce | 70 | 18 |
Widowed | 66 | 17 |
Single | 40 | 10 |
The educational level status of women | No formal education | 107 | 27 |
Primary | 134 | 34 |
Secondary | 105 | 27 |
collage and above | 45 | 12 |
Women’s occupation | Housewife | 122 | 31 |
Merchant | 58 | 15 |
government employee | 42 | 11 |
private employee | 89 | 23 |
Student | 29 | 7 |
Farmer | 52 | 13 |
Place of residence | Urban | 182 | 46.5 |
Rural | 209 | 53.5 |
3.2. Knowledge About Cervical Cancer
Seven questions were used to assess the knowledge status of HIV- positive women in the North Shewa zone of public hospitals. Among 391 of HIV- positive women 146 (37%) were heard about cervical cancer screening services. Three hundred two of HIV- positive women (82%) were doesn`t know HIV-AIDS was risk factors for cervical cancer (
Table 2).
Table 2. Knowledge items about cervical cancer screening among participants, 2024.
Variables | Response | Frequency | Percentage |
Have you ever heard about cervical cancer? | Yes | 146 | 37 |
No | 245 | 63 |
Do you know HIV- AIDS is the risk factors for cervical cancer? | Yes | 71 | 18 |
No | 320 | 82 |
Do you know the way of transmission? | Yes | 51 | 13 |
No | 340 | 87 |
Do you know the signs and symptoms? | Yes | 52 | 13 |
No | 339 | 87 |
Do you know the way of prevention? | Yes | 51 | 13 |
No | 339 | 87 |
Is it important for every woman who has HIV to screen for cancer of the cervix? | Yes | 232 | 59 |
No | 159 | 41 |
Do you know the availability of the service? | Yes | 104 | 26.5 |
No | 287 | 73.5 |
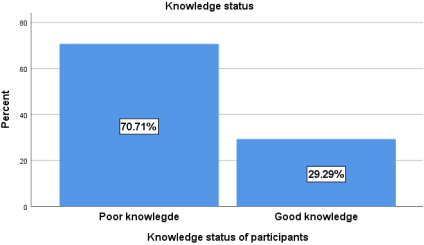
Figure 1. Knowledge about cervical cancer among HIV-positive in Public health Facility in Waliso Town, Oromia, Ethiopia, 2024.
The finding of this study revealed that less than one-third (29.3%) of the respondents had good knowledge with [95% CI 25%, 34%] (
Figure 1).
3.3. Reason for Cervical Cancer Screening Services
The main reasons for screened were seeing the need 34 (71%) and obedience to the health profession was 32 (67%). Among 47 women who screened cervical cancer 4 (8%) were knew the screening service was free (see
Table 3).
Table 3. Reason for screening among HIV-positive women in public health Facility in Waliso Town, Oromia, Ethiopia, 2024.
Response n=47 | Frequency | Percentage |
Saw the need for screening | 34 | 71 |
Obedience to health professional’s instructions | 32 | 67 |
I am at risk of getting cervical cancer | 17 | 35 |
The service was available at the clinic | 6 | 13 |
The screening service was free | 4 | 8 |
I know someone who screened | 4 | 8 |
My husband encouraged me | 4 | 8 |
3.4. Barrier of Cervical Cancer Screening
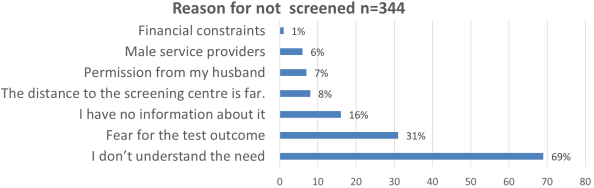
Figure 2. Barriers of cervical cancer screening services among HIV-positive women in Public health Facility in Waliso Town, Ethiopia, 2022.
The current study was showed that in contrast to motivators, there are barriers to screening services. The most common barriers mentioned were didn’t understand the needs 68.43% and fear of test outcome while financial constraints 1% were the least stated (see
Figure 2).
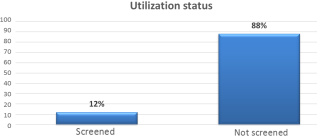
3.5. Prevalence of Uptake of Cervical Cancer Screening
In this study, we have found that 12% [95% CI 9%, 15%] of HIV-positive women were utilized cervical cancer screening at least once in their lifetime (see
Figure 3).
Figure 3. Uptake of cervical cancer screening services among HIV-positive women in public health Facility in Waliso Town, Oromia, Ethiopia, 2024.
3.6. Associated factors for Uptake of Cervical Cancer Screening
In bivariate logistic regression analysis, the age of women, marital status, maternal occupation, area of residence, educational level of women, information about screening services and knowledge level of women were candidate variables for multivariate analysis at (p-value <0.25). After controlling a possible confounding variable by multivariable logistic regression analysis, age, educational level, residence, and knowledge status had a significant association with the uptake of cervical cancer screening. Adjusted in a
Table 4.
Women aged 40-49 years were 3.65 [AOR = 3.65, 95% CI=1.20, 11.07] times more likely to receive cervical screening services when compared to women aged ≤29 years old.
This study found that women who lived in urban areas were 3.49 times [AOR = 3.49, 95%CI=1.64, 7.44] more likely to receive cervical cancer screening service uptake as compared to those who lived in rural areas.
The odds of cervical cancer screening service uptake among those having educational level college and above were 3.04 times [AOR = 3.04, 95% CI: 1.05, 8.80] higher as compared to those who had informal education. Also, women who had good knowledge about cervical cancer were 4 times [AOR 3.9=, 95%CI: 1.70, 8.83] more likely to be screened as compared to those who had poor knowledge about cervical cancer.
Table 4. Bivariate and multi-variable analysis of selected variables with cervical cancer screening uptake among HIV-positive women in public health Facility in Waliso Town, Oromia, Ethiopia, 2024.
Variables | | Screening service uptake | COR [95% CI] | P<.25 | AOR [95% CI] | P<.05 |
Yes | No |
Age category | ≤29 | 6 | 62 | 1 | | 1 | |
30-39 | 15 | 116 | 1.33 [.49, 3.61] | .56 | 1.757 [.57, 5.33] | .320 |
40-49 | 20 | 74 | 2.79 [1.05, 7.38] | .03 | 3.65 [1.20, 11.07] | .022** |
≥50 | 6 | 92 | .67 [.20, 2.18] | .51 | .94 [.26, 3.42] | .936 |
Area of residence | Rural | 13 | 196 | 1 | | 1 | |
Urban | 34 | 148 | 3.46 [1.76, 6.79] | .000 | 3.49 [1.64, 7.44] | .001** |
The educational level of woman | No formal education | 9 | 98 | 1 | | | |
Primary | 13 | 121 | 1.17 [.48, 2.85] | .73 | 1.05 [.39, 2.82] | .909 |
Secondary | 10 | 95 | 1.14 [.44, 2.94] | .77 | .60 [.21, 1.75] | .359 |
collage and above | 15 | 30 | 5.4 [2.16, 13.69] | .00 | 3.04 [1.05, 8.80] | .040** |
Knowledge status | Poor | 15 | 262 | 1 | | 1 | |
Good | 32 | 82 | 6.81 [3.51, 13.2] | .000 | 3.9 [1.70, 8.83] | .001** |
Keys: ** = Statistically significant at p<0.05; 1=Reference; COR=Crude Odds Ratio; Adjusted Odds Ratio and 95% CI = 95% Confidence Interval.
4. Discussion
This study aimed to assess the uptake of cervical cancer screening and associated factors among HIV-positive women at a public hospital in North Shewa Zone, Oromia, Ethiopia, 2024 The results of this study found that only 12% with [95% CI 9.1%- 15%] of women had utilized cervical cancer screening. This study was in line with the study conducted in Taiwan 14.7%
| [25] | Y. C. Chen et al., “Low papanicolaou smear screening rate of women with hiv infection: A nationwide population-based study in Taiwan, 2000-2010,” J. Women’s Heal., vol. 22, no. 12, pp. 1016-1022, 2018, https://doi.org/10.1089/jwh.2012.4127 |
[25]
, Addis Ababa, 11.5%
| [26] | Belete et al., “Willingness and acceptability of cervical cancer screening among women living with HIV / AIDS in Addis Ababa, Ethiopia : a cross sectional study,” Gynecol. Oncol. Res. Pract., pp. 4-9, 2015, https://doi.org/10.1186/s40661-015-0012-3 |
[26]
, and Northwest Ethiopia 10%
| [22] | Nega et al., “Low uptake of cervical cancer screening among HIV positive women in Gondar University referral hospital, Northwest Ethiopia : cross-sectional study design,” pp. 1-7, 2018. |
[22]
.
Nevertheless, the finding of this study was lower than the study conducted in Northern Italy 91%
| [27] | L. D. Maso, S. Franceschi, M. Lise, P. S. De Bianchi, J. Polesel, and F. Ghinelli, “Self-reported history of Pap-smear in HIV-positive women in Northern Italy : a cross-sectional study,” 2018. |
[27]
, Ontario, Canada 68%
, in Côte d’Ivoire 72.5%
| [29] | B. Tchounga et al., “Cervical cancer screening uptake and correlates among HIV-infected women : a cross-sectional survey in Côte d ’ Ivoire, West Africa,” pp. 3-5, 2019, https://doi.org/10.1136/bmjopen-2019-029882 |
[29]
, Estonia 61.45%
| [30] | M. Fitzpatrick et al., “Knowledge, attitudes, and practices of cervical Cancer screening among HIV-positive and HIV-negative women participating in human papillomavirus screening in rural Zimbabwe,” BMC Womens. Health, vol. 20, no. 1, pp. 1-10, 2020, https://doi.org/10.1186/s12905-020-01017-2 |
[30]
. The probable explanation for the observed discrepancy might be because the difference in uptake of cervical cancer screening is attributed to the difference in socio-demographic status, geographical barriers, availability, and accessibility of services. Another probable explanation might be the ineffectiveness of a health information system (HIS) on a routine collection of essential data and generation of regular monitoring reports at the health-facility level.
The result of this study this study found that women aged 40-49 years were positively associated with cervical cancer screening when compared to women aged ≤29 years old. It is concurrent with studies in Taiwan
| [25] | Y. C. Chen et al., “Low papanicolaou smear screening rate of women with hiv infection: A nationwide population-based study in Taiwan, 2000-2010,” J. Women’s Heal., vol. 22, no. 12, pp. 1016-1022, 2018, https://doi.org/10.1089/jwh.2012.4127 |
[25]
, and Côte d’Ivoire
| [29] | B. Tchounga et al., “Cervical cancer screening uptake and correlates among HIV-infected women : a cross-sectional survey in Côte d ’ Ivoire, West Africa,” pp. 3-5, 2019, https://doi.org/10.1136/bmjopen-2019-029882 |
[29]
. This is explained as women’s age increases, the probability of getting information about cervical cancer and its screening will be increased, which leads them to use cervical cancer screening services and the chance to have more contact with health facilities increases as age increases.
Similarly, the finding of this study showed that the odds of cervical screening service uptake among those having an educational level of college and above were positively associated as compared to those who had informal education. This study finding is concurrent with studies done in Ghana
| [31] | N. I. Ebu, “Socio-demographic characteristics influencing cervical cancer screening intention of HIV-positive women in the central region of Ghana,” Gynecol. Oncol. Res. Pract., vol. 5, no. 1, pp. 3-9, 2018, https://doi.org/10.1186/s40661-018-0060-6 |
[31]
, Côte d’Ivoire
| [29] | B. Tchounga et al., “Cervical cancer screening uptake and correlates among HIV-infected women : a cross-sectional survey in Côte d ’ Ivoire, West Africa,” pp. 3-5, 2019, https://doi.org/10.1136/bmjopen-2019-029882 |
[29]
, This is explained by the education enhances the knowledge of screening services and access to communicable disease and reproductive health information that might help women to utilize screening to the recommended time. Education might lead to an increased focus on preventative care and a decrease in health-risk behaviors.
According to the findings of this study revealed that, there is a sizable difference between rural and urban women's rates of cervical cancer screening uptake. Women who lived in urban areas were positively associated to receive cervical cancer screening services uptake as compared to those who lived in rural areas. This is supported by a study done in the United States of America
| [17] | L. R. B. Locklar and D. P. Do, “Rural-urban differences in HPV testing for cervical cancer screening.,” J. Rural Heal. Off. J. Am. Rural Heal. Assoc. Natl. Rural Heal. Care Assoc., Sep. 2021, https://doi.org/10.1111/jrh.12615 |
[17]
, in Ethiopia
| [32] | A. Oncol, R. Treat, T. Gelibo, L. Roets, T. Getachew, and A. Bekele, “Advances in Oncology Research and Treatments Coverage and Factors Associated with Cervical Cancer Screening : Results from a Population-Based WHO Steps Study in Ethiopia.,” vol. 1, no. 2, pp. 1-5, 2017. |
[32]
. This is explained by women of urban dwellers were more accessible to information and might have more knowledge about the need to be screened.
Furthermore, the finding of this study showed that knowledge about cervical cancer screening was another significant factor in the uptake of cervical cancer screening among HIV-positive women. This study found that women who had good knowledge about cervical cancer were positively associated with cervical cancer screening as compared to those who had poor knowledge about cervical cancer. This is supported by research done in Northern Tanzania
| [19] | D. Mrema and J. Ngocho, “Uptake of Cervical Cancer Screening and the Associated Factors Among Women Living With HIV in Northern Tanzania,” 2021. |
[19]
, Ethiopia
| [33] | B. D. Mekonnen, “Cervical Cancer Screening Uptake and Associated Factors among HIV-Positive Women in Ethiopia : A Systematic Review and Meta-Analysis,” vol. 2020, pp. 12-15, 2020. |
[33]
, Hawassa town, Ethiopia
| [20] | Assefa et al., “Cervical cancer screening service utilization and associated factors among HIV positive women attending adult ART clinic in public health facilities, Hawassa town, Ethiopia : a cross-sectional study,” vol. 5, pp. 1-11, 2019. |
[20]
, and Addis Ababa city
. The possible explanation might be being aware of disease-associated risk behaviors may promote prevention strategies, sustain healthy lifestyles and positive choices for seeking screening services.
5. Limitation
Since the data were collected from patients only attending hospitals where a cervical cancer screening program is available, the findings of this study might not be generalized to all age-eligible women for cervical cancer screening receiving in public health institutions in the public health Facility in Waliso Town, zone. Finally, during the interview, very few women had trouble remembering how they had previously been exposed to risk factors.
6. Conclusion
The finding of this study showed that nearly one in ten HIV-positive women was screened. The main factors that significantly associated with cervical cancer screening were: age, being an urban resident, having screening service information, and having good knowledge about cervical cancer. and poor knowledge, service interruption and rumor were barrier of uptake of cervical cancer screening. All age eligible women having ART follow-up should utilize for cervical cancer screening services, creating awareness on benefit of cervical cancer screening and advocacy for cervical cancer prevention. Health facility should decreases cervical cancer screening services interruption. Work hard to empower rural women with health education which enhances the uptake of recommended cervical cancer screening.
Abbreviations
ART | Anti-Retroviral Therapy |
HPV | Human-Papilloma Virus |
IARC | International Agency for Research on Cancer |
STI | Sexually Transmitted Infection |
WLHIV | Women Living with Human Immune Virus |
Acknowledgments
We would like to thank Salale University, college of health science, Department of Midwifery and data collectors for their contribution to accomplishing this research.
Author Contributions
Bacha Merga Chuko: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing
Mitiku Yonas: Data curation, Investigation, Resources, Validation, Writing - review & editing
Mulugeta Feyisa: Investigation, Resources, Validation
Gebreyes Mengistu: Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing - original draft, Formal Analysis, Writing - review& editing
Consent
Informed consent was taken from every study participant before the actual data collection started.
Data Availability Statement
The corresponding author is willing to provide the dataset that was used in this study based upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
WHO, WHO framework for strengthening and scaling- up of services for the management of invasive cervical cancer. 2020.
|
| [2] |
R. C. Christina, What Every Woman Should Know about Cervical Cancer. 2018.
|
| [3] |
WHO, “New WHO recommendations on screening and treatment to prevent cervical cancer among women living with HIV Policy brief,” vol. 2020, pp. 1-6, 2020,
https://doi.org/10.3322/caac.21660.3
|
| [4] |
ACOG, “Cervical Cancer Screening,” no. May, p. 20024, 2021.
|
| [5] |
World Health Organization, Global strategy to accelerate the elimination of cervical cancer as a public health problem and its associated goals and targets for the period 2020 - 2030, vol. 2, no. 1. 2021.
|
| [6] |
WHO, Global strategy to accelerate the elimination of cervical cancer as a public health problem. 2020.
|
| [7] |
Fmoh, “National Cervical Cancer Prevention Training Package Participant Manual,” 2015.
|
| [8] |
ETHIOPIA ICO/IARC on HPV report, “Human Papillomavirus and Related Diseases Report,” no. October, 2021.
|
| [9] |
UNAIDS, “Data 2017,” Program. HIV/AIDS, pp. 1-248, 2017.
|
| [10] |
D. Stelzle et al., “Estimates of the global burden of cervical cancer associated with HIV,” Lancet Glob. Heal., vol. 9, no. 2, pp. e161-e169, 2021,
https://doi.org/10.1016/S2214-109X(20)30459-9
|
| [11] |
S. Menon et al., “Associations between highly active antiretroviral therapy and the presence of HPV, premalignant and malignant cervical lesions in sub-Saharan Africa, a systematic review: Current evidence and directions for future research,” BMJ Open, vol. 7, no. 8, 2017,
https://doi.org/10.1136/bmjopen-2016-015123
|
| [12] |
L. G. Bona et al., “Economic Burden of Cancer on Cancer Patients Treated at Hawassa University Comprehensive Specialized Hospital,” Cancer Control, vol. 28, pp. 1-8, 2021,
https://doi.org/10.1177/10732748211009252
|
| [13] |
R. S. Chambuso, E. Kaambo, and S. Stephan, “Observed Age Difference and Clinical Characteristics of Invasive Cervical Cancer Patients in Tanzania; A Comparison between HIV-Positive and HIV-Negative Women,” J. Neoplasm, vol. 02, no. 03, 2017,
https://doi.org/10.21767/2576-3903.100025
|
| [14] |
N. Cancer and C. Plan, “FEDERAL MINISTRY OF HEALTH,” no. October 2015, 2020.
|
| [15] |
WHO, “Cervical cancer profile,” no. 2020, p. 2021, 2021.
|
| [16] |
Woldetsadik et al., “Socio-demographic characteristics and associated factors influencing cervical cancer screening among women attending in St. Paul’ s Teaching and Referral Hospital,” pp. 1-9, 2020.
|
| [17] |
L. R. B. Locklar and D. P. Do, “Rural-urban differences in HPV testing for cervical cancer screening.,” J. Rural Heal. Off. J. Am. Rural Heal. Assoc. Natl. Rural Heal. Care Assoc., Sep. 2021,
https://doi.org/10.1111/jrh.12615
|
| [18] |
A. M. Mugassa and G. Frumence, “Factors influencing the uptake of cervical cancer screening services in Tanzania: A health system perspective from national and district levels,” Nurs. Open, vol. 7, no. 1, pp. 345-354, 2020,
https://doi.org/10.1002/nop2.395
|
| [19] |
D. Mrema and J. Ngocho, “Uptake of Cervical Cancer Screening and the Associated Factors Among Women Living With HIV in Northern Tanzania,” 2021.
|
| [20] |
Assefa et al., “Cervical cancer screening service utilization and associated factors among HIV positive women attending adult ART clinic in public health facilities, Hawassa town, Ethiopia : a cross-sectional study,” vol. 5, pp. 1-11, 2019.
|
| [21] |
S. Getachew, E. Getachew, M. Gizaw, W. Ayele, A. Addissie, and E. J. Kantelhardt, “Cervical cancer screening knowledge and barriers among women in Addis Ababa, Ethiopia,” PLoS One, vol. 14, no. 5, pp. 1-13, 2019,
https://doi.org/10.1371/journal.pone.0216522
|
| [22] |
Nega et al., “Low uptake of cervical cancer screening among HIV positive women in Gondar University referral hospital, Northwest Ethiopia : cross-sectional study design,” pp. 1-7, 2018.
|
| [23] |
S. Shiferaw, A. Addissie, M. Gizaw, S. Hirpa, and W. Ayele, “Cancer Medicine,” pp. 1-10, 2018,
https://doi.org/10.1002/cam4.1334
|
| [24] |
M. Tavakol and R. Dennick, “Making sense of Cronbach’s alpha,” Int. J. Med. Educ., vol. 2, pp. 53-55, 2011,
https://doi.org/10.5116/ijme.4dfb.8dfd
|
| [25] |
Y. C. Chen et al., “Low papanicolaou smear screening rate of women with hiv infection: A nationwide population-based study in Taiwan, 2000-2010,” J. Women’s Heal., vol. 22, no. 12, pp. 1016-1022, 2018,
https://doi.org/10.1089/jwh.2012.4127
|
| [26] |
Belete et al., “Willingness and acceptability of cervical cancer screening among women living with HIV / AIDS in Addis Ababa, Ethiopia : a cross sectional study,” Gynecol. Oncol. Res. Pract., pp. 4-9, 2015,
https://doi.org/10.1186/s40661-015-0012-3
|
| [27] |
L. D. Maso, S. Franceschi, M. Lise, P. S. De Bianchi, J. Polesel, and F. Ghinelli, “Self-reported history of Pap-smear in HIV-positive women in Northern Italy : a cross-sectional study,” 2018.
|
| [28] |
A. N. Burchell et al., “PT US CR,” Prev. Med. (Baltim)., 2017,
https://doi.org/10.1016/j.ypmed.2017.11.023
|
| [29] |
B. Tchounga et al., “Cervical cancer screening uptake and correlates among HIV-infected women : a cross-sectional survey in Côte d ’ Ivoire, West Africa,” pp. 3-5, 2019,
https://doi.org/10.1136/bmjopen-2019-029882
|
| [30] |
M. Fitzpatrick et al., “Knowledge, attitudes, and practices of cervical Cancer screening among HIV-positive and HIV-negative women participating in human papillomavirus screening in rural Zimbabwe,” BMC Womens. Health, vol. 20, no. 1, pp. 1-10, 2020,
https://doi.org/10.1186/s12905-020-01017-2
|
| [31] |
N. I. Ebu, “Socio-demographic characteristics influencing cervical cancer screening intention of HIV-positive women in the central region of Ghana,” Gynecol. Oncol. Res. Pract., vol. 5, no. 1, pp. 3-9, 2018,
https://doi.org/10.1186/s40661-018-0060-6
|
| [32] |
A. Oncol, R. Treat, T. Gelibo, L. Roets, T. Getachew, and A. Bekele, “Advances in Oncology Research and Treatments Coverage and Factors Associated with Cervical Cancer Screening : Results from a Population-Based WHO Steps Study in Ethiopia.,” vol. 1, no. 2, pp. 1-5, 2017.
|
| [33] |
B. D. Mekonnen, “Cervical Cancer Screening Uptake and Associated Factors among HIV-Positive Women in Ethiopia : A Systematic Review and Meta-Analysis,” vol. 2020, pp. 12-15, 2020.
|
Cite This Article
-
APA Style
Chuko, B. M., Yonas, M., Feyisa, M., Mengistu, G. (2025). Uptake of Cervical Cancer Screening and Associated Factors Among HIV-Positive Women Attending Public Health Facility in Waliso Town, Ethiopia. International Journal of HIV/AIDS Prevention, Education and Behavioural Science, 11(2), 68-77. https://doi.org/10.11648/j.ijhpebs.20251102.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Chuko, B. M.; Yonas, M.; Feyisa, M.; Mengistu, G. Uptake of Cervical Cancer Screening and Associated Factors Among HIV-Positive Women Attending Public Health Facility in Waliso Town, Ethiopia. Int. J. HIV/AIDS Prev. Educ. Behav. Sci. 2025, 11(2), 68-77. doi: 10.11648/j.ijhpebs.20251102.11
Copy
|
Download
AMA Style
Chuko BM, Yonas M, Feyisa M, Mengistu G. Uptake of Cervical Cancer Screening and Associated Factors Among HIV-Positive Women Attending Public Health Facility in Waliso Town, Ethiopia. Int J HIV/AIDS Prev Educ Behav Sci. 2025;11(2):68-77. doi: 10.11648/j.ijhpebs.20251102.11
Copy
|
Download
-
@article{10.11648/j.ijhpebs.20251102.11,
author = {Bacha Merga Chuko and Mitiku Yonas and Mulugeta Feyisa and Gebreyes Mengistu},
title = {Uptake of Cervical Cancer Screening and Associated Factors Among HIV-Positive Women Attending Public Health Facility in Waliso Town, Ethiopia},
journal = {International Journal of HIV/AIDS Prevention, Education and Behavioural Science},
volume = {11},
number = {2},
pages = {68-77},
doi = {10.11648/j.ijhpebs.20251102.11},
url = {https://doi.org/10.11648/j.ijhpebs.20251102.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijhpebs.20251102.11},
abstract = {Introduction Cervical cancer screening is used to find changes in the cells of the cervix that could lead to cancer. Despite, screening is one of the secondary preventive strategies, the case is still growing. Therefore, the study aimed to assess the uptake of cervical cancer screening services and associated factors among Women living with human immunodeficiency virus at public health Facility in Waliso Town, Ethiopia, 2024. Methods and materials: A facility- based cross=sectional study done among 396 women was conducted from April 1-June 25, 2024 Systematic random sampling was used to select women for face-to-face interviews. The bivariable and multivariable logistic regression analyses were done. The data were collected through the face-to-face interview by a structured questionnaire. For analysis, the data were entered into Epi data version 4.6 and exported to Statistical Package for the Social Sciences version 26 software. Bivariate analysis for candidate variables selection (p< 0.25) was used. Multivariable analysis for p-value < 0.05 and 95% confidence level were considered as significantly associated. Results: The proportion of cervical cancer screening uptake among HIV-positive women was 12.1%, 95% confidence interval of 9%- 15%. Variables like an age between 40-49 years [AOR = 3.65; 95%CI=1.20, 11.07], having college above educational level [AOR = 3.04; 95% CI: 1.05, 8.80], Urban residents [AOR = 3.49; 95%CI=1.64, 7.44], and having good knowledge [AOR 3.9; 95%CI: 1.70, 8.83] were significantly associated with uptake of cervical cancer screening service. Service interruption, poor awareness, and rumor were barrier of uptake of cervical cancer screening among HIV-positive women. Conclusion and recommendation: The finding of this study showed that only one in ten HIV-positive women was screened. We recommend that increasing women’s knowledge about cervical cancer screening, particularly targeting the younger ones, is crucial to enhance the uptake of screening and promote health education among rural women so that recommended cervical cancer screening can be utilized more effectively.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Uptake of Cervical Cancer Screening and Associated Factors Among HIV-Positive Women Attending Public Health Facility in Waliso Town, Ethiopia
AU - Bacha Merga Chuko
AU - Mitiku Yonas
AU - Mulugeta Feyisa
AU - Gebreyes Mengistu
Y1 - 2025/08/19
PY - 2025
N1 - https://doi.org/10.11648/j.ijhpebs.20251102.11
DO - 10.11648/j.ijhpebs.20251102.11
T2 - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JF - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JO - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
SP - 68
EP - 77
PB - Science Publishing Group
SN - 2575-5765
UR - https://doi.org/10.11648/j.ijhpebs.20251102.11
AB - Introduction Cervical cancer screening is used to find changes in the cells of the cervix that could lead to cancer. Despite, screening is one of the secondary preventive strategies, the case is still growing. Therefore, the study aimed to assess the uptake of cervical cancer screening services and associated factors among Women living with human immunodeficiency virus at public health Facility in Waliso Town, Ethiopia, 2024. Methods and materials: A facility- based cross=sectional study done among 396 women was conducted from April 1-June 25, 2024 Systematic random sampling was used to select women for face-to-face interviews. The bivariable and multivariable logistic regression analyses were done. The data were collected through the face-to-face interview by a structured questionnaire. For analysis, the data were entered into Epi data version 4.6 and exported to Statistical Package for the Social Sciences version 26 software. Bivariate analysis for candidate variables selection (p< 0.25) was used. Multivariable analysis for p-value < 0.05 and 95% confidence level were considered as significantly associated. Results: The proportion of cervical cancer screening uptake among HIV-positive women was 12.1%, 95% confidence interval of 9%- 15%. Variables like an age between 40-49 years [AOR = 3.65; 95%CI=1.20, 11.07], having college above educational level [AOR = 3.04; 95% CI: 1.05, 8.80], Urban residents [AOR = 3.49; 95%CI=1.64, 7.44], and having good knowledge [AOR 3.9; 95%CI: 1.70, 8.83] were significantly associated with uptake of cervical cancer screening service. Service interruption, poor awareness, and rumor were barrier of uptake of cervical cancer screening among HIV-positive women. Conclusion and recommendation: The finding of this study showed that only one in ten HIV-positive women was screened. We recommend that increasing women’s knowledge about cervical cancer screening, particularly targeting the younger ones, is crucial to enhance the uptake of screening and promote health education among rural women so that recommended cervical cancer screening can be utilized more effectively.
VL - 11
IS - 2
ER -
Copy
|
Download