Laryngopharynx is funnel-shaped, wider above & has rich lymphatic supply. These two points are very significant in the management of cancers in this region. These patients present very late, usually in a very poor general condition, often with lymph node metastasis. Many such patients are not fit for major surgery. Advanced cancers can be treated by radical surgery like total laryngopharyngoesophagectomy which solves the swallowing problem. By creating a fistula between the stomach and trachea using a modified Blom-Singer technique, the patient will develop good gastric speech. Radical neck dissection & surgery for thyroid involvement can be combined with the main operation. Gastric pull-up was thought to be not possible earlier. The oesophagus is mobilized by blunt finger dissection from above and from below. Two teams of surgeons operate at the same time, one for the neck for doing total laryngopharyngotomy and, if necessary, radical neck dissection. The second team operates in the abdomen to mobilize the stomach, keeping the right gastroepiploic artery pedicle. Duodenum is mobilized & cocherisation is done. Pyloroplasty is done for drainage purpose. The neck surgeon, by blunt finger dissection, mobilizes the upper part of the thoracic oesophagus and trachea. The abdominal surgeon, by blunt finger dissection, mobilizes the lower oesophagus. Now the two teams work together and the stomach is pulled into the neck through the posterior mediastinum. By bringing the stomach to the neck through the posterior mediastinum, this technique works well, and the stomach, acts as a tamponade to prevent any bleeding in the mediastinum. By using Gluck-Sorensen's incision in the neck, the resulting scar is cosmetically acceptable. In course of time, this method has been used in many centers including ours.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Residual, recurrent and resistant Cancer of Laryngopharynx has to be treated only by surgery if patient’s general condition is good. Because of the proximity of the larynx, the larynx also has to be removed for any radical surgery. Because of the segmental blood supply to the Oesophagus not more than one inch can be mobilized. Hence, we have to remove the entire oesophagus for successful surgical treatment
[12]
A Short practice of Otorhinolaryngology, ENT text - by Ramalingam, Sreeramamurty and Ravi Ramalingam - fifth edition-2020.
[12]
. By creating a fistula between trachea and stomach patient develops good gastric speech.
[14]
JeroenMeulemans, Floor Couvreur, ElineBeckers, Philippe Nafteux Hans Van Veer, Vincent Vander Poorten, Pierre Delaere and Willy Coosemans- Oncologic and Functional outcomes after primary and salvage Laryngopharyngoesophagectomy wit gastric pill-up reconstruction for locally advanced hypopharyngeal squamous cell carcinoma
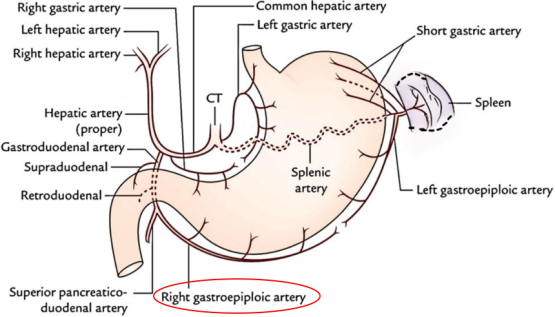
We have to address swallowing and voice problem. Two team of surgeons; one for the neck and upper chest and another for abdominothoracic regions have to operate at the same time. The neck surgeon does total laryngopharyngectomy with one or both sides radical neck dissection and single lobectomy or total thyroidectomy depending on the presence of neck nodes and thyroid involvement. The abdominothoracic team mobilizes the stomach with right gastroepiploic artery pedicle
[13]
D R Edwards, L Pope and S Berry – Survival and function following pharyngolaryngo- oesophagectomy in wales: a twelve- year case series.
[13]
(Figure 1). By finger dissection from above and from below the oesophagus is mobilized all around and by traction on the oesophagus the stomach is pulled through the posterior mediastinum into the neck. Oesophagus is removed at the cardiac end leaving a specimen of larynx, pharynx with proximal part of trachea and oesophagus (Figure 2).
Figure 2. The postoperative specimen showing Larynx, Pharynx and entire oesophagus.
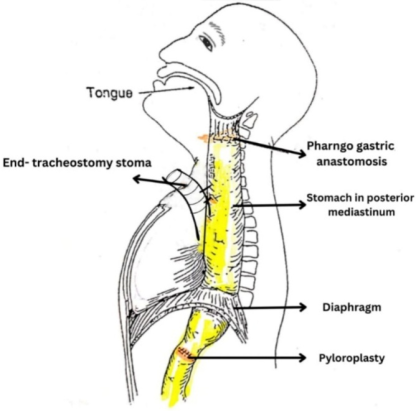
Suitable opening is made in the fundus of the stomach and is anastomosed to the remaining part of the pharynx and base of tongue. Remaining lower part of trachea is brought out and stitched to the skin as end tracheostomy (Figure 3).
In every case, pyloroplasty was done for drainage purpose, since both vagusnerve have been divided.
Figure 3. Final outcome of the operation with Pharyngogastric anastomosis &Pyloroplasty.
Very early cancer of Laryngopharynx is rarely diagnosed because of the functional nature of laryngopharynx. If it is diagnosed early complete treatment may be possible by radio therapy with or without chemotherapy. Residual, recurrent & resistant cancers can be managed successfully by total Laryngopharyngoesophagectomy solving the swallowing problem
[15]
Anthony J. Maniglia, MD, Steven B. Leder PhD, W. Jarrard Goodwin, Jr., MD, Robert Sawyer, MD, and Clarence T. Sasaki, MD- Tracheogastric puncture for vocal rehabilitation following total pharyngolarygoesophagectomy 1989.
[15]
.
When the Blom-Singer vocal prosthesis was first introduced in 1980, 90% of a series of 60 patients treated following laryngectomy had their voices successfully restored. Expired air is redirected into the oesophagus by the prosthesis, which functions as a one-way valve inside a surgically made tracheoesophageal fistula
[2]
Singer MI, Blom ED. An endoscopic technique for restoration of voice after laryngectomy. AnnOtolRhinolLaryngol 1980; 89: 529-33.
[2]
. Panje in 1981 described similar prosthesis
[3]
Panje WR. Prosthetic vocal rehabilitation following laryn-gectomy. The voice button. AnnOtolRhinolLaryngol 1981; 90: 116-20.
[3]
.
By using a modified Blom-Singer technique a puncture and fistula is created between trachea and stomach. This may be primary at the time of original operation or sometime later as a secondary procedure when patients general condition stabilises and improves
[2]
Singer MI, Blom ED. An endoscopic technique for restoration of voice after laryngectomy. AnnOtolRhinolLaryngol 1980; 89: 529-33.
[10]
Milford CA, Perry A, Cheesman AD. A British experience of surgical voice restoration as a primary procedure. Arch Oto-laryngol Head Neck Surg 1988; 114: 1419-21.
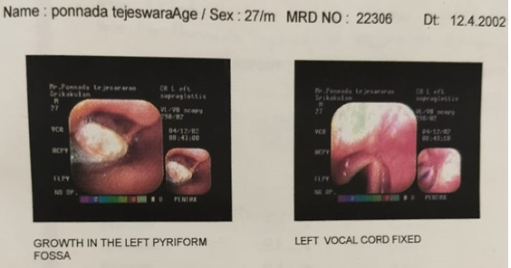
Figure 4. Advanced cancer of left pyriform fossa with left vocal cord involvement.
A27-year-old male, Mr. P, teacher by profession presented to us on 20th April 2002 with advanced left pyriform fossa growth involving one half of the larynx, post cricoid region, and cervical oesophagus. He was referred to us by an ENT surgeon. The patient is from Tholapi Village, Srikakulam district of Andhra Pradesh State in India. Presenting complaints were difficult and painful swallowing of solids, blood-stained sputum, and change of voice. The patient was not addicted to alcohol or smoking.
Indirect laryngoscopy revealed an ulceroproliferative growth involving Left Pyriform fossa. Left vocal cord was not visualised and right vocal cord found to be normal. Endoscopy showed a large ulceroproliferative growth in the left half of laryngopharynx involving the left pyriform fossa, post cricoid area and cervical oesophagus with fixity of left vocal cord (Figure 4). The scope was passed with difficulty through the cricopharynx up to the oesophagus.
Direct Laryngoscopy and biopsy was done. Biopsy report showed Well-Differentiated Squamous Cell Carcinoma.
4. Diagnosis: Carcinoma of the Left Pyriform Fossa with Extension to the Larynx and Cervical Oesophagus
Figure 5. Patient T with tracheostome, 23 years after pharyngolaryngo esophagus and trachea gastric fistula.
CT scan of upper neck and thorax was done which showed irregular growth in the laryngopharynx. The mass measured 3.3 x 3.2cms and inferiorly the mass extended into the post cricoid region and cervical oesophagus up to the D2 vertebral level (Cranio-caudal extent = 9cms). The mass infiltrated the aryepiglottic fold, Left pyriform sinus and the vocal cord on the left side. There were no significant lymphadenopathy in the neck and superior mediastinum. Both vallecula and the right pyriform fossa were normal.
Patient underwent total laryngopharyngoesophagectomy on 22/04/2002 since suitable radiotherapy was not available
[8]
Cheesman AD, Knight J, McIvor J, Perry A. Tracheo-oesophageal puncture speech. An assessment technique for failed oesophageal speakers. J LaryngolOtol 1986; 100: 191-9.
[8]
. For vocal rehabilitation a fistula was created between the stomach and trachea and later speech therapy was given (Figure 5).
Blom - Singer introduced the tracheoesophageal puncture in 1980 which is kept open by a duckbill process
[2]
Singer MI, Blom ED. An endoscopic technique for restoration of voice after laryngectomy. AnnOtolRhinolLaryngol 1980; 89: 529-33.
[2]
. This involves initial cost of buying the suitable prosthesis and frequent cleaning of the prosthesis. In the case being presented the patient once had an experience of the prosthesis slipping into the trachea producing severe cough, bleeding and other symptoms like difficulty in breathing.
Though the prosthesis was removed successfully from the trachea the patient did not want to have the prosthesis again. Instead, by applying slight pressure at the site of the tracheogastric fistula he avoids any aspirations of gastric contents into the trachea
[5]
Harrison DFN. Surgical repair in hypopharyngeal and cervical esophageal cancer. Analysis of 162 patients. Ann OtolRhinolLaryngol 1981; 90: 372-5.
[5]
. Unlike the tracheoesophageal fistula there is less chance of gastric contents aspirating into the trachea. Because of the volume of stomach, absence of sphincter, pyloroplasty and erect posture of stomach the stomach empties quickly and there is no stasis of stomach contents at the site of tracheogastric fistula. In tracheoesophageal fistula if stomach is full there are more chances of leak around the prosthesis. He has been living without the prosthesis for over 20 years. This way we can call this as Modified Blom Singer technique as applicable to gastrotracheal fistula. Blom singer reported 90 percent success rate after tracheoesophageal fistula for laryngectomy patients.
By using Gluck Sorenson incision, the patient has cosmetically acceptable scar in the neck. He is well and living 23 years after surgery. He has developed very good gastric speech and he is working as a teacher and leading a normal life as government servant in Srikakulam village in Andhra Pradesh, India. By virtue of his job, he is financially and morally good & has been supporting his family very well. His two sons have become engineers since he has been able to financially support their studies.
Table 1. BLOM SINGER TECHNIQUE AND MODIFIED BLOM SINGER TECHNIQUE.
BLOM SINGER TECHNIQUE
MODIFIED BLOM SINGER TECHNIQUE
Tracheoesophageal puncture and prosthesis
Tracheogastric puncture and fistula
Initial cost and recurrent cost of buying the prosthesis
No prosthetic cost
Frequent cleaning of the prosthesis to prevent blocking and fungus formation
No cleaning required
Leaking of oesophageal and gastric contents around the prosthesis because of GERD (Gastroesophageal Reflux Disease)
No leakage since there is no gastric contents at the site of fistula
Speech is good
Speech is good with slight gurgling because of the volume of the stomach
Stomal problems like stenosis and need for tracheostomy tube care
No stomal problem. No need for tracheostomy tube and its care
Simulates neoglottisphonatoria of Staffieri
No resemblance to neoglottisphonatoria of Staffieri
5. Discussion
Laryngopharyngeal carcinoma accounts for approximately 15% of all head and neck carcinomas and has poor prognosis. Laryngopharyngeal malignancies can originate from a number of sub-sites, including the pyriform sinus (80%), post cricoid (13.5%), and posterior pharyngeal wall (6.5%). When they originate from the posterior pharyngeal wall, they can restrict the upper airway and cause dyspnoea. The two main risk factors for the development oflaryngopharyngeal carcinoma are smoking and alcohol
[11]
Scott brown's Otorhinolaryngology, Head and Neck Surgery - the seventh edition published in great Britain in 2008 by Hodder Arnold.
[11]
.
The incidence of hypopharyngeal cancer is low, with 80,000 new cases (or 0.4% of all new cases worldwide) and 35,000 cancer-related deaths (or 0.4% of all cancer-related mortality) each year. Globally, there are 0.8% cases of laryngopharyngeal cancer for every 100,000 people (0.3 for women and 1.4 for men). Regional differences exist in the incidence of hypopharyngeal cancer; South-Central Asia has the greatest incidence, followed by Central and Eastern Europe, Western Europe, and North America.
In 95% of cases, the most prevalent histology found was squamous cell carcinoma originating from the mucosal layer. The other instances are adenocarcinoma, sarcoma, and non-epidermoid carcinoma. Local invasion and lymphatic dissemination are the hallmarks of hypopharyngeal tumors.
At the time of diagnosis, 70% of patients have involvement of lymph nodes. 50% of these cases die within 1 year Ranger et all (Personal communication)
[7]
Le Quesne LP, Ranger D. Pharyngolaryngectomy with immediate pharyngogastric anastomosis. Br J Surg 1966; 53: 105-9.
[8]
Cheesman AD, Knight J, McIvor J, Perry A. Tracheo-oesophageal puncture speech. An assessment technique for failed oesophageal speakers. J LaryngolOtol 1986; 100: 191-9.
[7, 8]
.
Laryngopharyngoesophagectomy and tracheogogastric anastomosis is an effective and established technique for treating extensive hypopharyngeal carcinoma
[8]
Cheesman AD, Knight J, McIvor J, Perry A. Tracheo-oesophageal puncture speech. An assessment technique for failed oesophageal speakers. J LaryngolOtol 1986; 100: 191-9.
[9]
Juarbe C, Shemen L, Eberie R, Klatsky I, Fox M. Primary tracheoesophagealpuncture for voice restoration. Am J Surg 1986; 152: 464-6.
[8, 9]
. The use of the stomach as a means of repair after laryngopharynoesophagectomy was for long considered impracticable. However, in 1960 Ong and Lee reported 3 cases in which this method of repair was used with successful results
[1]
ONG, G. B., and LEE, T. C. (1960)~Br. J. Surg., 48, 193. RANGER, D. (1964), Proc. R. SOC. Med., 57, 1099. THOMAS, A. B. (1960), personal communication. TURNER, G. G. (1936), Lancet, I, 67, 130.
[6]
Ong GB, Lee TC. Pharyngogastric anastomosis after oesophagopharyngectomy for carcinoma of the hypopharynx and cervical oesophagus. Br J Surg 1960; 48: 193-200.
[1, 6]
. A larger series of 10 patients was reported by Le Quesne and Ranger' in 1966
[4]
Harrison DFN, Thompson AE. Pharyngolaryngoesophagectomy with pharyngogastric anastomosis for cancer of the hypopharynx: review of 101 operations. Head Neck Surg 1986; 8: 418-28.
[7]
Le Quesne LP, Ranger D. Pharyngolaryngectomy with immediate pharyngogastric anastomosis. Br J Surg 1966; 53: 105-9.
[4, 7]
. The advantages of using the stomach include its good vascular supply, its ease of suture to the remaining pharynx, and the wide anastomosis that can be made and less or almost no chance of stenosis at the pharyngogastric anastomosis.
However, there may be patients who have undergone operations on the stomach like gastrojejunostomy or gastrectomy (Billroth operation) the stomach is too small and for that reason a barium-meal examination is carried out before operation to assess the size of the stomach.
6. Duration of Operation
It is an operation requiring considerable time, Initially abdominal surgeon used to start the operation at 8 am and finish by 12 noon. The neck surgeon used to start at 12 noon and finish by around 4.00 pm. Both teams used to work together from 4pm to 5.30 pm. The total duration was about 8 hours and 30 minutes.
However, during the course of time from 1969 to 1994, doing 90 cases; (10 cases at Middlesex hospital, 35 cases at KKR ENT Hospital, Kilpauk, Chennai, India and 45 cases at Government general hospital, Chennai, India) reduced the duration of the operation by starting neck and abdominal operation at the same time. Average time taken is 5 hours.
The main advantages of this form of repair are that it can restore normal swallowing within few days, it is free of the risk of late stenosis, and fistula formation is unlikely.
7. Material or Method
It is a retrospective study. Total of 90 cases are included, period of study -1967 to 1994.
10 cases at the Middle Sex Hospital, London, U.K.
35 cases at KKR ENT Hospital, Kilpauk, Chennai, India.
45 cases at Government Hospital, Chennai, India.
Of the Total 90 cases TGP (Tracheo Gastric Puncture was done in 15 cases. 11 of them developed gastric speech, 5 of them had fairly good speech, rest 6 of them developed some speech better after speech than electrolarynx.
Abbreviations
KKR
Kombupalayam Komarappa Gounder Ramalingam
GERD
Gastroesophageal Reflux Disease
Acknowledgments
We wish to express our appreciation to all those who have helped in the treatment of these patients especially Dr. RajanSanthosham (Thoracic Surgeon), Dr. Raja Sundaram (Surgical Oncologist), Dr. Pacifica Simon and Dr. SreeRamamoorthy.
Author Contributions
Komarappa Gounder Ramalingam: Conceptualization
Ravi Ramalingam: Data Curation
Raja Sundaram: Formal Analysis
Ramakrishnamma Raju: Investigation
Wasim Khan: Methodology
Ravi Rajan: Supervision
Aravind Thulaseedharan Indira: Resources
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
ONG, G. B., and LEE, T. C. (1960)~Br. J. Surg., 48, 193. RANGER, D. (1964), Proc. R. SOC. Med., 57, 1099. THOMAS, A. B. (1960), personal communication. TURNER, G. G. (1936), Lancet, I, 67, 130.
[2]
Singer MI, Blom ED. An endoscopic technique for restoration of voice after laryngectomy. AnnOtolRhinolLaryngol 1980; 89: 529-33.
[3]
Panje WR. Prosthetic vocal rehabilitation following laryn-gectomy. The voice button. AnnOtolRhinolLaryngol 1981; 90: 116-20.
[4]
Harrison DFN, Thompson AE. Pharyngolaryngoesophagectomy with pharyngogastric anastomosis for cancer of the hypopharynx: review of 101 operations. Head Neck Surg 1986; 8: 418-28.
[5]
Harrison DFN. Surgical repair in hypopharyngeal and cervical esophageal cancer. Analysis of 162 patients. Ann OtolRhinolLaryngol 1981; 90: 372-5.
[6]
Ong GB, Lee TC. Pharyngogastric anastomosis after oesophagopharyngectomy for carcinoma of the hypopharynx and cervical oesophagus. Br J Surg 1960; 48: 193-200.
[7]
Le Quesne LP, Ranger D. Pharyngolaryngectomy with immediate pharyngogastric anastomosis. Br J Surg 1966; 53: 105-9.
[8]
Cheesman AD, Knight J, McIvor J, Perry A. Tracheo-oesophageal puncture speech. An assessment technique for failed oesophageal speakers. J LaryngolOtol 1986; 100: 191-9.
[9]
Juarbe C, Shemen L, Eberie R, Klatsky I, Fox M. Primary tracheoesophagealpuncture for voice restoration. Am J Surg 1986; 152: 464-6.
[10]
Milford CA, Perry A, Cheesman AD. A British experience of surgical voice restoration as a primary procedure. Arch Oto-laryngol Head Neck Surg 1988; 114: 1419-21.
[11]
Scott brown's Otorhinolaryngology, Head and Neck Surgery - the seventh edition published in great Britain in 2008 by Hodder Arnold.
[12]
A Short practice of Otorhinolaryngology, ENT text - by Ramalingam, Sreeramamurty and Ravi Ramalingam - fifth edition-2020.
[13]
D R Edwards, L Pope and S Berry – Survival and function following pharyngolaryngo- oesophagectomy in wales: a twelve- year case series.
[14]
JeroenMeulemans, Floor Couvreur, ElineBeckers, Philippe Nafteux Hans Van Veer, Vincent Vander Poorten, Pierre Delaere and Willy Coosemans- Oncologic and Functional outcomes after primary and salvage Laryngopharyngoesophagectomy wit gastric pill-up reconstruction for locally advanced hypopharyngeal squamous cell carcinoma
Anthony J. Maniglia, MD, Steven B. Leder PhD, W. Jarrard Goodwin, Jr., MD, Robert Sawyer, MD, and Clarence T. Sasaki, MD- Tracheogastric puncture for vocal rehabilitation following total pharyngolarygoesophagectomy 1989.
Ramalingam, K. G., Ramalingam, R., Sundaram, R., Raju, R., Khan, W., et al. (2026). Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique. International Journal of Otorhinolaryngology, 12(1), 25-30. https://doi.org/10.11648/j.ijo.20261201.15
Ramalingam, K. G.; Ramalingam, R.; Sundaram, R.; Raju, R.; Khan, W., et al. Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique. Int. J. Otorhinolaryngol.2026, 12(1), 25-30. doi: 10.11648/j.ijo.20261201.15
@article{10.11648/j.ijo.20261201.15,
author = {Komarappa Gounder Ramalingam and Ravi Ramalingam and Raja Sundaram and Ramakrishnamma Raju and Wasim Khan and Ravi Rajan and Aravind Thulaseedharan Indira},
title = {Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique},
journal = {International Journal of Otorhinolaryngology},
volume = {12},
number = {1},
pages = {25-30},
doi = {10.11648/j.ijo.20261201.15},
url = {https://doi.org/10.11648/j.ijo.20261201.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20261201.15},
abstract = {Laryngopharynx is funnel-shaped, wider above & has rich lymphatic supply. These two points are very significant in the management of cancers in this region. These patients present very late, usually in a very poor general condition, often with lymph node metastasis. Many such patients are not fit for major surgery. Advanced cancers can be treated by radical surgery like total laryngopharyngoesophagectomy which solves the swallowing problem. By creating a fistula between the stomach and trachea using a modified Blom-Singer technique, the patient will develop good gastric speech. Radical neck dissection & surgery for thyroid involvement can be combined with the main operation. Gastric pull-up was thought to be not possible earlier. The oesophagus is mobilized by blunt finger dissection from above and from below. Two teams of surgeons operate at the same time, one for the neck for doing total laryngopharyngotomy and, if necessary, radical neck dissection. The second team operates in the abdomen to mobilize the stomach, keeping the right gastroepiploic artery pedicle. Duodenum is mobilized & cocherisation is done. Pyloroplasty is done for drainage purpose. The neck surgeon, by blunt finger dissection, mobilizes the upper part of the thoracic oesophagus and trachea. The abdominal surgeon, by blunt finger dissection, mobilizes the lower oesophagus. Now the two teams work together and the stomach is pulled into the neck through the posterior mediastinum. By bringing the stomach to the neck through the posterior mediastinum, this technique works well, and the stomach, acts as a tamponade to prevent any bleeding in the mediastinum. By using Gluck-Sorensen's incision in the neck, the resulting scar is cosmetically acceptable. In course of time, this method has been used in many centers including ours.},
year = {2026}
}
TY - JOUR
T1 - Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique
AU - Komarappa Gounder Ramalingam
AU - Ravi Ramalingam
AU - Raja Sundaram
AU - Ramakrishnamma Raju
AU - Wasim Khan
AU - Ravi Rajan
AU - Aravind Thulaseedharan Indira
Y1 - 2026/05/14
PY - 2026
N1 - https://doi.org/10.11648/j.ijo.20261201.15
DO - 10.11648/j.ijo.20261201.15
T2 - International Journal of Otorhinolaryngology
JF - International Journal of Otorhinolaryngology
JO - International Journal of Otorhinolaryngology
SP - 25
EP - 30
PB - Science Publishing Group
SN - 2472-2413
UR - https://doi.org/10.11648/j.ijo.20261201.15
AB - Laryngopharynx is funnel-shaped, wider above & has rich lymphatic supply. These two points are very significant in the management of cancers in this region. These patients present very late, usually in a very poor general condition, often with lymph node metastasis. Many such patients are not fit for major surgery. Advanced cancers can be treated by radical surgery like total laryngopharyngoesophagectomy which solves the swallowing problem. By creating a fistula between the stomach and trachea using a modified Blom-Singer technique, the patient will develop good gastric speech. Radical neck dissection & surgery for thyroid involvement can be combined with the main operation. Gastric pull-up was thought to be not possible earlier. The oesophagus is mobilized by blunt finger dissection from above and from below. Two teams of surgeons operate at the same time, one for the neck for doing total laryngopharyngotomy and, if necessary, radical neck dissection. The second team operates in the abdomen to mobilize the stomach, keeping the right gastroepiploic artery pedicle. Duodenum is mobilized & cocherisation is done. Pyloroplasty is done for drainage purpose. The neck surgeon, by blunt finger dissection, mobilizes the upper part of the thoracic oesophagus and trachea. The abdominal surgeon, by blunt finger dissection, mobilizes the lower oesophagus. Now the two teams work together and the stomach is pulled into the neck through the posterior mediastinum. By bringing the stomach to the neck through the posterior mediastinum, this technique works well, and the stomach, acts as a tamponade to prevent any bleeding in the mediastinum. By using Gluck-Sorensen's incision in the neck, the resulting scar is cosmetically acceptable. In course of time, this method has been used in many centers including ours.
VL - 12
IS - 1
ER -
Ramalingam, K. G., Ramalingam, R., Sundaram, R., Raju, R., Khan, W., et al. (2026). Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique. International Journal of Otorhinolaryngology, 12(1), 25-30. https://doi.org/10.11648/j.ijo.20261201.15
Ramalingam, K. G.; Ramalingam, R.; Sundaram, R.; Raju, R.; Khan, W., et al. Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique. Int. J. Otorhinolaryngol.2026, 12(1), 25-30. doi: 10.11648/j.ijo.20261201.15
@article{10.11648/j.ijo.20261201.15,
author = {Komarappa Gounder Ramalingam and Ravi Ramalingam and Raja Sundaram and Ramakrishnamma Raju and Wasim Khan and Ravi Rajan and Aravind Thulaseedharan Indira},
title = {Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique},
journal = {International Journal of Otorhinolaryngology},
volume = {12},
number = {1},
pages = {25-30},
doi = {10.11648/j.ijo.20261201.15},
url = {https://doi.org/10.11648/j.ijo.20261201.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20261201.15},
abstract = {Laryngopharynx is funnel-shaped, wider above & has rich lymphatic supply. These two points are very significant in the management of cancers in this region. These patients present very late, usually in a very poor general condition, often with lymph node metastasis. Many such patients are not fit for major surgery. Advanced cancers can be treated by radical surgery like total laryngopharyngoesophagectomy which solves the swallowing problem. By creating a fistula between the stomach and trachea using a modified Blom-Singer technique, the patient will develop good gastric speech. Radical neck dissection & surgery for thyroid involvement can be combined with the main operation. Gastric pull-up was thought to be not possible earlier. The oesophagus is mobilized by blunt finger dissection from above and from below. Two teams of surgeons operate at the same time, one for the neck for doing total laryngopharyngotomy and, if necessary, radical neck dissection. The second team operates in the abdomen to mobilize the stomach, keeping the right gastroepiploic artery pedicle. Duodenum is mobilized & cocherisation is done. Pyloroplasty is done for drainage purpose. The neck surgeon, by blunt finger dissection, mobilizes the upper part of the thoracic oesophagus and trachea. The abdominal surgeon, by blunt finger dissection, mobilizes the lower oesophagus. Now the two teams work together and the stomach is pulled into the neck through the posterior mediastinum. By bringing the stomach to the neck through the posterior mediastinum, this technique works well, and the stomach, acts as a tamponade to prevent any bleeding in the mediastinum. By using Gluck-Sorensen's incision in the neck, the resulting scar is cosmetically acceptable. In course of time, this method has been used in many centers including ours.},
year = {2026}
}
TY - JOUR
T1 - Advanced Laryngopharyngeal Cancer – Swallowing and Vocal Rehabilitation by Radical Surgery & Modified Blom Singer Technique
AU - Komarappa Gounder Ramalingam
AU - Ravi Ramalingam
AU - Raja Sundaram
AU - Ramakrishnamma Raju
AU - Wasim Khan
AU - Ravi Rajan
AU - Aravind Thulaseedharan Indira
Y1 - 2026/05/14
PY - 2026
N1 - https://doi.org/10.11648/j.ijo.20261201.15
DO - 10.11648/j.ijo.20261201.15
T2 - International Journal of Otorhinolaryngology
JF - International Journal of Otorhinolaryngology
JO - International Journal of Otorhinolaryngology
SP - 25
EP - 30
PB - Science Publishing Group
SN - 2472-2413
UR - https://doi.org/10.11648/j.ijo.20261201.15
AB - Laryngopharynx is funnel-shaped, wider above & has rich lymphatic supply. These two points are very significant in the management of cancers in this region. These patients present very late, usually in a very poor general condition, often with lymph node metastasis. Many such patients are not fit for major surgery. Advanced cancers can be treated by radical surgery like total laryngopharyngoesophagectomy which solves the swallowing problem. By creating a fistula between the stomach and trachea using a modified Blom-Singer technique, the patient will develop good gastric speech. Radical neck dissection & surgery for thyroid involvement can be combined with the main operation. Gastric pull-up was thought to be not possible earlier. The oesophagus is mobilized by blunt finger dissection from above and from below. Two teams of surgeons operate at the same time, one for the neck for doing total laryngopharyngotomy and, if necessary, radical neck dissection. The second team operates in the abdomen to mobilize the stomach, keeping the right gastroepiploic artery pedicle. Duodenum is mobilized & cocherisation is done. Pyloroplasty is done for drainage purpose. The neck surgeon, by blunt finger dissection, mobilizes the upper part of the thoracic oesophagus and trachea. The abdominal surgeon, by blunt finger dissection, mobilizes the lower oesophagus. Now the two teams work together and the stomach is pulled into the neck through the posterior mediastinum. By bringing the stomach to the neck through the posterior mediastinum, this technique works well, and the stomach, acts as a tamponade to prevent any bleeding in the mediastinum. By using Gluck-Sorensen's incision in the neck, the resulting scar is cosmetically acceptable. In course of time, this method has been used in many centers including ours.
VL - 12
IS - 1
ER -