Abstract
OBJECTIVE: To determine whether qualitative pain characteristics in chronic vulvar discomfort correspond to diagnosis-specific epidermal and dermal histopathological patterns in vulvodynia and vulvar dermatoses. METHODS: This prospective observational sub-analysis of the DATRIV study included 328 women equally stratified into four groups: normal vulva, impaired asymptomatic vulvar skin, vulvodynia, and vulvar dermatoses (n = 82 per group). Pain quality was assessed using structured clinical interviews and categorized as sharp (fast) or dull (slow) descriptors. Vulvar biopsies underwent blinded histopathological evaluation of epidermal architecture and dermal features, including inflammatory infiltrates, fibrosis, vascularity, adnexal structures, nerve fibers, and mast cells. Associations between pain quality, histopathological findings, and symptom duration were analyzed using proportion tests, pairwise comparisons, and multivariate models. RESULTS: Epidermal architecture was largely preserved in normal vulva, impaired asymptomatic skin, and vulvodynia, whereas epidermal thinning, atrophy, and keratinization disorders were predominantly confined to vulvar dermatoses (p < 0.001). Vulvar dermatoses demonstrated a stable inflammatory–fibrotic dermal phenotype characterized by collagen accumulation and hyalinization. In contrast, vulvodynia exhibited a neurovascular–adnexal dermal profile marked by increased nerve fibers, vascular proliferation, sebaceous gland prominence, and increased mast cell density (p < 0.001). Sharp pain descriptors were strongly associated with vulvodynia and, within this group, were significantly more prevalent in cases with subtle epidermal abnormalities. Dull descriptors predominated in vulvar dermatoses and corresponded to structural remodeling. In vulvodynia, longer symptom duration was associated with increased dermal inflammation and vascularity, whereas dermal characteristics in vulvar dermatoses remained stable over time. CONCLUSION: Chronic vulvar discomfort demonstrates diagnosis-specific sensory–histopathological coupling. Vulvodynia is characterized by sharp, fast pain qualities linked to a neurocutaneous dermal phenotype, whereas vulvar dermatoses are dominated by dull, slow, inflammation-driven nociception associated with fibrotic remodeling. Integrating structured pain quality assessment with histopathological evaluation enhances diagnostic differentiation and supports mechanism-oriented stratification and individualized management.
|
Published in
|
Journal of Gynecology and Obstetrics (Volume 14, Issue 2)
|
|
DOI
|
10.11648/j.jgo.20261402.11
|
|
Page(s)
|
50-64 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Chronic Vulvar Discomfort, Vulvodynia, Vulvar Dermatoses, Pain Quality, Histopathology, Peripheral Sensitization,
Inflammatory Remodeling
1. Introduction
Chronic vulvar discomfort (CVD) represents a multifactorial clinical entity encompassing a spectrum of conditions, including vulvodynia and various vulvar dermatoses. These conditions commonly present with persistent pain, burning, itching, and sensory hypersensitivity, often in the absence of clearly identifiable lesions
| [1] | Bornstein J, Goldstein AT, Stockdale CK, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20(2): 126–130.
https://doi.org/10.1097/LGT.0000000000000194 |
| [2] | Leclair CM, Goetsch MF, Korcheva VB, Anderson R, Peters D, Morgan TK. Differences in primary compared with secondary vestibulodynia by immunohistochemistry. Obstet Gynecol. 2011; 117(6): 1307–1313.
https://doi.org/10.1097/AOG.0b013e31821f7db0 |
| [3] | Reed BD, Harlow SD, Legocki LJ, et al. Chronic vulvar pain: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2012; 119(5): 1025–1033.
https://doi.org/10.1097/AOG.0b013e31824c3b8f |
[1-3]
. The diagnostic process remains challenging due to substantial symptom overlap, the frequent lack of visible pathology in early disease stages, and limited awareness among clinicians
| [1] | Bornstein J, Goldstein AT, Stockdale CK, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20(2): 126–130.
https://doi.org/10.1097/LGT.0000000000000194 |
| [4] | Goldstein AT, Pukall CF, Brown C, Bergeron S, Stein A, Kellogg-Spadt S. Vulvodynia: Assessment and Treatment. J Sex Med. 2016 Apr; 13(4): 572-90.
https://doi.org/10.1016/j.jsxm.2016.01.020 |
[1, 4]
. Consequently, many patients experience delayed diagnosis, repeated ineffective treatments, and prolonged symptom duration, all of which contribute to psychological distress and impaired quality of life
.
In recent years, increasing attention has been directed toward sensory profiling as a tool to refine the clinical evaluation of vulvar pain syndromes. Prior studies suggest that verbal pain descriptors may reflect distinct underlying neurophysiological mechanisms rather than representing nonspecific subjective complaints
| [7] | Bohm-Starke N, Hilliges M, Falconer C, Rylander E. Neurochemical characterization of the vestibular nerves in women with vulvar vestibulitis syndrome. Gynecol Obstet Invest. 2001; 52(4): 243–248. https://doi.org/10.1159/000010198 |
| [8] | Farmer MA, Maykut CA, Baggish MS, Binik YM, Khalife S. Pain ratings and pain language in vulvodynia. Pain Res Manag. 2010; 15(1): 1–6. https://doi.org/10.1155/2010/847613 |
[7, 8]
. In our previous work, we introduced a structured approach to symptom classification in CVD by identifying recurring sensory patterns such as burning, stinging, and tenderness, which tended to cluster in patients diagnosed with either vulvodynia or vulvar dermatoses
| [9] | Harni V, Babic D, Hadzavdic S, Barisic D, Karadza M. Burning, stinging, tenderness: sensory profiling of vulvar pain in chronic discomfort—A DATRIV study perspective. J Gynecol Obstet. 2024; 12(6): 118–131.
https://doi.org/10.11648/j.jgo.20241206.11 |
[9]
. Building on this framework, we further differentiated pain phenotypes consistent with A-delta– and C-fiber–mediated nociceptive processing, associating predominantly sharp pain sensations with A-delta fiber hyperexcitability and dull pain sensations with C-fiber–mediated input.
Despite these advances in clinical phenotyping, the relationship between subjective pain quality and objective histopathological alterations remains largely unexplored in gynecologic literature. A persistent clinical question concerns whether vulvodynia and vulvar dermatoses represent biologically distinct entities or mechanistically overlapping phenotypes along a shared neuroimmune spectrum. Conceptual and clinical overlap between these conditions has been acknowledged, particularly with respect to symptom presentation and diagnostic uncertainty
. Sensory profiling data from the DATRIV study further suggested partial convergence between vulvodynia and vulvar dermatoses, with descriptors such as burning and stinging occurring across both diagnostic groups despite differences in clinical classification
| [9] | Harni V, Babic D, Hadzavdic S, Barisic D, Karadza M. Burning, stinging, tenderness: sensory profiling of vulvar pain in chronic discomfort—A DATRIV study perspective. J Gynecol Obstet. 2024; 12(6): 118–131.
https://doi.org/10.11648/j.jgo.20241206.11 |
[9]
.
In other chronic pain disorders, including peripheral neuropathies and fibromyalgia, pain quality has been shown to correlate with measurable tissue-level alterations such as changes in small nerve fiber density, immune cell infiltration, and connective tissue remodeling
. These observations support the concept that qualitative aspects of pain perception may provide insight into underlying biological mechanisms. Whether similar correlations exist in chronic vulvar pain conditions has not yet been systematically investigated.
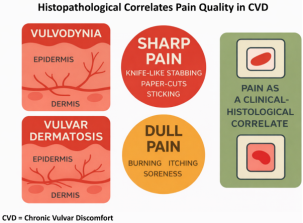
Figure 1. Study Framework and Clinical Translation: Histopathology and Pain Quality in Chronic Vulvar Discomfort (DATRIV Study).
This figure integrates the diagnostic framework, key findings, and clinical implications of the DATRIV study. Vulvodynia and vulvar dermatoses are presented as distinct clinicopathological entities, characterized by different pain qualities. Sharp pain (knife-like, stabbing, paper-cut) and dull pain (burning, itching, soreness) are shown as clinically relevant correlates of underlying histopathological patterns, highlighting pain quality as a potential tool for tissue-specific inference.
The present study addresses this gap by analyzing vulvar biopsy specimens from patients enrolled in the DATRIV study and systematically correlating categorized pain profiles with blinded epidermal and dermal histopathological findings. The primary objective was to determine whether distinct pain qualities – specifically sharp versus dull sensory phenotypes – are consistently associated with specific microscopic tissue patterns in vulvodynia and vulvar dermatoses. By linking structured verbal pain descriptors to objective morphological alterations, this study evaluates whether pain quality functions as a biologically grounded diagnostic signal rather than a purely subjective symptom, thereby contributing to mechanism-oriented differentiation within chronic vulvar discomfort.
2. Methods
2.1. Study Design and Setting
This study represents a predefined sub-analysis of the DATRIV study (Diagnostic Accuracy of Three Rings Vulvoscopy), a prospective, observational investigation conducted at Polyclinic Harni, Zagreb, Croatia, between December 1, 2011, and December 31, 2016. The primary objective of the DATRIV study was to evaluate the diagnostic accuracy of chronic vulvar discomfort (CVD) using the Three Rings Vulvoscopy (TRIV) approach, a structured method designed to improve systematic visual assessment and localization of vulvar pathology
| [16] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the vulvoscopy index for detection of vulvar dermatoses (DATRIV Study, Part 1). J Gynecol Obstet. 2022; 10(1): 39–47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [17] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N–S–P scheme for detection of vulvar dermatoses (DATRIV Study, Part 2). J Gynecol Obstet. 2022; 10(3): 159–166.
https://doi.org/10.11648/j.jgo.20221003.11 |
| [18] | Harni V, Babic D, Hadzavdic S, Barisic D. Nonspecific lesions in patients with chronic vulvar discomfort revealed vulvodynia as chronic reflex pain syndrome (CRPS) type I. J Gynecol Obstet. 2022; 10(6): 243–252.
https://doi.org/10.11648/j.jgo.20221006.12 |
[16-18]
.
In addition to its primary diagnostic focus, the DATRIV study incorporated a secondary exploratory objective aimed at symptom-based phenotyping to better characterize sensory patterns reported by affected women. The present sub-analysis focuses specifically on correlating patient-reported pain quality descriptors—categorized as sharp or dull—with corresponding histopathological findings in women diagnosed with vulvodynia and vulvar dermatoses.
2.2. Patient Selection
A total of 328 women aged 18 to 75 years were enrolled in the DATRIV study. Eligibility criteria included the presence of chronic vulvar symptoms persisting for longer than three months, in accordance with established definitions of persistent vulvar pain
| [1] | Bornstein J, Goldstein AT, Stockdale CK, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20(2): 126–130.
https://doi.org/10.1097/LGT.0000000000000194 |
[1]
. Exclusion criteria comprised active vulvovaginal infection, gynecologic or dermatologic malignancy, incomplete clinical documentation, or deviation from the predefined study protocol.
All enrolled participants underwent a standardized gynecologic examination, comprehensive TRIV vulvoscopy, and structured symptom assessment. Based on clinical history, vulvoscopic findings, and responses to standardized vulvar pain questionnaires aligned with ISSVD terminology
| [1] | Bornstein J, Goldstein AT, Stockdale CK, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20(2): 126–130.
https://doi.org/10.1097/LGT.0000000000000194 |
[1]
, participants were stratified into four diagnostic groups. Asymptomatic participants were subclassified into women with entirely normal vulvar appearance and women with nonspecific vulvar changes in the absence of symptoms. Symptomatic participants were categorized as having either primary vulvar pain (vulvodynia) or secondary pain attributable to histologically confirmed vulvar dermatoses.
The diagnosis of vulvodynia was established in accordance with the ISSVD consensus criteria defining persistent vulvar pain of at least three months’ duration without an identifiable cause
| [1] | Bornstein J, Goldstein AT, Stockdale CK, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20(2): 126–130.
https://doi.org/10.1097/LGT.0000000000000194 |
[1]
. Vulvar dermatoses—including lichen sclerosis, lichen planus, and nonspecific inflammatory vulvar dermatoses—were diagnosed based on clinicopathological correlation and confirmed by biopsy when clinically indicated.
2.3. Symptom Classification
Pain quality was classified as sharp or dull based on patient-reported language obtained through structured clinical interviews and standardized symptom documentation forms. Pain descriptors were derived from established pain-language frameworks and clinician-guided interviews conducted at the time of evaluation
| [7] | Bohm-Starke N, Hilliges M, Falconer C, Rylander E. Neurochemical characterization of the vestibular nerves in women with vulvar vestibulitis syndrome. Gynecol Obstet Invest. 2001; 52(4): 243–248. https://doi.org/10.1159/000010198 |
| [8] | Farmer MA, Maykut CA, Baggish MS, Binik YM, Khalife S. Pain ratings and pain language in vulvodynia. Pain Res Manag. 2010; 15(1): 1–6. https://doi.org/10.1155/2010/847613 |
[7, 8]
. Sharp pain descriptors included stabbing, knife-like, paper-cut, and pricking sensations, whereas dull pain descriptors encompassed aching, soreness, itching, irritation, and persistent burning.
All pain qualities were recorded independently, regardless of their assignment to sharp or dull categories. Each descriptor was initially analyzed separately, after which results were integrated into sharp and dull pain groups. When patients reported both pain qualities, classification was determined according to the dominant symptom affecting daily functioning or the area of greatest sensitivity during clinical provocation testing, including the cotton-swab test. If no dominant quality could be identified, dual coding was applied.
To ensure methodological consistency in symptom categorization, all structured clinical interviews and pain classifications were conducted by the same experienced clinician (V.H.) using predefined descriptor categories. Interviews followed a standardized clinical format with predefined pain-language descriptors, allowing systematic documentation of sensory qualities. This approach minimized interobserver variability and ensured uniform interpretation of patient-reported pain characteristics across all study participants.
2.4. Biopsy and Histopathology
Vulvar biopsies were performed under local anesthesia according to a standardized protocol. Vulvar biopsies were performed under local anesthesia according to a standardized protocol. In asymptomatic participants undergoing elective labiaplasty procedures, reference tissue samples were obtained using a 5 mm punch biopsy from the inner aspect of the labia minora. This anatomical location was selected to ensure comparability with biopsy sites obtained from symptomatic participants, particularly those involving the vestibular and inner vulvar regions. These specimens provided histologically normal reference tissue while maintaining anatomical consistency across study groups.
All clinical examinations, structured interviews, vulvoscopic assessments, biopsies, and aesthetic surgical procedures were performed by the same physician (V.H.). This approach ensured procedural consistency in patient evaluation, biopsy site selection, and tissue sampling, thereby reducing potential variability related to operator-dependent factors.
Biopsy sites in symptomatic participants were selected according to lesion localization identified during vulvoscopy and classified as specific or nonspecific. In asymptomatic women undergoing elective labiaplasty for non-medical indications, tissue specimens obtained during the procedure were used as reference samples for histological comparison
.
In all cases, 5 mm punch biopsies were obtained, fixed in formalin, and processed as formalin-fixed, paraffin-embedded (FFPE) tissue blocks. Sections measuring 4–5 μm were mounted on glass slides and routinely stained with hematoxylin and eosin (H&E) for primary histopathological assessment. Additional special stains, including periodic acid–Schiff and Masson’s trichrome, as well as immunohistochemical markers (S-100 and PGP 9.5 for nerve fibers), were applied when clinically indicated.
All histopathological specimens were reviewed by an experienced dermatopathologist (D.B.) who was blinded to clinical symptom profiles. A standardized evaluation protocol with predefined criteria was applied to ensure consistent histopathological assessment based on established dermatopathological criteria
| [20] | Weedon D. Weedon’s skin pathology. 5th ed. Elsevier; 2020. |
| [21] | Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X. Lever’s histopathology of the skin. 11th ed. Wolters Kluwer; 2014. |
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
| [23] | Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020. |
[20-23]
.
Normal epidermis was defined as stratified squamous epithelium with preserved layering (stratum basale, spinosum, granulosum, and corneum), intact rete ridge architecture, and thickness within the expected range for vulvar skin (approximately 80–120 μm)
| [19] | Vural E, Kecici AS, Sevim DG, et al. Human epidermal thickness at different body sites: a histometric study. Int J Morphol. 2022; 40(1): 67–74.
https://doi.org/10.4067/S0717-95022022000100067 |
| [20] | Weedon D. Weedon’s skin pathology. 5th ed. Elsevier; 2020. |
| [21] | Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X. Lever’s histopathology of the skin. 11th ed. Wolters Kluwer; 2014. |
[19-21]
. Epidermal atrophy was defined as epithelial thinning below 70 μm, frequently accompanied by flattening of rete ridges and reduction in keratinocyte layers
| [20] | Weedon D. Weedon’s skin pathology. 5th ed. Elsevier; 2020. |
| [21] | Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X. Lever’s histopathology of the skin. 11th ed. Wolters Kluwer; 2014. |
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
[20-22]
. Hyperkeratosis was defined as thickening of the stratum corneum without nuclear retention, whereas parakeratosis was defined by retention of nuclei within the stratum corneum, reflecting incomplete keratinocyte maturation and accelerated epidermal turnover
| [21] | Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X. Lever’s histopathology of the skin. 11th ed. Wolters Kluwer; 2014. |
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
| [23] | Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020. |
[21-23]
.
Basement membrane integrity was assessed as intact or disrupted based on the continuity and thickness of the basal lamina. Dermal fibrosis and collagen sclerosis were defined as excessive collagen deposition with hyalinization of the papillary dermis and were graded semiquantitatively as mild, moderate, or severe
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
| [23] | Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020. |
[22, 23]
. Perivascular and perineural inflammatory infiltrates were graded according to lymphocyte density (absent, mild, moderate, dense), with distribution patterns recorded
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
[22]
. Vascular changes were categorized as congestion or proliferation based on vessel caliber and density
| [23] | Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020. |
[23]
. Additional microscopic features, including lymphocytic exocytosis, apoptotic keratinocytes, and spongiosis, were documented when present
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
| [23] | Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020. |
[22, 23]
.
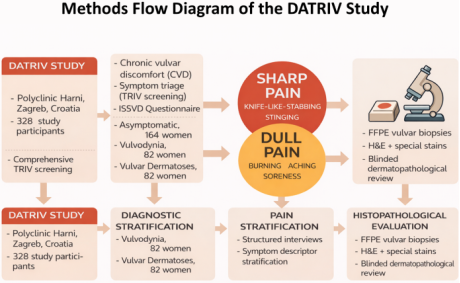
Figure 2. Methods Flow Diagram. FFPE – Formalin Fixed Paraffin-Embedded; H&E-Hematoxylin and Eosin.
Overview of the DATRIV study workflow. A total of 328 women were stratified into asymptomatic (n = 164) and symptomatic groups, including vulvodynia (n = 82) and vulvar dermatoses (n = 82), based on TRIV screening and symptom assessment. Symptomatic patients were further classified by pain quality (sharp vs. dull).
2.5. Statistical Analysis
Descriptive statistics were used to summarize patient demographics, symptom profiles, and histopathological characteristics. Categorical variables were analyzed using chi-square or Fisher’s exact tests, while continuous variables were evaluated using Student’s t-test or the Mann–Whitney U test, depending on data distribution.
Correlation analyses were performed to assess associations between pain quality (sharp vs. dull) and specific histopathological features. Multivariate logistic regression models were constructed to adjust for potential confounding variables, including age, symptom duration, biopsy site, and diagnostic category (vulvodynia vs. vulvar dermatoses).
Subgroup analyses were conducted based on anatomical biopsy location (outer, middle, and inner vulvar ring). Hierarchical cluster analysis was employed to identify patterns of histopathological features associated with specific pain qualities. A two-sided p-value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 25.0 and R version 4.0.2.
In cases where patients reported both sharp and dull pain qualities without a clearly dominant descriptor, dual coding was initially recorded in the descriptive dataset. For multivariate regression analyses, cases were assigned to the dominant pain category based on the symptom reported as most functionally limiting during daily activities or during clinical provocation testing. Secondary descriptors were retained for descriptive and exploratory analyses to preserve the multidimensional nature of pain reporting.
2.6. Ethical Considerations
All participants were informed of the voluntary nature of study participation and were given the option to decline involvement in structured symptom interviews without consequence. Written informed consent was obtained from all patients undergoing vulvoscopy and vulvar biopsy following detailed explanation of study procedures, potential risks, benefits, and the right to withdraw at any time.
The study protocol was approved by the Institutional Review Board of Polyclinic Harni (Ethical Approval No. 20111201001) and conducted in accordance with the principles of the Declaration of Helsinki.
3. Results
3.1. Study Population
The study included 328 women enrolled in the DATRIV study, stratified into four predefined groups: women with normal vulvar findings, women with asymptomatic nonspecific vulvar changes, women diagnosed with vulvodynia, and women with histologically confirmed vulvar dermatoses. The distribution of age, symptom duration, and biopsy location was comparable across diagnostic groups, allowing meaningful comparison of histopathological features and pain profiles.
3.2. Distribution of Pain Quality Descriptors
Pain qualities demonstrated a statistically robust and clinically meaningful stratification across the four predefined groups (normal vulva, impaired asymptomatic skin, vulvodynia, vulvar dermatoses). Dull descriptors—including burning, itching, aching, and soreness—predominated in vulvar dermatoses (p < 0.001), forming a coherent sensory pattern within this diagnostic category.
In contrast, sharp pain descriptors—such as stabbing, knife-like, and paper-cut sensations—were significantly overrepresented in the vulvodynia group compared with all other groups (p < 0.001).
The normal vulva and impaired asymptomatic skin groups showed minimal endorsement of persistent pain descriptors, supporting the internal construct validity of the classification framework. A subset of patients in both diagnostic groups reported mixed pain qualities; in these cases, classification was based on the dominant symptom affecting daily functioning.
3.3. Epidermal Histopathology and Pain Quality
Vulvar dermatoses exhibited a significantly higher prevalence of measurable epidermal abnormalities compared with all other groups (
Table 1). These alterations included hyperkeratosis, acanthosis, basal layer irregularity, and focal atrophy. Pairwise comparisons confirmed that these structural changes were specific to the dermatoses group and did not meaningfully overlap with vulvodynia. The epidermal compartment in vulvar dermatoses therefore demonstrated consistent architectural disruption rather than incidental or borderline variation.
In contrast, epidermal architecture was preserved in the majority of women with vulvodynia, closely resembling the histological pattern observed in normal vulva and impaired asymptomatic skin. In these groups, the epidermis typically demonstrated intact stratification and thickness within the expected range for vulvar skin. Subtle epidermal alterations—including focal thinning, irregular rete ridge patterns, and keratinization abnormalities—were more frequently observed in patients reporting sharp pain descriptors; however, the overall prevalence of epidermal thinning, hyperplasia, or keratinization disorders in vulvodynia did not significantly exceed baseline levels.
When stratified by dominant pain quality rather than diagnosis alone, dull or burning phenotypes showed a strong association with epidermal thickening and basal layer changes, whereas sharp or stinging phenotypes clustered within morphologically preserved epidermis. This sensory–structural concordance remained statistically significant after adjustment for age and symptom duration.
Table 1. Histopathological Characteristics of the Vulvar Epidermis Across Study Subgroups.
Histopathological Features | Normal vulva N=82 | Impaired vulvar skin N=82 | Vulvodynia N=82 | Vulvar dermatoses N=82 | p-value |
Normal epidermis | 76 (92.7%) | 72 (87.8%) | 73 (89.0%) | 6 (7.3%)** | p < 0.001 |
Epidermal thinning | 0 (0%) | 0 (0%) | 0 (0%) | 53 (64.6%)** | p < 0.001 |
Hyperkeratosis | 0 (0%) | 6 (7.3%) | 3 (3.7%) | 62 (75.6%)** | p < 0.001 |
Parakeratosis | 3 (3.7%) | 5 (6.1%) | 7 (8.5%) | 30 (36.6%)** | p < 0.001 |
Acanthosis | 3 (3.7%) | 1 (1.2%) | 1 (1.2%) | 16 (19.5%)** | p < 0.001 |
Epidermal atrophy | 0 (0%) | 0 (0%) | 0 (0%) | 25 (30.5%)** | p < 0.001 |
3.4. Dermal Histopathology and Pain Quality
Dermal analysis revealed the most pronounced divergence between sensory phenotypes (
Table 2 and 3;
Figure 3).
Vulvar dermatoses, predominantly associated with dull pain descriptors, demonstrated a significantly increased prevalence of chronic inflammatory infiltrates, collagen remodeling, hyalinization, and perivascular inflammatory infiltrates, independent of symptom duration (p < 0.001). Although inflammatory infiltrates were observed in both symptomatic groups, only vulvar dermatoses demonstrated concurrent collagen remodeling and hyalinization, indicating structural reorganization rather than reactive inflammatory activity alone. The dermal compartment in this group therefore reflected sustained structural remodeling rather than transient inflammatory activity.
In contrast, sharp or fast pain phenotypes—most commonly observed in vulvodynia—frequently exhibited increased vascularity, prominent adnexal structures, and increased nerve fiber density, while remaining largely associated with dermal preservation or only subtle, nonspecific changes. Mast cells were observed predominantly in vulvodynia and were not detected in vulvar dermatoses. These dermal features were observed across a range of symptom durations, with nerve fiber enrichment evident even in earlier stages.
Table 2. Histopathological Characteristics of the Vulvar Dermis Across Clinical Subgroups.
Histopathological Characteristics | Normal vulva N=82 | Impaired vulvar skin N=82 | Vulvodynia N=82 | Vulvar Dermatoses N=82 | p-value |
Inflammatory cells | 42 (51.2%) | 52 (63.4%) | 65 (79.3%)** | 73 (89.0%)** | p < 0.001 |
Mononuclear inflammatory cells | 33 (40.2%) | 46 (56.1%) | 61 (74.4%)** | 63 (76.8%)** | p < 0.001 |
Lymphocytes | 9 (11.0%) | 3 (3.7%) | 3 (3.7%) | 13 (15.9%)* | p = 0.011 |
Mast cells | 2 (2.4%) | 0 (0%) | 6 (7.3%)* | 0 (0%) | p = 0.006 |
Collagen fibres | 7 (8.5%) | 1 (1.2%) | 9 (11.0%) | 44 (53.7%)** | p < 0.001 |
Hyalinization | 2 (2.4%) | 0 (0%) | 0 (0%) | 25 (30.5%)** | p < 0.001 |
Hyperpigmentation | 7 (8.5%)* | 2 (2.4%) | 5 (6.1%)* | 0 (0%) | p = 0.034 |
Elongated dermal papillae | 5 (6.1%)* | 7 (8.5%)* | 0 (0%) | 1 (1.2%) | p = 0.015 |
Blood vessels | 31 (37.8%) | 30 (36.6%) | 53 (64.6%)** | 5 (6.1%) | p < 0.001 |
Sebaceous glands | 39 (47.6%) | 48 (58.5%) | 61 (74.4%)** | 1 (1.2%) | p < 0.001 |
Nerve fibres | 28 (34.1%) | 27 (32.9%) | 68 (82.9%)** | 0 (0%) | P < 0.001 |
Table 3. Post-hoc Pairwise Proportion Tests for Dermal Features Across Subgroups (Vulvodynia vs. Other Groups).
Feature | vs. Normal vulva N=82 | vs. Impaired vulvar skin N=82 | vs. Vulvar dermatoses N=82 |
Inflammatory cells | p < 0.001** | p = 0.025* | n.s. |
Mononuclear inflammatory cells | p < 0.001** | p = 0.017* | n.s. |
Lymphocytes | n.s. | n.s. | p = 0.011* |
Mast cells | n.s. | p = 0.016* | p = 0.016* |
Collagen fibres | n.s. | p = 0.008* | p < 0.001** |
Hyalinization | n.s. | - | p < 0.001** |
Hyperpigmentation | n.s. | n.s. | p = 0.026* |
Elongated dermal papillae | p = 0.026* | p = 0.001** | - |
Blood vessels | p < 0.001** | p < 0.001** | p < 0.001** |
Sebaceous glands | p = 0.001** | p = 0.032* | p < 0.001** |
Nerve fibres | p < 0.001** | p < 0.001** | p < 0.001** |
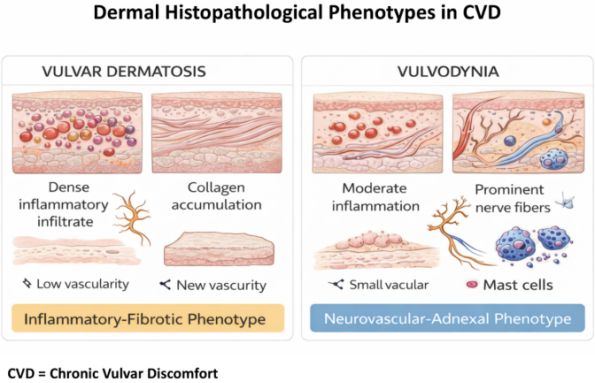
Figure 3. Distinct Dermal Histopathological Phenotypes in Vulvar Dermatoses and Vulvodynia.
Schematic comparison of dominant dermal features. Vulvar dermatoses demonstrate an inflammatory–fibrotic phenotype characterized by collagen accumulation and hyalinization, whereas vulvodynia is defined by a neurovascular–adnexal phenotype with increased vascularity, nerve fibers, sebaceous glands, and mast cell density.
3.5. Symptom-epidermis Association
Associations between pain quality and epidermal histopathology differed substantially between diagnostic groups. Sharp pain descriptors exhibited distinct diagnostic and histopathological patterns.
3.5.1. Vulvar Dermatoses
In women with vulvar dermatoses, sharp pain descriptors were overall infrequent and showed minimal association with epidermal abnormalities (
Table 4). Even in the presence of pronounced epidermal pathology, sharp pain was rarely reported, indicating that inflammatory or degenerative epidermal changes alone are insufficient to generate fast pain sensations in this group. Among sharp pain qualities, only knife-like pain demonstrated a weak association with altered epidermal architecture, suggesting a limited contribution of the epidermis to sharp pain perception in vulvar dermatoses.
Table 4. Association Between Epidermal Histopathology and Sharp Pain Descriptors in Patients with Vulvar Dermatoses (N=82).
Sharp Pain Descriptor | Vulvar Dermatoses N=82 | Normal Epidermis N=29 | Abnormal Epidermis N=53 | p-value |
Sharp pain | 12/82 (14.6%) | 3/29 (10.3%) | 9/53 (16.9%) | n.s. |
Knife-Like | 5/82 (6.1%) | 0/29 (0%) | 5/53 (9.4%)* | p = 0.033 |
Paper-Cut | 3/82 (3.6%) | 1/29 (3.5%) | 2/53 (3.8%) | n.s. |
Stabbing | 6/82 (7.4%) | 2/29 (6.9%) | 4/53 (7.6%) | n.s. |
Sticking | 9/82 (10.9%) | 3/29 (10.3%) | 6/53 (11.3%) | n.s. |
3.5.2. Vulvodynia
In contrast, in women with vulvodynia, sharp pain descriptors were strongly associated with abnormal epidermal findings. Knife-like, paper-cut, and stabbing pain qualities were significantly more prevalent in the presence of epidermal abnormalities (
Table 5), indicating a close relationship between superficial epithelial alterations and sharp pain perception. These findings suggest that, in vulvodynia, the epidermis may function as a critical interface for nociceptive signaling related to fast, well-localized pain. Overall, these results underscore a diagnosis-specific role of the epidermis in sharp pain perception, with a pronounced contribution in vulvodynia and a marginal role in vulvar dermatoses (
Figure 4).
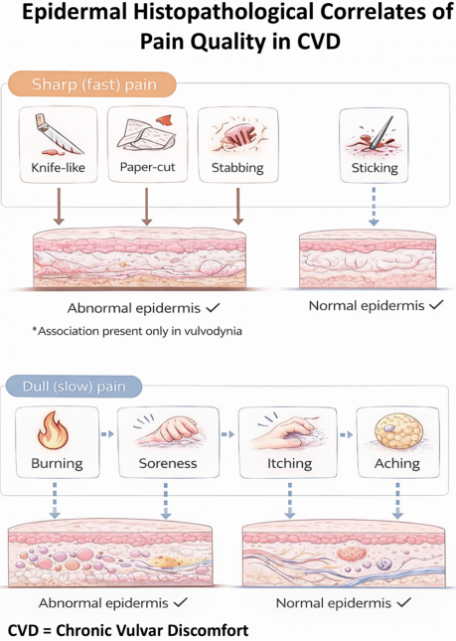
Figure 4. Associations Between Pain Quality and Epidermal Histopathology.
Table 5. Association Between Epidermal Histopathology and Sharp Pain Descriptors in Patients with Vulvodynia (N=82).
Sharp Pain Descriptor | Vulvodynia N=82 | Normal Epidermis N=71 | Abnormal Epidermis N=11 | p-value |
Sharp pain | 31/82 (37.8%) | 22/71 (31.0%) | 9/11 (81.8%)** | p = 0.001 |
Knife-Like | 13/82 (15.9%) | 7/71 (9.9%) | 6/11 (54.6%)** | p = 0.001 |
Paper-Cut | 10/82 (12.2%) | 6/71 (8.4%) | 4/11 (36.4%)* | p = 0.021 |
Stabbing | 17/82 (20.7%) | 12/71 (16.9%) | 5/11 (45.5%)* | p = 0.044 |
Sticking | 18/82 (22.0%) | 15/71 (21.1%) | 3/11 (27.3%) | n.s. |
Conceptual diagram illustrating the relationship between epidermal status and pain quality. Sharp (fast) pain descriptors are strongly associated with epidermal abnormalities in vulvodynia but not in vulvar dermatoses, whereas dull (slow) pain descriptors are independent of epidermal histopathology in both diagnostic groups.
3.6. Dull Pain Descriptors
Dull pain descriptors, including burning, aching, soreness, and tenderness, did not differ according to epidermal status in either diagnostic group. The absence of association between dull pain descriptors and epidermal abnormalities suggests that the epidermis is not the primary histological substrate underlying slow, diffuse pain perception (
Tables 6 and 7;
Figure 4).
Table 6. Association Between Epidermal Histopathology and Dull Pain Descriptors in Patients with Vulvar Dermatoses (N=82).
Dull Pain Descriptors | Vulvar Dermatoses N=82 | Normal Epidermis N=29 | Abnormal Epidermis N=53 | p-value |
Dull pain | 82/82 (100.0%) | 29/29 (100.0%) | 53/53 (100.0%) | n.s. |
Burning | 22/82 (26.8%) | 6/29 (20.7%) | 16/53 (30.2%) | n.s. |
Stinging | 65/82 (79.3%) | 24/29 (82.8%) | 41/53 (77.4%) | n.s. |
Soreness | 37/82 (45.1%) | 13/29 (44.8%) | 24/53 (45.3%) | n.s. |
Irritation | 35/82 (42.7%) | 12/29 (41.4%) | 23/53 (43.4%) | n.s. |
Itching | 79/82 (96.3%) | 28/29 (96.6%) | 51/53 (96.2%) | n.s. |
Inflammation | 38/82 (46.3%) | 13/29 (44.8%) | 25/53 (47.2%) | n.s. |
Aching | 21/82 (25.6%) | 8/29 (27.6%) | 13/53 (24.5%) | n.s. |
Table 7. Association Between Epidermal Histopathology and Dull Pain Descriptors in Patients with Vulvodynia (N=82).
Dull Pain Descriptors | Vulvodynia N=82 | Normal Epidermis N=71 | Abnormal Epidermis N=11 | p-value |
Dull pain | 81/82 (98.8%) | 70/71 (98.6%) | 11/11 (100.0%) | n.s. |
Burning | 37/82 (45.1%) | 30/71 (42.3%) | 7/11 (63.6%) | n.s. |
Stinging | 66/82 (80.5%) | 57/71 (80.3%) | 9/11 (81.8%) | n.s. |
Soreness | 54/82 (65.9%) | 48/71 (67.6%) | 6/11 (54.4%) | n.s. |
Irritation | 48/82 (58.5%) | 39/71 (54.9%) | 9/11 (81.8%) | n.s. |
Itching | 63/82 (76.8%) | 54/71 (76.1%) | 9/11 (81.8%) | n.s. |
Inflammation | 49/82 (59.8%) | 41/71 (57.8%) | 8/11 (72.7%) | n.s. |
Aching | 45/82 (54.9%) | 38/71 (53.5%) | 7/11 (63.6%) | n.s. |
3.7. Temporal Association
3.7.1. Vulvar Dermatoses
Table 8. Histopathological Features of the Vulvar Dermis According to Symptom Duration in Patients with Vulvar Dermatoses (N = 82).
Dermal Histopathological Characteristics in Vulvar Dermatoses | Duration of Symptoms | p-value |
<24 months N=24 | >24 months N=58 |
Inflammatory cells | 23 (95.8%) | 50 (86.2%) | n.s. |
Mononuclear inflammatory cells | 19 (79.2%) | 44 (75.9%) | n.s. |
Lymphocytes | 5 (20.8%) | 8 (13.8%) | n.s. |
Mast cells | 0 (0%) | 0 (0%) | - |
Collagen fibres | 11 (45.8%) | 33 (56.9%) | n.s. |
Hyalinization | 7 (29.2%) | 18 (31.0%) | n.s. |
Hyperpigmentation | 0 (0%) | 0 (0%) | - |
Elongated dermal papillae | 0 (0%) | 1 (1.7%) | - |
Blood vessels | 1 (4.2%) | 4 (6.9%) | - |
Sebaceous glands | 0 (0%) | 1 (1.7%) | - |
Nerve fibres | 0 (0%) | 0 (0%) | - |
Analysis of symptom duration indicated that the inflammatory–fibrotic signature of vulvar dermatoses stabilizes early after symptom onset. Inflammation, collagen deposition, and hyalinization were common and similar across duration groups, while mast cells, hyperpigmentation, and nerve fibers were absent in both (
Table 8).
3.7.2. Vulvodynia
Table 9. Histopathological Features of the Vulvar Dermis According to Symptom Duration in Patients with Vulvodynia (N=82).
Dermal Histopathological Characteristics in Vulvodynia | Duration of Symptoms | p-value |
<24 months N=29 | >24 months N=53 |
Inflammatory cells | 18 (62.1%) | 47 (88.7%)* | p = 0.005 |
Mononuclear inflammatory cells | 16 (55.2%) | 45 (84.9%)* | p = 0.003 |
Lymphocytes | 1 (3.4%) | 2 (3.8%) | - |
Mast cells | 4 (13.8%) | 2 (3.8%) | - |
Collagen fibres | 1 (3.4%) | 8 (15.1%) | n.s. |
Hyalinization | 0 (0%) | 0 (0%) | - |
Hyperpigmentation | 1 (4.2%) | 4 (6.9%) | - |
Elongated dermal papillae | 0 (0%) | 0 (0%) | - |
Blood vessels | 14 (48.3%) | 39 (73.6%)* | p = 0.022 |
Sebaceous glands | 22 (75.9%) | 39 (73.6%) | n.s. |
Nerve fibres | 21 (72.4%) | 47 (88.7%) | p = 0.061 |
In vulvodynia, longer symptom duration was associated with increased dermal inflammation and vascular changes, whereas nerve fiber enrichment was already evident in patients with shorter symptom duration, suggesting early neurocutaneous involvement followed by progressive inflammatory amplification. (
Table 9;
Figure 5).
Figure 5. Temporal Dermal Changes in Chronic Vulvar Discomfort.
Timeline-based schematic illustrating the effect of symptom duration on dermal features. In vulvar dermatoses, inflammatory–fibrotic changes emerge early and remain relatively stable over time. In vulvodynia, longer symptom duration is associated with progressive increases in inflammation and vascularity, superimposed on an early-established neurocutaneous phenotype.
3.8. Multivariate and Subgroup Analyses
Multivariate logistic regression analysis demonstrated that sharp pain quality was independently associated with epidermal abnormalities and neurovascular dermal features, after adjustment for age, symptom duration, biopsy site, and diagnostic category. Dull pain quality was independently associated with dermal fibrosis, inflammatory infiltrates, and collagen sclerosis.
Subgroup analyses based on anatomical biopsy location revealed consistent associations between pain quality and histopathological features across the inner vestibule, outer vestibule, labia minora, and labia majora. Hierarchical cluster analysis further supported the separation of sharp and dull pain phenotypes based on distinct combinations of epidermal and dermal features.
4. Discussion
At the tissue level, the present results demonstrate that pain quality is not an epiphenomenon but a clinically meaningful expression of underlying peripheral biology. The clear statistical separation between sharp and dull descriptors across diagnostic groups indicates that chronic vulvar discomfort (CVD) does not represent a homogeneous sensory continuum. Rather, it comprises distinct phenotypic clusters in which subjective pain language mirrors divergent histopathological substrates.
Sharp, stabbing, knife-like, and cutting sensations—predominantly reported in vulvodynia—were consistently associated with preserved epidermal architecture and the absence of substantial inflammatory or fibrotic dermal remodeling. This structural–sensory dissociation strengthens the interpretation of vulvodynia as a predominantly neuropathic or dysfunction-driven pain phenotype rather than a primary inflammatory dermatosis
| [8] | Farmer MA, Maykut CA, Baggish MS, Binik YM, Khalife S. Pain ratings and pain language in vulvodynia. Pain Res Manag. 2010; 15(1): 1–6. https://doi.org/10.1155/2010/847613 |
| [9] | Harni V, Babic D, Hadzavdic S, Barisic D, Karadza M. Burning, stinging, tenderness: sensory profiling of vulvar pain in chronic discomfort—A DATRIV study perspective. J Gynecol Obstet. 2024; 12(6): 118–131.
https://doi.org/10.11648/j.jgo.20241206.11 |
| [11] | Edwards L. Vulvodynia. Clin Obstet Gynecol. 2015 Mar; 58(1): 143-52. https://doi.org/10.1097/GRF.0000000000000093 |
| [24] | Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011; 152 (Suppl 3): S2–S15.
https://doi.org/10.1016/j.pain.2010.09.030 |
| [25] | Treede RD, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain. Pain. 2019; 160(1): 19–27. https://doi.org/10.1097/j.pain.0000000000001384 |
| [26] | Baron R, Maier C, Attal N, et al. Peripheral neuropathic pain: a mechanism-related organizing principle. Pain. 2017; 158(2): 261–272. https://doi.org/10.1097/j.pain.0000000000000790 |
| [27] | Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology. 2008; 70(18): 1630–1635.
https://doi.org/10.1212/01.wnl.0000282763.29778.59 |
[8, 9, 11, 24-27]
. Importantly, the preservation of epidermal thickness and the lack of significant basal or dermal alterations argue against tissue destruction as the principal driver of nociception in this group. Instead, the results support a model in which altered peripheral excitability, enhanced signal gain, and central amplification generate disproportionate sensory experience in the context of morphologically subtle tissue.
Conversely, dull, burning, itching, and soreness qualities—more frequently observed in vulvar dermatoses—demonstrated robust statistical associations with measurable structural abnormalities. Epidermal thickening, basal layer disruption, dermal inflammatory infiltrates, collagen deposition, and vascular remodeling formed a stable morphological constellation corresponding to slow, diffuse pain descriptors
| [9] | Harni V, Babic D, Hadzavdic S, Barisic D, Karadza M. Burning, stinging, tenderness: sensory profiling of vulvar pain in chronic discomfort—A DATRIV study perspective. J Gynecol Obstet. 2024; 12(6): 118–131.
https://doi.org/10.11648/j.jgo.20241206.11 |
| [19] | Vural E, Kecici AS, Sevim DG, et al. Human epidermal thickness at different body sites: a histometric study. Int J Morphol. 2022; 40(1): 67–74.
https://doi.org/10.4067/S0717-95022022000100067 |
| [20] | Weedon D. Weedon’s skin pathology. 5th ed. Elsevier; 2020. |
| [21] | Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X. Lever’s histopathology of the skin. 11th ed. Wolters Kluwer; 2014. |
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
| [23] | Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020. |
[9, 19-23]
. These findings reinforce the interpretation of inflammatory vulvar dermatoses as tissue-driven nociceptive phenotypes in which structural remodeling and chronic immune activation provide continuous peripheral input. The convergence between morphological remodeling and slow pain qualities supports a C-fiber–dominant mechanism characterized by sustained, metabolically mediated nociception.
Mechanistically, the dichotomy observed in the Results section aligns with established neurobiological models of fast and slow pain processing. Sharp, stabbing, and cutting sensations correspond to A-delta–mediated signaling characterized by rapid conduction, spatial precision, and phasic activation
| [24] | Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011; 152 (Suppl 3): S2–S15.
https://doi.org/10.1016/j.pain.2010.09.030 |
| [25] | Treede RD, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain. Pain. 2019; 160(1): 19–27. https://doi.org/10.1097/j.pain.0000000000001384 |
| [26] | Baron R, Maier C, Attal N, et al. Peripheral neuropathic pain: a mechanism-related organizing principle. Pain. 2017; 158(2): 261–272. https://doi.org/10.1097/j.pain.0000000000000790 |
| [27] | Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology. 2008; 70(18): 1630–1635.
https://doi.org/10.1212/01.wnl.0000282763.29778.59 |
| [28] | Jensen TS, Finnerup NB. Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. Lancet Neurol. 2014; 13(9): 924–935.
https://doi.org/10.1016/S1474-4422(14)70102-4 |
| [29] | Tracey I, Mantyh PW. The cerebral signature for pain perception and its modulation. Neuron. 2007; 55(3): 377–391.
https://doi.org/10.1016/j.neuron.2007.07.012 |
| [30] | Basbaum AI, Bautista DM, Scherrer G, Julius D. Cellular and molecular mechanisms of pain. Cell. 2009; 139(2): 267–284. https://doi.org/10.1016/j.cell.2009.10.028 |
| [31] | McMahon SB, Koltzenburg M, Tracey I, Turk DC, editors. Wall & Melzack’s textbook of pain. 6th ed. Elsevier; 2013. |
| [32] | Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013; 154 (Suppl 1): S29–S43.
https://doi.org/10.1016/j.pain.2013.09.001 |
[24-32]
. The statistical predominance of such descriptors in vulvodynia suggests heightened excitability or sensitization of fast-conducting nociceptive pathways, potentially accompanied by central disinhibition or maladaptive cortical processing. In contrast, dull and burning pain qualities correspond to polymodal C-fiber activation, which is typically associated with sustained inflammatory signaling, tissue acidosis, cytokine release, and structural remodeling
| [20] | Weedon D. Weedon’s skin pathology. 5th ed. Elsevier; 2020. |
| [21] | Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X. Lever’s histopathology of the skin. 11th ed. Wolters Kluwer; 2014. |
| [22] | Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020. |
| [23] | Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020. |
| [30] | Basbaum AI, Bautista DM, Scherrer G, Julius D. Cellular and molecular mechanisms of pain. Cell. 2009; 139(2): 267–284. https://doi.org/10.1016/j.cell.2009.10.028 |
| [33] | Maier C, Baron R, Tölle TR, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): reference data for the trunk and head. Pain. 2011; 152(1): 262–274. https://doi.org/10.1016/j.pain.2010.10.002 |
[20-23, 30, 33]
. The dermal inflammatory–fibrotic phenotype observed in vulvar dermatoses provides a morphological substrate compatible with such sustained nociceptive drive.
Notably, the absence of overt structural damage in vulvodynia does not imply biological normality. Previous histopathological and molecular studies have demonstrated that vulvodynia may be associated with subtle neuroimmune alterations despite macroscopically preserved vulvar tissue. Increased intraepithelial nerve fiber density has been reported in vestibular mucosa of affected women, suggesting peripheral neural hyperinnervation as a potential substrate of hypersensitivity. In parallel, elevated mast cell density and increased levels of neurotrophic and inflammatory mediators, including nerve growth factor and pro-inflammatory cytokines, have been documented in vulvar vestibular tissue. These findings support the concept that neuroimmune interactions and local inflammatory signaling may contribute to peripheral sensitization and persistent pain perception in vulvodynia even in the absence of overt structural dermatosis
| [34] | Bohm-Starke N, Hilliges M, Falconer C, Rylander E. Increased intraepithelial innervation in women with vulvar vestibulitis syndrome. Gynecol Obstet Invest. 1998; 46(4): 256–260.
https://doi.org/10.1159/000010045 |
| [35] | Papoutsis D, Haefner HK, Crum CP, Opipari AW Jr, Reed BD. Vestibular mast cell density in vulvodynia: a case-controlled study. J Low Genit Tract Dis. 2016; 20(3): 275–279.
https://doi.org/10.1097/LGT.0000000000000206 |
| [36] | Reed BD, Plegue MA, Sen A, Haefner HK, Siddiqui J, Remick DG. Nerve growth factor and selected cytokines in women with and without vulvodynia. J Low Genit Tract Dis. 2018; 22(2): 139–146. https://doi.org/10.1097/LGT.0000000000000370 |
[34-36]
.
Increasing evidence supports the presence of subtle neuroimmune interactions, altered small-fiber function, and peripheral sensitization even in macroscopically intact vulvar tissue
| [2] | Leclair CM, Goetsch MF, Korcheva VB, Anderson R, Peters D, Morgan TK. Differences in primary compared with secondary vestibulodynia by immunohistochemistry. Obstet Gynecol. 2011; 117(6): 1307–1313.
https://doi.org/10.1097/AOG.0b013e31821f7db0 |
| [7] | Bohm-Starke N, Hilliges M, Falconer C, Rylander E. Neurochemical characterization of the vestibular nerves in women with vulvar vestibulitis syndrome. Gynecol Obstet Invest. 2001; 52(4): 243–248. https://doi.org/10.1159/000010198 |
| [37] | Hore Z, Denk F. Neuroimmune interactions in chronic pain - An interdisciplinary perspective. Brain Behav Immun. 2019 Jul; 79: 56-62. https://doi.org/10.1016/j.bbi.2019.04.033 |
| [38] | Osborne, N. R.; Davis, K. D. Sex and Gender Differences in Pain. Int. Rev. Neurobiol. 2022, 164, 277–307.
https://doi.org/10.1016/bs.irn.2022.05.009 |
[2, 7, 37, 38]
. Although intraepidermal nerve fiber density was not directly quantified in the present study, the interpretation of neuropathic involvement should therefore be considered inferential and based on indirect histopathological and sensory correlations rather than direct quantitative measurement. Nevertheless, the consistent association between sharp pain descriptors and preserved epidermal architecture observed in this cohort aligns with established models of small-fiber–mediated pain syndromes and peripheral sensitization
. Thus, the contrast between “sharp without structure” and “dull with remodeling” should be interpreted as a divergence of dominant mechanisms rather than a binary distinction between organic and functional pathology.
Within the DATRIV diagnostic framework, these findings provide an additional integrative layer. Earlier components of the DATRIV study validated structured three-rings vulvoscopy and the N–S–P scheme as reliable tools for morphological stratification and diagnostic accuracy
| [16] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the vulvoscopy index for detection of vulvar dermatoses (DATRIV Study, Part 1). J Gynecol Obstet. 2022; 10(1): 39–47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [17] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N–S–P scheme for detection of vulvar dermatoses (DATRIV Study, Part 2). J Gynecol Obstet. 2022; 10(3): 159–166.
https://doi.org/10.11648/j.jgo.20221003.11 |
| [18] | Harni V, Babic D, Hadzavdic S, Barisic D. Nonspecific lesions in patients with chronic vulvar discomfort revealed vulvodynia as chronic reflex pain syndrome (CRPS) type I. J Gynecol Obstet. 2022; 10(6): 243–252.
https://doi.org/10.11648/j.jgo.20221006.12 |
[16-18]
. The present analysis extends this architecture by demonstrating that sensory profiling refines and biologically contextualizes morphological categories. In practical terms, combining pain quality assessment with vulvoscopic mapping enhances diagnostic resolution: sharp-dominant phenotypes with N–S–S patterns and minimal histological alteration align with neuropathic mechanisms, whereas dull-dominant phenotypes with P-containing patterns correspond to inflammatory dermatoses. Sensory profiling therefore functions not merely as descriptive symptom documentation but as a mechanistically informative diagnostic dimension embedded within the DATRIV model
| [9] | Harni V, Babic D, Hadzavdic S, Barisic D, Karadza M. Burning, stinging, tenderness: sensory profiling of vulvar pain in chronic discomfort—A DATRIV study perspective. J Gynecol Obstet. 2024; 12(6): 118–131.
https://doi.org/10.11648/j.jgo.20241206.11 |
| [16] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the vulvoscopy index for detection of vulvar dermatoses (DATRIV Study, Part 1). J Gynecol Obstet. 2022; 10(1): 39–47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [17] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N–S–P scheme for detection of vulvar dermatoses (DATRIV Study, Part 2). J Gynecol Obstet. 2022; 10(3): 159–166.
https://doi.org/10.11648/j.jgo.20221003.11 |
| [18] | Harni V, Babic D, Hadzavdic S, Barisic D. Nonspecific lesions in patients with chronic vulvar discomfort revealed vulvodynia as chronic reflex pain syndrome (CRPS) type I. J Gynecol Obstet. 2022; 10(6): 243–252.
https://doi.org/10.11648/j.jgo.20221006.12 |
[9, 16-18]
.
The statistical coherence between symptom clusters and histopathological patterns further supports the conceptual shift from viewing CVD as a severity spectrum to recognizing it as a constellation of mechanism-based entities. Pain quality emerges as a biological signal reflecting the dominant nociceptive pathway engaged. This reconceptualization has direct therapeutic implications: interventions targeting neural sensitization may be prioritized in sharp-dominant phenotypes, whereas anti-inflammatory and anti-remodeling strategies may be more rational in dull-dominant inflammatory dermatoses.
Several limitations warrant consideration. The cross-sectional design limits inference regarding temporal evolution—whether sharp phenotypes may, over time, transition into remodeling-dominant states or remain mechanistically distinct cannot be determined. Quantitative nerve fiber density, molecular markers of neuroinflammation, and cytokine profiling were not incorporated, restricting direct histological–molecular correlation
. Additionally, pain descriptors were derived from structured interviews rather than formal quantitative sensory testing, which could have further delineated threshold alterations, hyperalgesia, or allodynia patterns
| [33] | Maier C, Baron R, Tölle TR, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): reference data for the trunk and head. Pain. 2011; 152(1): 262–274. https://doi.org/10.1016/j.pain.2010.10.002 |
[33]
. Finally, although the DATRIV population was rigorously stratified, replication in broader and non-specialist settings is necessary to confirm generalizability.
These limitations delineate future directions. Longitudinal designs could clarify whether sensory phenotypes remain stable or evolve alongside tissue remodeling and therapeutic response. Integration of quantitative sensory testing, immunohistochemistry, and molecular neuroimmune markers would enable deeper mechanistic mapping of fast versus slow nociceptive pathways
| [12] | Lauria G, Hsieh ST, Johansson O, et al. EFNS/PNS guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. Eur J Neurol. 2010; 17(7): 903–912.
https://doi.org/10.1111/j.1468-1331.2010.03023.x |
| [13] | Oaklander AL, Nolano M. Scientific advances in and clinical approaches to small-fiber polyneuropathy. JAMA Neurol. 2019; 76(11): 1240–1247.
https://doi.org/10.1001/jamaneurol.2019.1862 |
| [14] | Uceyler N, Zeller D, Kahn AK, et al. Small fibre pathology in patients with fibromyalgia syndrome. Brain. 2013; 136(Pt 6): 1857–1867. https://doi.org/10.1093/brain/awt053 |
| [15] | Oaklander AL, Klein MM. Evidence of small-fiber polyneuropathy in unexplained chronic pain syndromes. Pain. 2013; 154(11): 2310–2316.
https://doi.org/10.1016/j.pain.2013.06.001 |
| [33] | Maier C, Baron R, Tölle TR, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): reference data for the trunk and head. Pain. 2011; 152(1): 262–274. https://doi.org/10.1016/j.pain.2010.10.002 |
| [37] | Hore Z, Denk F. Neuroimmune interactions in chronic pain - An interdisciplinary perspective. Brain Behav Immun. 2019 Jul; 79: 56-62. https://doi.org/10.1016/j.bbi.2019.04.033 |
| [38] | Osborne, N. R.; Davis, K. D. Sex and Gender Differences in Pain. Int. Rev. Neurobiol. 2022, 164, 277–307.
https://doi.org/10.1016/bs.irn.2022.05.009 |
[12-15, 33, 37, 38]
. Such multimodal integration could ultimately refine classification systems and support mechanism-based treatment algorithms consistent with contemporary frameworks that define chronic pain as a disease entity with identifiable biological substrates
.
In summary, the findings substantiate a mechanistically grounded distinction “between sharp and dull.” Rather than representing merely descriptive variations of pain intensity, these sensory qualities appear to reflect fundamentally different biological processes operating within vulvar tissue. Sharp pain phenotypes correspond predominantly to neural sensitization and altered signal processing, whereas dull pain phenotypes arise in the context of inflammatory remodeling and sustained nociceptive input. Recognizing this divergence allows chronic vulvar discomfort to be interpreted not as a single clinical continuum but as a set of mechanism-based entities with distinct tissue substrates
| [1] | Bornstein J, Goldstein AT, Stockdale CK, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20(2): 126–130.
https://doi.org/10.1097/LGT.0000000000000194 |
| [4] | Goldstein AT, Pukall CF, Brown C, Bergeron S, Stein A, Kellogg-Spadt S. Vulvodynia: Assessment and Treatment. J Sex Med. 2016 Apr; 13(4): 572-90.
https://doi.org/10.1016/j.jsxm.2016.01.020 |
| [9] | Harni V, Babic D, Hadzavdic S, Barisic D, Karadza M. Burning, stinging, tenderness: sensory profiling of vulvar pain in chronic discomfort—A DATRIV study perspective. J Gynecol Obstet. 2024; 12(6): 118–131.
https://doi.org/10.11648/j.jgo.20241206.11 |
| [16] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the vulvoscopy index for detection of vulvar dermatoses (DATRIV Study, Part 1). J Gynecol Obstet. 2022; 10(1): 39–47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [17] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N–S–P scheme for detection of vulvar dermatoses (DATRIV Study, Part 2). J Gynecol Obstet. 2022; 10(3): 159–166.
https://doi.org/10.11648/j.jgo.20221003.11 |
| [18] | Harni V, Babic D, Hadzavdic S, Barisic D. Nonspecific lesions in patients with chronic vulvar discomfort revealed vulvodynia as chronic reflex pain syndrome (CRPS) type I. J Gynecol Obstet. 2022; 10(6): 243–252.
https://doi.org/10.11648/j.jgo.20221006.12 |
| [24] | Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011; 152 (Suppl 3): S2–S15.
https://doi.org/10.1016/j.pain.2010.09.030 |
| [25] | Treede RD, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain. Pain. 2019; 160(1): 19–27. https://doi.org/10.1097/j.pain.0000000000001384 |
| [26] | Baron R, Maier C, Attal N, et al. Peripheral neuropathic pain: a mechanism-related organizing principle. Pain. 2017; 158(2): 261–272. https://doi.org/10.1097/j.pain.0000000000000790 |
| [27] | Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology. 2008; 70(18): 1630–1635.
https://doi.org/10.1212/01.wnl.0000282763.29778.59 |
| [28] | Jensen TS, Finnerup NB. Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. Lancet Neurol. 2014; 13(9): 924–935.
https://doi.org/10.1016/S1474-4422(14)70102-4 |
[1, 4, 9, 16-18, 24-28]
.
5. Conclusion
The present study demonstrates that pain quality in chronic vulvar discomfort is not merely a descriptive component of clinical history but a biologically meaningful indicator consistently aligned with specific peripheral histopathological patterns. By systematically correlating structured sensory phenotypes with blinded microscopic evaluation, the analysis confirms that distinct qualitative pain categories correspond to divergent tissue substrates in vulvodynia and vulvar dermatoses.
Sharp, stabbing, knife-like, and cutting descriptors clustered with largely preserved epidermal and superficial dermal architecture, supporting a predominantly sensitization-driven or neuropathic phenotype. In contrast, dull descriptors—including burning, itching, aching, and soreness—were consistently associated with inflammatory infiltrates, epidermal remodeling, basal layer alteration, and dermal structural reorganization, indicating tissue-driven nociceptive activation. This structured alignment between sensory phenotype and morphological substrate supports the interpretation of pain quality as a mechanism-reflective clinical parameter.
Within the DATRIV diagnostic framework, the integration of three-rings vulvoscopy, the N–S–P scheme, and structured sensory profiling establishes complementary diagnostic layers: anatomical localization, lesion specificity, and functional nociceptive expression. Together, these dimensions enable mechanism-oriented differentiation between primarily neural dysregulation and inflammatory dermatoses, reducing diagnostic ambiguity and improving therapeutic alignment.
More broadly, these findings support a reconceptualization of chronic vulvar discomfort as a heterogeneous construct composed of biologically distinguishable entities. Pain in this setting should not be reduced to intensity alone but recognized as a patterned expression of neural-tissue interaction. Operationalizing the distinction between sharp and dull phenotypes advances clinical reasoning toward biologically informed diagnosis and individual management.
Abbreviations
CVD | Chronic Vulvar Discomfort |
DATRIV | Diagnostic Accuracy of Three Rings Vulvoscopy |
TRIV | Three-Rings Vulvoscopy |
ISSVD | The International Society for the Study of Vulvovaginal Disease |
FFPE | Formalin-Fixed Paraffin-Embedded |
H&E | Hematoxylin and Eosin |
Author Contributions
Vesna Harni: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing
Damir Babic: Conceptualization, Investigation, Methodology, Supervision, Validation
Suzana Ljubojevic Hadzavdic: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Supervision, Validation
Dubravko Barisic: Conceptualization, Methodology, Supervision
Magdalena Karadza: Conceptualization, Formal Analysis, Investigation, Methodology, Resources, Visualization
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Bornstein J, Goldstein AT, Stockdale CK, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20(2): 126–130.
https://doi.org/10.1097/LGT.0000000000000194
|
| [2] |
Leclair CM, Goetsch MF, Korcheva VB, Anderson R, Peters D, Morgan TK. Differences in primary compared with secondary vestibulodynia by immunohistochemistry. Obstet Gynecol. 2011; 117(6): 1307–1313.
https://doi.org/10.1097/AOG.0b013e31821f7db0
|
| [3] |
Reed BD, Harlow SD, Legocki LJ, et al. Chronic vulvar pain: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2012; 119(5): 1025–1033.
https://doi.org/10.1097/AOG.0b013e31824c3b8f
|
| [4] |
Goldstein AT, Pukall CF, Brown C, Bergeron S, Stein A, Kellogg-Spadt S. Vulvodynia: Assessment and Treatment. J Sex Med. 2016 Apr; 13(4): 572-90.
https://doi.org/10.1016/j.jsxm.2016.01.020
|
| [5] |
Nguyen RHN, Mathur C, Wynne C, et al. The impact of vulvodynia on quality of life. J Womens Health (Larchmt). 2012; 21(5): 522–530.
https://doi.org/10.1089/jwh.2011.2848
|
| [6] |
Arnold LD, Bachmann GA, Kelly S, Rosen R. Vulvodynia: characteristics and associations with comorbidities and quality of life. Am J Obstet Gynecol. 2006; 195(3): 835–840.
https://doi.org/10.1016/j.ajog.2006.06.005
|
| [7] |
Bohm-Starke N, Hilliges M, Falconer C, Rylander E. Neurochemical characterization of the vestibular nerves in women with vulvar vestibulitis syndrome. Gynecol Obstet Invest. 2001; 52(4): 243–248.
https://doi.org/10.1159/000010198
|
| [8] |
Farmer MA, Maykut CA, Baggish MS, Binik YM, Khalife S. Pain ratings and pain language in vulvodynia. Pain Res Manag. 2010; 15(1): 1–6.
https://doi.org/10.1155/2010/847613
|
| [9] |
Harni V, Babic D, Hadzavdic S, Barisic D, Karadza M. Burning, stinging, tenderness: sensory profiling of vulvar pain in chronic discomfort—A DATRIV study perspective. J Gynecol Obstet. 2024; 12(6): 118–131.
https://doi.org/10.11648/j.jgo.20241206.11
|
| [10] |
Bornstein J, Preti M, Radici G, Stockdale CK, Vieira-Baptista P. Vulvodynia: a neglected chronic pain diagnosis. Pain. 2019 Jul; 160(7): 1680-1681.
https://doi.org/10.1097/j.pain.0000000000001559
|
| [11] |
Edwards L. Vulvodynia. Clin Obstet Gynecol. 2015 Mar; 58(1): 143-52.
https://doi.org/10.1097/GRF.0000000000000093
|
| [12] |
Lauria G, Hsieh ST, Johansson O, et al. EFNS/PNS guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. Eur J Neurol. 2010; 17(7): 903–912.
https://doi.org/10.1111/j.1468-1331.2010.03023.x
|
| [13] |
Oaklander AL, Nolano M. Scientific advances in and clinical approaches to small-fiber polyneuropathy. JAMA Neurol. 2019; 76(11): 1240–1247.
https://doi.org/10.1001/jamaneurol.2019.1862
|
| [14] |
Uceyler N, Zeller D, Kahn AK, et al. Small fibre pathology in patients with fibromyalgia syndrome. Brain. 2013; 136(Pt 6): 1857–1867.
https://doi.org/10.1093/brain/awt053
|
| [15] |
Oaklander AL, Klein MM. Evidence of small-fiber polyneuropathy in unexplained chronic pain syndromes. Pain. 2013; 154(11): 2310–2316.
https://doi.org/10.1016/j.pain.2013.06.001
|
| [16] |
Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the vulvoscopy index for detection of vulvar dermatoses (DATRIV Study, Part 1). J Gynecol Obstet. 2022; 10(1): 39–47.
https://doi.org/10.11648/j.jgo.20221001.16
|
| [17] |
Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N–S–P scheme for detection of vulvar dermatoses (DATRIV Study, Part 2). J Gynecol Obstet. 2022; 10(3): 159–166.
https://doi.org/10.11648/j.jgo.20221003.11
|
| [18] |
Harni V, Babic D, Hadzavdic S, Barisic D. Nonspecific lesions in patients with chronic vulvar discomfort revealed vulvodynia as chronic reflex pain syndrome (CRPS) type I. J Gynecol Obstet. 2022; 10(6): 243–252.
https://doi.org/10.11648/j.jgo.20221006.12
|
| [19] |
Vural E, Kecici AS, Sevim DG, et al. Human epidermal thickness at different body sites: a histometric study. Int J Morphol. 2022; 40(1): 67–74.
https://doi.org/10.4067/S0717-95022022000100067
|
| [20] |
Weedon D. Weedon’s skin pathology. 5th ed. Elsevier; 2020.
|
| [21] |
Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X. Lever’s histopathology of the skin. 11th ed. Wolters Kluwer; 2014.
|
| [22] |
Calonje E, Brenn T, Lazar AJ, Billings SD. McKee’s pathology of the skin. 5th ed. Elsevier; 2020.
|
| [23] |
Barnhill RL, Crowson AN, Magro CM, Piepkorn M. Dermatopathology. 4th ed. McGraw-Hill; 2020.
|
| [24] |
Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011; 152 (Suppl 3): S2–S15.
https://doi.org/10.1016/j.pain.2010.09.030
|
| [25] |
Treede RD, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain. Pain. 2019; 160(1): 19–27.
https://doi.org/10.1097/j.pain.0000000000001384
|
| [26] |
Baron R, Maier C, Attal N, et al. Peripheral neuropathic pain: a mechanism-related organizing principle. Pain. 2017; 158(2): 261–272.
https://doi.org/10.1097/j.pain.0000000000000790
|
| [27] |
Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology. 2008; 70(18): 1630–1635.
https://doi.org/10.1212/01.wnl.0000282763.29778.59
|
| [28] |
Jensen TS, Finnerup NB. Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. Lancet Neurol. 2014; 13(9): 924–935.
https://doi.org/10.1016/S1474-4422(14)70102-4
|
| [29] |
Tracey I, Mantyh PW. The cerebral signature for pain perception and its modulation. Neuron. 2007; 55(3): 377–391.
https://doi.org/10.1016/j.neuron.2007.07.012
|
| [30] |
Basbaum AI, Bautista DM, Scherrer G, Julius D. Cellular and molecular mechanisms of pain. Cell. 2009; 139(2): 267–284.
https://doi.org/10.1016/j.cell.2009.10.028
|
| [31] |
McMahon SB, Koltzenburg M, Tracey I, Turk DC, editors. Wall & Melzack’s textbook of pain. 6th ed. Elsevier; 2013.
|
| [32] |
Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013; 154 (Suppl 1): S29–S43.
https://doi.org/10.1016/j.pain.2013.09.001
|
| [33] |
Maier C, Baron R, Tölle TR, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): reference data for the trunk and head. Pain. 2011; 152(1): 262–274.
https://doi.org/10.1016/j.pain.2010.10.002
|
| [34] |
Bohm-Starke N, Hilliges M, Falconer C, Rylander E. Increased intraepithelial innervation in women with vulvar vestibulitis syndrome. Gynecol Obstet Invest. 1998; 46(4): 256–260.
https://doi.org/10.1159/000010045
|
| [35] |
Papoutsis D, Haefner HK, Crum CP, Opipari AW Jr, Reed BD. Vestibular mast cell density in vulvodynia: a case-controlled study. J Low Genit Tract Dis. 2016; 20(3): 275–279.
https://doi.org/10.1097/LGT.0000000000000206
|
| [36] |
Reed BD, Plegue MA, Sen A, Haefner HK, Siddiqui J, Remick DG. Nerve growth factor and selected cytokines in women with and without vulvodynia. J Low Genit Tract Dis. 2018; 22(2): 139–146.
https://doi.org/10.1097/LGT.0000000000000370
|
| [37] |
Hore Z, Denk F. Neuroimmune interactions in chronic pain - An interdisciplinary perspective. Brain Behav Immun. 2019 Jul; 79: 56-62.
https://doi.org/10.1016/j.bbi.2019.04.033
|
| [38] |
Osborne, N. R.; Davis, K. D. Sex and Gender Differences in Pain. Int. Rev. Neurobiol. 2022, 164, 277–307.
https://doi.org/10.1016/bs.irn.2022.05.009
|
Cite This Article
-
APA Style
Harni, V., Babic, D., Hadzavdic, S. L., Barisic, D., Karadza, M. (2026). Pain Quality and Tissue Signatures: Histopathological Insights into Vulvodynia and Vulvar Dermatoses. Journal of Gynecology and Obstetrics, 14(2), 50-64. https://doi.org/10.11648/j.jgo.20261402.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Harni, V.; Babic, D.; Hadzavdic, S. L.; Barisic, D.; Karadza, M. Pain Quality and Tissue Signatures: Histopathological Insights into Vulvodynia and Vulvar Dermatoses. J. Gynecol. Obstet. 2026, 14(2), 50-64. doi: 10.11648/j.jgo.20261402.11
Copy
|
Download
AMA Style
Harni V, Babic D, Hadzavdic SL, Barisic D, Karadza M. Pain Quality and Tissue Signatures: Histopathological Insights into Vulvodynia and Vulvar Dermatoses. J Gynecol Obstet. 2026;14(2):50-64. doi: 10.11648/j.jgo.20261402.11
Copy
|
Download
-
@article{10.11648/j.jgo.20261402.11,
author = {Vesna Harni and Damir Babic and Suzana Ljubojevic Hadzavdic and Dubravko Barisic and Magdalena Karadza},
title = {Pain Quality and Tissue Signatures: Histopathological Insights into Vulvodynia and Vulvar Dermatoses},
journal = {Journal of Gynecology and Obstetrics},
volume = {14},
number = {2},
pages = {50-64},
doi = {10.11648/j.jgo.20261402.11},
url = {https://doi.org/10.11648/j.jgo.20261402.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20261402.11},
abstract = {OBJECTIVE: To determine whether qualitative pain characteristics in chronic vulvar discomfort correspond to diagnosis-specific epidermal and dermal histopathological patterns in vulvodynia and vulvar dermatoses. METHODS: This prospective observational sub-analysis of the DATRIV study included 328 women equally stratified into four groups: normal vulva, impaired asymptomatic vulvar skin, vulvodynia, and vulvar dermatoses (n = 82 per group). Pain quality was assessed using structured clinical interviews and categorized as sharp (fast) or dull (slow) descriptors. Vulvar biopsies underwent blinded histopathological evaluation of epidermal architecture and dermal features, including inflammatory infiltrates, fibrosis, vascularity, adnexal structures, nerve fibers, and mast cells. Associations between pain quality, histopathological findings, and symptom duration were analyzed using proportion tests, pairwise comparisons, and multivariate models. RESULTS: Epidermal architecture was largely preserved in normal vulva, impaired asymptomatic skin, and vulvodynia, whereas epidermal thinning, atrophy, and keratinization disorders were predominantly confined to vulvar dermatoses (p CONCLUSION: Chronic vulvar discomfort demonstrates diagnosis-specific sensory–histopathological coupling. Vulvodynia is characterized by sharp, fast pain qualities linked to a neurocutaneous dermal phenotype, whereas vulvar dermatoses are dominated by dull, slow, inflammation-driven nociception associated with fibrotic remodeling. Integrating structured pain quality assessment with histopathological evaluation enhances diagnostic differentiation and supports mechanism-oriented stratification and individualized management.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Pain Quality and Tissue Signatures: Histopathological Insights into Vulvodynia and Vulvar Dermatoses
AU - Vesna Harni
AU - Damir Babic
AU - Suzana Ljubojevic Hadzavdic
AU - Dubravko Barisic
AU - Magdalena Karadza
Y1 - 2026/03/26
PY - 2026
N1 - https://doi.org/10.11648/j.jgo.20261402.11
DO - 10.11648/j.jgo.20261402.11
T2 - Journal of Gynecology and Obstetrics
JF - Journal of Gynecology and Obstetrics
JO - Journal of Gynecology and Obstetrics
SP - 50
EP - 64
PB - Science Publishing Group
SN - 2376-7820
UR - https://doi.org/10.11648/j.jgo.20261402.11
AB - OBJECTIVE: To determine whether qualitative pain characteristics in chronic vulvar discomfort correspond to diagnosis-specific epidermal and dermal histopathological patterns in vulvodynia and vulvar dermatoses. METHODS: This prospective observational sub-analysis of the DATRIV study included 328 women equally stratified into four groups: normal vulva, impaired asymptomatic vulvar skin, vulvodynia, and vulvar dermatoses (n = 82 per group). Pain quality was assessed using structured clinical interviews and categorized as sharp (fast) or dull (slow) descriptors. Vulvar biopsies underwent blinded histopathological evaluation of epidermal architecture and dermal features, including inflammatory infiltrates, fibrosis, vascularity, adnexal structures, nerve fibers, and mast cells. Associations between pain quality, histopathological findings, and symptom duration were analyzed using proportion tests, pairwise comparisons, and multivariate models. RESULTS: Epidermal architecture was largely preserved in normal vulva, impaired asymptomatic skin, and vulvodynia, whereas epidermal thinning, atrophy, and keratinization disorders were predominantly confined to vulvar dermatoses (p CONCLUSION: Chronic vulvar discomfort demonstrates diagnosis-specific sensory–histopathological coupling. Vulvodynia is characterized by sharp, fast pain qualities linked to a neurocutaneous dermal phenotype, whereas vulvar dermatoses are dominated by dull, slow, inflammation-driven nociception associated with fibrotic remodeling. Integrating structured pain quality assessment with histopathological evaluation enhances diagnostic differentiation and supports mechanism-oriented stratification and individualized management.
VL - 14
IS - 2
ER -
Copy
|
Download