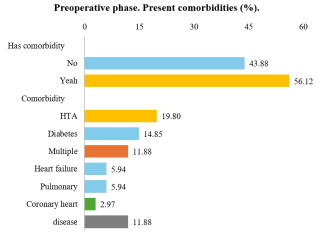
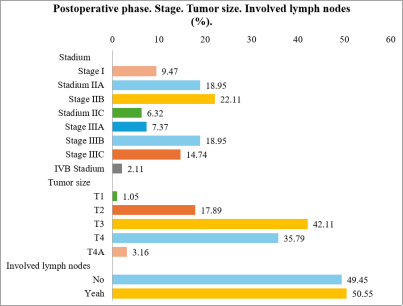
Colon cancer is a major cause of mortality worldwide. This study evaluates postoperative mortality and associated risk factors in patients undergoing laparoscopic resection, highlighting the benefits of this approach and the need to investigate outcomes and recurrence. The objective was to evaluate postoperative mortality in colon cancer treated laparoscopically, identify associated factors, the most frequent histopathologies, and the predominant location of the tumor in patients in a high-complexity hospital located in Norte de Santander, Colombia. A quantitative, descriptive, retrospective, and cross-sectional study was conducted, analyzing data from patients treated between 2020 and 2024 based on medical records. Risk factors, comorbidities, and postoperative complications were assessed. Statistical tests such as Chi-square, Student's t-test, Kaplan-Meier, and Receiver Operating Characteristic curves were applied to evaluate the efficacy and safety of laparoscopic management. Postoperative mortality in the laparoscopic group was 12.24%. The most common comorbidities were hypertension (19.80%) and diabetes mellitus (14.85%). Moderately differentiated adenocarcinoma was present in 44.90% of cases, with tumor distribution evenly distributed between the right and left colon (45.92% in each case). Clinical stage IIB was present in 22.11% of patients, and 42.11% were classified as T3. Postoperative mortality was 12.24%, primarily due to tumor progression. Factors associated with higher mortality included stage IIB, lymph node involvement (50.55%), and comorbidities such as hypertension and diabetes. Early staging and control of comorbidities are crucial to improve postoperative outcomes.
| Published in | Journal of Surgery (Volume 13, Issue 4) |
| DOI | 10.11648/j.js.20251304.16 |
| Page(s) | 100-111 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Mortality, Laparoscopy, Surgical Management, Minimally Invasive Surgery, Risk Facto
Age (years) | Patients | % |
|---|---|---|
Adulthood | 38 | 38,78 |
Older adult | 60 | 61,22 |
98 | 100 |
Year | Patients | % |
|---|---|---|
2020 | 23 | 23,47 |
2021 | 23 | 23,47 |
2022 | 21 | 21,43 |
2023 | 21 | 21,43 |
2024 | 10 | 10,20 |
98 | 100,00 |
Mean | Deviation | C.V. (%) | Mínimum | Máximum | |
|---|---|---|---|---|---|
Overall | 26,0 | 4,39 | 16,88 | 17,2 | 38,1 |
Age group | |||||
Adulthood | 26,5 | 4,40 | 16,60 | 17,2 | 35,7 |
Older Adult | 25,7 | 4,38 | 17,04 | 17,3 | 38,1 |
patient’s gender | |||||
Female | 26,4 | 4,89 | 18,52 | 17,2 | 38,1 |
Male | 25,5 | 3,70 | 14,51 | 17,3 | 33,1 |
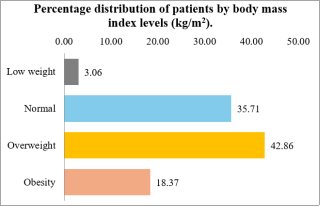
Underweight: BMI less than 18.5 kg/m² |
Normal weight: BMI between 18.5 and 24.9 kg/m² |
Overweight: BMI between 25 and 29.9 kg/m² |
Obesity: BMI equal to or greater than 30 kg/m² |
Level | Patients | % |
|---|---|---|
Underweight to normal | 38 | 38.78% |
Overweight to obesity | 60 | 61.22% |
Total | 98 | 100% |
Age (years) | Female | Male | Total |
|---|---|---|---|
Adulthood | 22.45% | 16.33% | 38.78% |
Older Adult | 31.63% | 29.59% | 61.22% |
Total | 54.08% | 45.92% | 100.00% |
Age (years) | Underweight to Normal | Overweight to Obesity | Total |
|---|---|---|---|
Adulthood | 12.24% | 26.53% | 38.78% |
Older Adult | 26.53% | 34.69% | 61.22% |
Total | 38.78% | 61.22% | 100.00% |
Items | Response | Patients | % |
|---|---|---|---|
Surgical Conversion | No | 93 | 94.90% |
Yes | 5 | 5.10% | |
Total | 98 | 100% | |
Indication for Conversion | Adhesions | 1 | 20.00% |
Technical difficulty | 1 | 20.00% | |
Tumor size | 1 | 20.00% | |
Infiltration to others | 2 | 40.00% | |
Total | 5 | 100% | |
Previous Surgery | No | 72 | 73.47% |
Yes | 26 | 26.53% | |
Total | 98 | 100% | |
Which Previous Surgery? | Kocher incision | 8 | 30.77% |
Pfannenstiel | 5 | 19.23% | |
Laparotomy | 4 | 15.38% | |
Infraumbilical midline | 4 | 15.38% | |
Supraumbilical midline | 3 | 11.54% | |
Rocky Davis | 2 | 7.69% | |
Total | 26 | 100% |
Items | Response | Patients | % |
|---|---|---|---|
Bleeding | 0 - 100 ml | 73 | 74.49% |
101 - 200 ml | 18 | 18.37% | |
201 - 500 ml | 7 | 7.14% | |
Total | 98 | 100% | |
ASA Classification | (II) Mild to moderate systemic disease, medically well controlled without functional limitation | 83 | 84.69% |
(III) Severe systemic disease resulting in functional limitation | 15 | 15.31% | |
Total | 98 | 100% |
Items | Response | Patients | % |
|---|---|---|---|
Tumor Location | Right colon cancer (total) | 45 | 45.92% |
Right colon tumor | 31 | 31.63% | |
Proximal colon tumor | 8 | 8.16% | |
Right colon tumor extending to hepatic flexure | 6 | 6.12% | |
Left colon cancer (total) | 45 | 45.92% | |
Left sigmoid colon | 18 | 18.37% | |
Left colon: rectum and mid-rectum | 14 | 14.29% | |
Left sigmoid colon and rectosigmoid junction | 9 | 9.18% | |
Descending colon cancer | 4 | 4.08% | |
Right colon plus left colon | 8 | 8.16% | |
Total | 98 | 100% |
Malignant Histology | ||
|---|---|---|
Moderately differentiated adenocarcinoma | 44 | 44.90% |
Well-differentiated adenocarcinoma | 30 | 30.61% |
Mucinous adenocarcinoma | 7 | 7.14% |
Poorly differentiated | 6 | 6.12% |
Other | 11 | 11.22% |
Total | 98 | 100% |
Items | Response | Patients | % |
|---|---|---|---|
Number of lymph nodes | < 8 | 1 | 1.09% |
8-11 | 17 | 18.48% | |
> 11 | 74 | 80.43% | |
Total | 92 | 100% | |
Involved lymph nodes | 0 (None) | 51 | 52.58 % |
1 | 16 | 16.49% | |
2-3 | 9 | 9.28% | |
4-6 | 5 | 5.15% | |
≥ 7 | 16 | 16.49% | |
Total | 12 | 100% |
Items | Response | Patients | % |
|---|---|---|---|
ICU Admission | No | 68 | 69.39% |
Yes | 30 | 30.61% | |
Total | 98 | 100% | |
Readmission | No | 93 | 94.90% |
Yes | 5 | 5.10% | |
Total | 98 | 100% |
Items | Response | Patients | % |
|---|---|---|---|
Status | Alive | 86 | 87.76% |
Deceased | 12 | 12.24% | |
Total | 98 | 100% | |
Death due to other causes | No | 2 | 16.67% |
Yes | 10 | 83.33% | |
Total | 12 | 100% | |
Cause of death | Tumor extension | 6 | 60.00% |
Paraneoplastic syndrome | 2 | 20.00% | |
Mesenteric ischemia | 1 | 10.00% | |
Sepsis + paralytic ileus | 1 | 10.00% | |
Total | 10 | 100% |
Variable | Category | Survival | Survival (%) | P-value |
|---|---|---|---|---|
Overall | All | 0.670 | 67.0 | |
Age groups | Adult | 0.758 | 75.8 | 0.063 * |
Older adult | 0.591 | 59.1 | ||
Sex | Female | 0.676 | 67.6 | 0.599 ns |
Male | 0.653 | 65.3 | ||
BMI categories | Low to normal | 0.603 | 60.3 | 0.378 ns |
Overweight to obese | 0.714 | 71.4 | ||
Comorbidity | Absent | 0.756 | 75.6 | 0.190 ns |
Present | 0.612 | 61.2 | ||
Lymph node involvement | Absent | 0.899 | 89.9 | 0.133 ns |
Present | 0.400 | 40.0 | ||
ASA classification | II | 0.689 | 68.9 | 0.010 * |
III | 0.495 | 49.5 | ||
Reintervention | Absent | 0.713 | 71.3 | 0.000 ** |
Present | 0.298 | 29.8 |
CRC | Colorectal Cancer |
COPD | Chronic Obstructive Pulmonary Disease |
ASA | American Society of Anesthesiologist |
ROC | Receiver Operating Characteristic |
WHO | World Health Organization |
| [1] | Arias, F. R., Armijos, Q. D., Risueño, V. F., et al. (2023). Colorectal cancer - diagnosis and treatment: A literature review. Gastroenterol Latinoam, 34(1), 31-38. |
| [2] | Barrera, E. A., & Muñoz, P. N. (2020). Laparoscopic surgery in colon cancer. Rev Cir, 72(2), 164-170. |
| [3] | Chen, Y., Xi, D., & Zhang, Q. (2022). Laparoscopic radical resection versus routine surgery for colorectal cancer. Comput Math Methods Med, 2022, Article ID 4899555. |
| [4] | Manterola, C., Pineda, V., & Vial, M. (2005). Open versus laparoscopic resection in non-complicated colon cancer: A systematic review. Rev Chil Cir [Cir Esp], 78(1), 28-33. |
| [5] | Márquez-Ustáriz, A., Guerrero-Macías, S., Burgos-Sánchez, R., Campillo-Pardo, J., Bustos-Guerrero, A., García-Mora, M., et al. (2023). Update on colorectal cancer screening. Rev Colomb Cancerol, 27(Suppl 3), 291-300. |
| [6] | Vanegas-Moreno, D. P., Ramírez López, L. X., Limas Solano, L. M., Pedraza Bernal, A. M., & Monroy Díaz, A. L. (2020). Factors associated with colorectal cancer. Rev Med Risaralda, 26(1), 68-77. |
| [7] | Miranda, B. C. J., Tustumi, F., Nakamura, E. T., Shimanoe, V. H., Kikawa, D., & Waisberg, J. (2024). Obesity and colorectal cancer: A narrative review. Medicina, 60(8), 1218. |
| [8] | Qiu, H., Wang, L., Zhou, L., & Wang, X. (2023). Comorbidity patterns in patients newly diagnosed with colorectal cancer: A network-based study. JMIR Public Health Surveill, 9, e41999. |
| [9] | Charúa-Guindic, L., Lagunes-Gasca, A. A., Villanueva-Herrero, J. A., et al. (2009). Epidemiologic behavior of colon and rectal cancer in the General Hospital of Mexico: A 20‑year analysis, 1988-2007. Rev Gastroenterol Mex, 74(2), 99-104. |
| [10] | Villegas-Mejía, C. R., Chacón-Cardona, J. A., Villegas-Jaramillo, M., & Villegas-Jaramillo, P. (2018). Colon cancer: A single entity? Considerations on laterality in a Colombian oncological institution (2001-2016). Rev CES Med, 32(3), 191-202. |
| [11] | Cheng, L., Eng, C., Nieman, L. Z., Kapadia, A. S., & Du, X. L. (2011). Trends in colorectal cancer incidence by anatomic site and disease stage in the United States from 1976 to 2005. Am J Clin Oncol, 34(6), 573-580. |
| [12] | Instituto Nacional de Cancerología ESE (National Cancer Institute - Colombia). Clinical practice guideline (CPG) for early detection, diagnosis, treatment, follow-up, and rehabilitation of patients diagnosed with colon and rectal cancer: patient and caregiver version. Bogotá: Instituto Nacional de Cancerología ESE; 2013. Guideline No. GPC-2013-20. |
| [13] |
American Cancer Society. What is colorectal cancer? [Internet]. Atlanta (GA): American Cancer Society; [cited 3 Aug 2025]. Available from:
https://www.cancer.org/es/cancer/cancer-de-colon-y-recto/acerca/que-es.html |
| [14] |
Macrae FA, Parikh AR, Ricciardi R. Clinical presentation, diagnosis, and staging of colorectal cancer [Internet]. In: Tanabe KK, editor. UpToDate, Waltham (MA): UpToDate; 2025. Available from:
https://www.uptodate.com/contents/clinical-presentation-diagnosis-and-staging-of-colorectal-cancer |
| [15] | Torrecillas-Torres L, Cervantes-Sánchez G, Cárdenas E, Martínez B, Reyes-Pérez JA, Sánchez IC, et al. Recommendations for diagnosis and treatment of colon and rectal cancer in Mexico. Gac Mex Oncol. 2019 Dec; 18(4): 265-327. Epub 08-Aug-2022. |
| [16] | Thompson MR, O’Leary DP, Flashman K, et al. Clinical assessment to determine the risk of bowel cancer using Symptoms, Age, Mass and Iron deficiency anaemia (SAMI). Br J Surg. 2017; 104(11): 1393-400. |
APA Style
Monserrat, G. C. P., David, J. B. C., Hender, H. M., Alexander, B. F., Deivis, L. M. (2025). Mortality Associated with Laparoscopic Surgery for Colon Cancer in a Tertiary Care Institution in Norte de Santander, Colombia: A Retrospective Analysis from 2020 to 2024 (Period A). Journal of Surgery, 13(4), 100-111. https://doi.org/10.11648/j.js.20251304.16
ACS Style
Monserrat, G. C. P.; David, J. B. C.; Hender, H. M.; Alexander, B. F.; Deivis, L. M. Mortality Associated with Laparoscopic Surgery for Colon Cancer in a Tertiary Care Institution in Norte de Santander, Colombia: A Retrospective Analysis from 2020 to 2024 (Period A). J. Surg. 2025, 13(4), 100-111. doi: 10.11648/j.js.20251304.16
AMA Style
Monserrat GCP, David JBC, Hender HM, Alexander BF, Deivis LM. Mortality Associated with Laparoscopic Surgery for Colon Cancer in a Tertiary Care Institution in Norte de Santander, Colombia: A Retrospective Analysis from 2020 to 2024 (Period A). J Surg. 2025;13(4):100-111. doi: 10.11648/j.js.20251304.16
@article{10.11648/j.js.20251304.16,
author = {Guerrero Contreras Pierina Monserrat and Julio Blanco Cesar David and Hernández Martínez Hender and Bahamón Flórez Alexander and López Melo Deivis},
title = {Mortality Associated with Laparoscopic Surgery for Colon Cancer in a Tertiary Care Institution in Norte de Santander, Colombia: A Retrospective Analysis from 2020 to 2024 (Period A)
},
journal = {Journal of Surgery},
volume = {13},
number = {4},
pages = {100-111},
doi = {10.11648/j.js.20251304.16},
url = {https://doi.org/10.11648/j.js.20251304.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251304.16},
abstract = {Colon cancer is a major cause of mortality worldwide. This study evaluates postoperative mortality and associated risk factors in patients undergoing laparoscopic resection, highlighting the benefits of this approach and the need to investigate outcomes and recurrence. The objective was to evaluate postoperative mortality in colon cancer treated laparoscopically, identify associated factors, the most frequent histopathologies, and the predominant location of the tumor in patients in a high-complexity hospital located in Norte de Santander, Colombia. A quantitative, descriptive, retrospective, and cross-sectional study was conducted, analyzing data from patients treated between 2020 and 2024 based on medical records. Risk factors, comorbidities, and postoperative complications were assessed. Statistical tests such as Chi-square, Student's t-test, Kaplan-Meier, and Receiver Operating Characteristic curves were applied to evaluate the efficacy and safety of laparoscopic management. Postoperative mortality in the laparoscopic group was 12.24%. The most common comorbidities were hypertension (19.80%) and diabetes mellitus (14.85%). Moderately differentiated adenocarcinoma was present in 44.90% of cases, with tumor distribution evenly distributed between the right and left colon (45.92% in each case). Clinical stage IIB was present in 22.11% of patients, and 42.11% were classified as T3. Postoperative mortality was 12.24%, primarily due to tumor progression. Factors associated with higher mortality included stage IIB, lymph node involvement (50.55%), and comorbidities such as hypertension and diabetes. Early staging and control of comorbidities are crucial to improve postoperative outcomes.},
year = {2025}
}
TY - JOUR T1 - Mortality Associated with Laparoscopic Surgery for Colon Cancer in a Tertiary Care Institution in Norte de Santander, Colombia: A Retrospective Analysis from 2020 to 2024 (Period A) AU - Guerrero Contreras Pierina Monserrat AU - Julio Blanco Cesar David AU - Hernández Martínez Hender AU - Bahamón Flórez Alexander AU - López Melo Deivis Y1 - 2025/08/16 PY - 2025 N1 - https://doi.org/10.11648/j.js.20251304.16 DO - 10.11648/j.js.20251304.16 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 100 EP - 111 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20251304.16 AB - Colon cancer is a major cause of mortality worldwide. This study evaluates postoperative mortality and associated risk factors in patients undergoing laparoscopic resection, highlighting the benefits of this approach and the need to investigate outcomes and recurrence. The objective was to evaluate postoperative mortality in colon cancer treated laparoscopically, identify associated factors, the most frequent histopathologies, and the predominant location of the tumor in patients in a high-complexity hospital located in Norte de Santander, Colombia. A quantitative, descriptive, retrospective, and cross-sectional study was conducted, analyzing data from patients treated between 2020 and 2024 based on medical records. Risk factors, comorbidities, and postoperative complications were assessed. Statistical tests such as Chi-square, Student's t-test, Kaplan-Meier, and Receiver Operating Characteristic curves were applied to evaluate the efficacy and safety of laparoscopic management. Postoperative mortality in the laparoscopic group was 12.24%. The most common comorbidities were hypertension (19.80%) and diabetes mellitus (14.85%). Moderately differentiated adenocarcinoma was present in 44.90% of cases, with tumor distribution evenly distributed between the right and left colon (45.92% in each case). Clinical stage IIB was present in 22.11% of patients, and 42.11% were classified as T3. Postoperative mortality was 12.24%, primarily due to tumor progression. Factors associated with higher mortality included stage IIB, lymph node involvement (50.55%), and comorbidities such as hypertension and diabetes. Early staging and control of comorbidities are crucial to improve postoperative outcomes. VL - 13 IS - 4 ER -
Health Sciences, University of Santander, Cúcuta, Colombia
Health Sciences, University of Santander, Cúcuta, Colombia
Gastrointestinal Surgery Service, Universidad Nacional de Colombia, Hospital Universitario Erasmo Meoz, Cúcuta, Colombia
Colon and Rectal Surgery Service, Universidad Industrial de Santander, Erasmo Meoz University Hospital, Cúcuta, Colombia
Information