Primary cystadenocarcinoma of the mesentery is an extremely rare malignant cystic epithelial tumor and represents the malignant spectrum of mesenteric mucinous cystic neoplasms. Due to its rarity, fewer than 25 cases have been reported in the literature, and the clinical characteristics, diagnostic features, and optimal management strategies remain poorly defined. Patients usually present with nonspecific symptoms related to mass effect, including abdominal pain, abdominal distension, nausea, vomiting, constipation, or a palpable abdominal mass, often mimicking ovarian or gastrointestinal tumors. Preoperative diagnosis is particularly challenging because radiological findings are not pathognomonic and tumor markers have limited diagnostic value. We report a rare case of primary mesenteric cystadenocarcinoma in a 20-year-old female who presented with progressive abdominal distension, abdominal pain, nausea, vomiting, constipation, and exertional shortness of breath. Clinical examination revealed a large abdominal mass. Contrast-enhanced positron emission tomography–computed tomography demonstrated a large lobulated abdominopelvic mass with internal septations and heterogeneous enhancement, producing significant mass effect including bilateral ureteric dilatation and hydronephrosis. However, the exact origin of the lesion could not be determined preoperatively. Exploratory laparotomy revealed a large cystic mass arising from the mesentery with dense adhesions to the colon. Complete surgical excision was performed without rupture. Histopathological examination confirmed papillary mucinous cystadenocarcinoma of mesenteric origin. This case highlights the diagnostic difficulty associated with mesenteric cystic malignancies and emphasizes that complete surgical excision remains essential for definitive diagnosis and management.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Cystadenocarcinoma of the mesentery is an extremely rare malignant cystic epithelial tumor arising from mesenteric tissue and represents the malignant counterpart of benign or borderline mesenteric mucinous cystic neoplasms
[1]
Metaxas, G., Tangalos, A., Pappa, P., Papageorgiou, I. Mucinous cystic neoplasms of the mesentery: A case report and review of the literature. World Journal of Surgical Oncology. 2009, 7, 47.
. Mesenteric cystic tumors have an estimated incidence ranging from 1:27,000 to 1:250,000 in adults, with a reported malignancy rate of approximately 3%
[1]
Metaxas, G., Tangalos, A., Pappa, P., Papageorgiou, I. Mucinous cystic neoplasms of the mesentery: A case report and review of the literature. World Journal of Surgical Oncology. 2009, 7, 47.
. Fewer than 25 cases of primary mesenteric cystadenocarcinoma have been documented in the literature to date
[1]
Metaxas, G., Tangalos, A., Pappa, P., Papageorgiou, I. Mucinous cystic neoplasms of the mesentery: A case report and review of the literature. World Journal of Surgical Oncology. 2009, 7, 47.
Sobnach, S., Singh, B., Satyapal, K. S., et al. Primary seromucinous cystadenocarcinoma of the mesentery. South African Journal of Surgery. 2016, 54(3), 44–45.
[7]
Jaiswal, R., Dubey, D. B., Singh, R., Mishra, A. Recurrent mucinous cystic neoplasm of the mesentery in a young nullipara mimicking ovarian carcinoma. Journal of Cancer Research and Therapeutics. 2024, 20, 454–456.
Clinically, these tumors present with nonspecific symptoms such as abdominal pain, distension, nausea, vomiting, constipation, or a palpable abdominal mass, often mimicking ovarian, pancreatic, or appendiceal neoplasms
[2]
Jayaraghavan, R., Bhat, G. Mucinous cystic neoplasm of the mesentery: A case report. Cureus. 2022, 14(1), e21482.
Obuchi, T., Sasaki, A., Wakabayashi, G., et al. Serous cystadenocarcinoma of the mesentery in a man: A case report and review of the literature. Gastroenterology Report. 2014, 2(4), 306–310.
Sobnach, S., Singh, B., Satyapal, K. S., et al. Surgical excision as definitive treatment of mesenteric cystic malignancies. South African Journal of Surgery. 2016, 54(3), 44–45.
[2, 5, 8]
. Preoperative diagnosis remains challenging, as imaging findings are not pathognomonic and tumor markers have limited diagnostic utility
[3]
Hozaka, Y., Murakami, T., Kato, T., et al. Usefulness of 18F-FDG PET/CT in primary cystadenocarcinoma of the mesentery: A case report. Surgical Case Reports. 2020, 6, 306.
Hozaka, Y., Murakami, T., Kato, T., et al. Malignancy suspicion in mesenteric cystic tumors using PET/CT imaging. Surgical Case Reports. 2020, 6, 306.
[3, 6]
. Consequently, definitive diagnosis relies on histopathological examination following complete surgical excision
[1]
Metaxas, G., Tangalos, A., Pappa, P., Papageorgiou, I. Mucinous cystic neoplasms of the mesentery: A case report and review of the literature. World Journal of Surgical Oncology. 2009, 7, 47.
Jaiswal, R., Dubey, D. B., Singh, R., Mishra, A. Recurrent mucinous cystic neoplasm of the mesentery in a young nullipara mimicking ovarian carcinoma. Journal of Cancer Research and Therapeutics. 2024, 20, 454–456.
This presents a descriptive single-patient case report managed in the Department of Surgery, Saraswathi Institute of Medical Sciences, Hapur, Uttar Pradesh, India. The report was prepared following standard institutional clinical and academic practices for documenting rare surgical conditions. The case involved a 20-year-old female who presented with progressive abdominal distension, abdominal pain, nausea, vomiting, constipation, and exertional shortness of breath. Owing to the rarity of primary mesenteric cystadenocarcinoma and its unusual presentation in a young patient, the case was selected for detailed reporting.
A comprehensive clinical evaluation was undertaken, including detailed history-taking and thorough general and abdominal examination. Routine preoperative haematological and biochemical investigations were performed, with particular attention to identifying anaemia and features suggestive of a large intra-abdominal mass with pressure effects. Clinical findings were correlated with imaging studies to guide further management.
Radiological assessment was performed using contrast-enhanced positron emission tomography–computed tomography of the abdomen and pelvis. Imaging was evaluated for lesion size, anatomical location, internal characteristics such as septations and density, relationship to adjacent organs, and secondary effects including ureteric compression and hydronephrosis. Despite advanced imaging, the exact origin and nature of the lesion could not be definitively established preoperatively.
In view of progressive symptoms and inconclusive radiological findings, exploratory laparotomy was undertaken under general anaesthesia. Intraoperatively, a large cystic mass arising from the mesentery was identified, causing displacement of surrounding abdominal viscera and showing dense adhesions to the colon. Meticulous adhesiolysis was performed, and the mass was completely excised in toto without rupture. The resected specimen was sent for pathological examination.
Gross examination of the excised specimen revealed a partially encapsulated mass with an irregular external surface. On sectioning, the lesion demonstrated solid areas interspersed with cystic and mucin-filled spaces. Representative tissue sections were processed and stained with hematoxylin and eosin for microscopic evaluation. Histopathological analysis focused on epithelial architecture, papillary and glandular patterns, stromal invasion, nuclear atypia, mitotic activity, and mucin production. The microscopic findings were correlated with clinical, radiological, and intraoperative observations to establish the final diagnosis.
Ethical Considerations: Written informed consent for publication of this case report and accompanying images was obtained from the patient. Institutional ethical approval was not required for a single case report according to institutional policy.
3. Case Presentation
A 20-year-old female presented to the Surgery Outpatient Department of the Saraswathi Institute of Medical Sciences, Hapur, with complaints of abdominal distention, pain, nausea, vomiting, and constipation for two months, along with progressive shortness of breath for one month. Abdominal pain was gradual in onset, progressive, and non-radiating. On clinical examination, the patient was found to be anemic. Abdominal examination revealed a distended abdomen with a vague palpable mass occupying the entire abdomen, with variable consistency on palpation. Lump was non mobile.
Contrast-enhanced positron emission tomography–computed tomography revealed a large lobulated abdominopelvic soft tissue dense mass measuring approximately 24 × 18 × 15 cm, with internal septations and heterogeneous enhancement, displacing abdominal structures superiorly and contributing to abdominal distension. The uterus and adnexa were clear. The mass caused significant mass effect, including dilatation of the bilateral ureters proximally, bilateral renal pelvis dilatation, and left ureteric obstruction with secondary hydronephrosis.
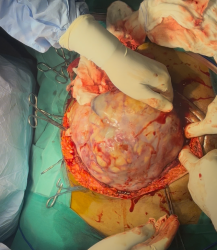
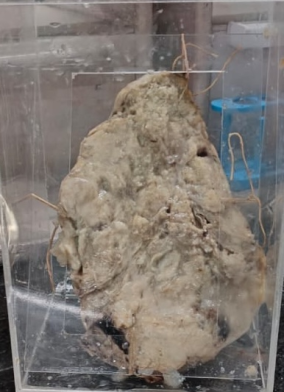
No definitive preoperative diagnosis can be established based on imaging and clinical examinations. Therefore, a surgical excision was performed. During laparotomy, a mass was identified that was fixed to the mesentery (Figure 1), displacing all the surrounding structures superiorly. Dense adhesion to the colon was also observed. As the lesion did not share a common blood supply with the adjacent structures, excision was performed. Adhesiolysis was performed and the mass was removed (Figure 2). The specimen was sent for histopathological examination.
Figure 1. Abdominal mass arising from the mesentery.
Postoperative Course and Outcome
The patient initially recovered from anesthesia and was hemodynamically stable. However, she developed sudden cardiac arrest in the immediate postoperative period and could not be revived despite resuscitative measures.
A large mass was identified on gross examination. The mass appeared partially encapsulated, with nodular, irregular, and glistening surfaces. Cut sections revealed solid areas, along with mucinous and cystic spaces (Figure 3).
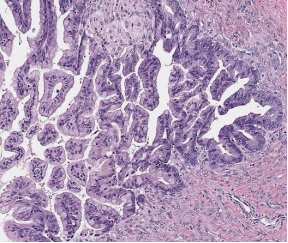
Microscopic examination of H&E-stained sections revealed atypical epithelial cells forming large cysts and complex glands arranged in papillary patterns, some irregular and fragmented, and invading stroma. The tumor cells resembled the intestinal epithelium, with intracellular mucin in some cells, extracellular mucin pools, goblet cells, and occasional signet-ring cells (Figure 4).
Cytological features include a high nuclear-to-cytoplasmic ratio, nuclear pleomorphism, hyperchromasia, irregular nuclear membranes, prominent nucleoli, and frequent mitotic activity. Mixed inflammatory infiltrates were also observed. The histopathological features were consistent with Papillary Mucinous Cystadenocarcinoma of Mesentery.
Primary cystadenocarcinoma of the mesentery is an exceptionally rare entity, with most knowledge derived from isolated case reports and small series
[1]
Metaxas, G., Tangalos, A., Pappa, P., Papageorgiou, I. Mucinous cystic neoplasms of the mesentery: A case report and review of the literature. World Journal of Surgical Oncology. 2009, 7, 47.
Sobnach, S., Singh, B., Satyapal, K. S., et al. Primary seromucinous cystadenocarcinoma of the mesentery. South African Journal of Surgery. 2016, 54(3), 44–45.
[7]
Jaiswal, R., Dubey, D. B., Singh, R., Mishra, A. Recurrent mucinous cystic neoplasm of the mesentery in a young nullipara mimicking ovarian carcinoma. Journal of Cancer Research and Therapeutics. 2024, 20, 454–456.
. These tumors share histological and immunohistochemical similarities with ovarian and pancreatic mucinous neoplasms, suggesting a common pathogenesis possibly related to coelomic metaplasia or Mullerian remnants.
Preoperative differentiation between benign, borderline, and malignant mesenteric cystic lesions remains difficult despite advances in CT, MRI, and PET-CT imaging. Recent reports suggest that increased FDG uptake on PET-CT may raise suspicion for malignancy
[3]
Hozaka, Y., Murakami, T., Kato, T., et al. Usefulness of 18F-FDG PET/CT in primary cystadenocarcinoma of the mesentery: A case report. Surgical Case Reports. 2020, 6, 306.
Hozaka, Y., Murakami, T., Kato, T., et al. Malignancy suspicion in mesenteric cystic tumors using PET/CT imaging. Surgical Case Reports. 2020, 6, 306.
[3, 6]
, However histopathology remains the gold standard. Complete surgical excision with intact cyst removal is crucial, as cyst rupture and incomplete resection are associated with recurrence and poorer outcomes
[4]
Sobnach, S., Singh, B., Satyapal, K. S., et al. Primary seromucinous cystadenocarcinoma of the mesentery. South African Journal of Surgery. 2016, 54(3), 44–45.
[7]
Jaiswal, R., Dubey, D. B., Singh, R., Mishra, A. Recurrent mucinous cystic neoplasm of the mesentery in a young nullipara mimicking ovarian carcinoma. Journal of Cancer Research and Therapeutics. 2024, 20, 454–456.
Sobnach, S., Singh, B., Satyapal, K. S., et al. Surgical excision as definitive treatment of mesenteric cystic malignancies. South African Journal of Surgery. 2016, 54(3), 44–45.
[4, 7, 8]
.
The role of adjuvant chemotherapy or radiotherapy is not clearly established due to the rarity of the condition, and long-term outcomes remain uncertain. Therefore, careful long-term follow-up is advised.
Table 1. Summarizes previously reported cases of primary mesenteric cystadenocarcinoma in comparison with the present case, highlighting patient demographics, tumor characteristics, management strategies, and outcomes.
Author (Year)
Age / Sex
Tumor Location
Tumor Size
Management
Adjuvant Therapy
Outcome / Follow-up
Metaxas et al. (2009)
35 F (median malignant cases)
Mesocolon / small bowel mesentery
Large (>10 cm in most cases)
Complete excision ± bowel resection
Not standardized
Variable; recurrence reported after incomplete excision
Obuchi et al. (2014)
41 M
Mesocolon
7.5 × 8.6 × 9.5 cm
Right hemicolectomy with cyst excision
None
Recurrence with peritoneal dissemination; deceased at 19 months
Cystadenocarcinoma of the mesentery, though extremely rare, should be considered in the differential diagnosis of large intra-abdominal cystic masses, particularly in young females. Definitive diagnosis relies on histopathological examination, and complete surgical excision remains the cornerstone of management
[3]
Hozaka, Y., Murakami, T., Kato, T., et al. Usefulness of 18F-FDG PET/CT in primary cystadenocarcinoma of the mesentery: A case report. Surgical Case Reports. 2020, 6, 306.
Jaiswal, R., Dubey, D. B., Singh, R., Mishra, A. Recurrent mucinous cystic neoplasm of the mesentery in a young nullipara mimicking ovarian carcinoma. Journal of Cancer Research and Therapeutics. 2024, 20, 454–456.
Yadavalli Sri Venkata Raviteja: Data curation, Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Metaxas, G., Tangalos, A., Pappa, P., Papageorgiou, I. Mucinous cystic neoplasms of the mesentery: A case report and review of the literature. World Journal of Surgical Oncology. 2009, 7, 47.
Hozaka, Y., Murakami, T., Kato, T., et al. Usefulness of 18F-FDG PET/CT in primary cystadenocarcinoma of the mesentery: A case report. Surgical Case Reports. 2020, 6, 306.
Sobnach, S., Singh, B., Satyapal, K. S., et al. Primary seromucinous cystadenocarcinoma of the mesentery. South African Journal of Surgery. 2016, 54(3), 44–45.
[5]
Obuchi, T., Sasaki, A., Wakabayashi, G., et al. Serous cystadenocarcinoma of the mesentery in a man: A case report and review of the literature. Gastroenterology Report. 2014, 2(4), 306–310.
Hozaka, Y., Murakami, T., Kato, T., et al. Malignancy suspicion in mesenteric cystic tumors using PET/CT imaging. Surgical Case Reports. 2020, 6, 306.
[7]
Jaiswal, R., Dubey, D. B., Singh, R., Mishra, A. Recurrent mucinous cystic neoplasm of the mesentery in a young nullipara mimicking ovarian carcinoma. Journal of Cancer Research and Therapeutics. 2024, 20, 454–456.
Sobnach, S., Singh, B., Satyapal, K. S., et al. Surgical excision as definitive treatment of mesenteric cystic malignancies. South African Journal of Surgery. 2016, 54(3), 44–45.
Majumdar, R. K., Raviteja, Y. S. V. (2026). Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management. Journal of Surgery, 14(2), 30-34. https://doi.org/10.11648/j.js.20261402.12
Majumdar, R. K.; Raviteja, Y. S. V. Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management. J. Surg.2026, 14(2), 30-34. doi: 10.11648/j.js.20261402.12
@article{10.11648/j.js.20261402.12,
author = {Rajib Kumar Majumdar and Yadavalli Sri Venkata Raviteja},
title = {Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management},
journal = {Journal of Surgery},
volume = {14},
number = {2},
pages = {30-34},
doi = {10.11648/j.js.20261402.12},
url = {https://doi.org/10.11648/j.js.20261402.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20261402.12},
abstract = {Primary cystadenocarcinoma of the mesentery is an extremely rare malignant cystic epithelial tumor and represents the malignant spectrum of mesenteric mucinous cystic neoplasms. Due to its rarity, fewer than 25 cases have been reported in the literature, and the clinical characteristics, diagnostic features, and optimal management strategies remain poorly defined. Patients usually present with nonspecific symptoms related to mass effect, including abdominal pain, abdominal distension, nausea, vomiting, constipation, or a palpable abdominal mass, often mimicking ovarian or gastrointestinal tumors. Preoperative diagnosis is particularly challenging because radiological findings are not pathognomonic and tumor markers have limited diagnostic value. We report a rare case of primary mesenteric cystadenocarcinoma in a 20-year-old female who presented with progressive abdominal distension, abdominal pain, nausea, vomiting, constipation, and exertional shortness of breath. Clinical examination revealed a large abdominal mass. Contrast-enhanced positron emission tomography–computed tomography demonstrated a large lobulated abdominopelvic mass with internal septations and heterogeneous enhancement, producing significant mass effect including bilateral ureteric dilatation and hydronephrosis. However, the exact origin of the lesion could not be determined preoperatively. Exploratory laparotomy revealed a large cystic mass arising from the mesentery with dense adhesions to the colon. Complete surgical excision was performed without rupture. Histopathological examination confirmed papillary mucinous cystadenocarcinoma of mesenteric origin. This case highlights the diagnostic difficulty associated with mesenteric cystic malignancies and emphasizes that complete surgical excision remains essential for definitive diagnosis and management.},
year = {2026}
}
TY - JOUR
T1 - Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management
AU - Rajib Kumar Majumdar
AU - Yadavalli Sri Venkata Raviteja
Y1 - 2026/03/17
PY - 2026
N1 - https://doi.org/10.11648/j.js.20261402.12
DO - 10.11648/j.js.20261402.12
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 30
EP - 34
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20261402.12
AB - Primary cystadenocarcinoma of the mesentery is an extremely rare malignant cystic epithelial tumor and represents the malignant spectrum of mesenteric mucinous cystic neoplasms. Due to its rarity, fewer than 25 cases have been reported in the literature, and the clinical characteristics, diagnostic features, and optimal management strategies remain poorly defined. Patients usually present with nonspecific symptoms related to mass effect, including abdominal pain, abdominal distension, nausea, vomiting, constipation, or a palpable abdominal mass, often mimicking ovarian or gastrointestinal tumors. Preoperative diagnosis is particularly challenging because radiological findings are not pathognomonic and tumor markers have limited diagnostic value. We report a rare case of primary mesenteric cystadenocarcinoma in a 20-year-old female who presented with progressive abdominal distension, abdominal pain, nausea, vomiting, constipation, and exertional shortness of breath. Clinical examination revealed a large abdominal mass. Contrast-enhanced positron emission tomography–computed tomography demonstrated a large lobulated abdominopelvic mass with internal septations and heterogeneous enhancement, producing significant mass effect including bilateral ureteric dilatation and hydronephrosis. However, the exact origin of the lesion could not be determined preoperatively. Exploratory laparotomy revealed a large cystic mass arising from the mesentery with dense adhesions to the colon. Complete surgical excision was performed without rupture. Histopathological examination confirmed papillary mucinous cystadenocarcinoma of mesenteric origin. This case highlights the diagnostic difficulty associated with mesenteric cystic malignancies and emphasizes that complete surgical excision remains essential for definitive diagnosis and management.
VL - 14
IS - 2
ER -
Majumdar, R. K., Raviteja, Y. S. V. (2026). Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management. Journal of Surgery, 14(2), 30-34. https://doi.org/10.11648/j.js.20261402.12
Majumdar, R. K.; Raviteja, Y. S. V. Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management. J. Surg.2026, 14(2), 30-34. doi: 10.11648/j.js.20261402.12
@article{10.11648/j.js.20261402.12,
author = {Rajib Kumar Majumdar and Yadavalli Sri Venkata Raviteja},
title = {Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management},
journal = {Journal of Surgery},
volume = {14},
number = {2},
pages = {30-34},
doi = {10.11648/j.js.20261402.12},
url = {https://doi.org/10.11648/j.js.20261402.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20261402.12},
abstract = {Primary cystadenocarcinoma of the mesentery is an extremely rare malignant cystic epithelial tumor and represents the malignant spectrum of mesenteric mucinous cystic neoplasms. Due to its rarity, fewer than 25 cases have been reported in the literature, and the clinical characteristics, diagnostic features, and optimal management strategies remain poorly defined. Patients usually present with nonspecific symptoms related to mass effect, including abdominal pain, abdominal distension, nausea, vomiting, constipation, or a palpable abdominal mass, often mimicking ovarian or gastrointestinal tumors. Preoperative diagnosis is particularly challenging because radiological findings are not pathognomonic and tumor markers have limited diagnostic value. We report a rare case of primary mesenteric cystadenocarcinoma in a 20-year-old female who presented with progressive abdominal distension, abdominal pain, nausea, vomiting, constipation, and exertional shortness of breath. Clinical examination revealed a large abdominal mass. Contrast-enhanced positron emission tomography–computed tomography demonstrated a large lobulated abdominopelvic mass with internal septations and heterogeneous enhancement, producing significant mass effect including bilateral ureteric dilatation and hydronephrosis. However, the exact origin of the lesion could not be determined preoperatively. Exploratory laparotomy revealed a large cystic mass arising from the mesentery with dense adhesions to the colon. Complete surgical excision was performed without rupture. Histopathological examination confirmed papillary mucinous cystadenocarcinoma of mesenteric origin. This case highlights the diagnostic difficulty associated with mesenteric cystic malignancies and emphasizes that complete surgical excision remains essential for definitive diagnosis and management.},
year = {2026}
}
TY - JOUR
T1 - Rare Presentation of a Primary Mesenteric Cystadenocarcinoma: Surgical Management
AU - Rajib Kumar Majumdar
AU - Yadavalli Sri Venkata Raviteja
Y1 - 2026/03/17
PY - 2026
N1 - https://doi.org/10.11648/j.js.20261402.12
DO - 10.11648/j.js.20261402.12
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 30
EP - 34
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20261402.12
AB - Primary cystadenocarcinoma of the mesentery is an extremely rare malignant cystic epithelial tumor and represents the malignant spectrum of mesenteric mucinous cystic neoplasms. Due to its rarity, fewer than 25 cases have been reported in the literature, and the clinical characteristics, diagnostic features, and optimal management strategies remain poorly defined. Patients usually present with nonspecific symptoms related to mass effect, including abdominal pain, abdominal distension, nausea, vomiting, constipation, or a palpable abdominal mass, often mimicking ovarian or gastrointestinal tumors. Preoperative diagnosis is particularly challenging because radiological findings are not pathognomonic and tumor markers have limited diagnostic value. We report a rare case of primary mesenteric cystadenocarcinoma in a 20-year-old female who presented with progressive abdominal distension, abdominal pain, nausea, vomiting, constipation, and exertional shortness of breath. Clinical examination revealed a large abdominal mass. Contrast-enhanced positron emission tomography–computed tomography demonstrated a large lobulated abdominopelvic mass with internal septations and heterogeneous enhancement, producing significant mass effect including bilateral ureteric dilatation and hydronephrosis. However, the exact origin of the lesion could not be determined preoperatively. Exploratory laparotomy revealed a large cystic mass arising from the mesentery with dense adhesions to the colon. Complete surgical excision was performed without rupture. Histopathological examination confirmed papillary mucinous cystadenocarcinoma of mesenteric origin. This case highlights the diagnostic difficulty associated with mesenteric cystic malignancies and emphasizes that complete surgical excision remains essential for definitive diagnosis and management.
VL - 14
IS - 2
ER -