Background: Breast cancer has remained as a major cause of death and a growing public health challenge in developing countries. Nevertheless, there is a paucity of research evidence on breast cancer patients’ presentation and contributing factors for the delay in Eastern Ethiopia. Hence, this study aimed to assess delay in presentation and contributing factors among patients with breast cancer who visited Oncology Unit at tertiary Hospital in Harar, Eastern Ethiopia. Methods: An institution-based cross-sectional study was conducted with newly diagnosed breast cancer patients at the Oncology Units of Hiwot-Fana Comprehensive Specialized University Hospital from January 2022 to June 2023. Data were collected from July 5 to October 30, 2023, using a structured tool, and entered into SPSS version 26 for cleaning and analysis. Descriptive statistics were applied to compute the socio-demographic and clinical characteristics of the patients. Logistic regression was carried out to examine factors associated with patient delay in presentation. AOR at a 95% confidence interval and P-value <0.05 was used to declare a significant association. Results: From the total of 206 patients included in the study, 98.5% of them were females and 1.5% were males with the median age of 43 years. Three-fourth (76.7%) of the study participants were presented after 3 months of experiencing sign and symptoms which ranged from 3-15 months and a median time of presentation was 6 months. Of these, 84% of the patients diagnosed advanced-stage breast cancer. among Being residents of rural setting of Ethiopia (AOR=7.63; 95% CI=1.97-29.44), being illiterate (AOR=5.23; 95% CI=1.05-26.18), having a painless lump (AOR=6.83; 95% CI=1.85-25.14), travel distance ≥5 km from the Hospital (AOR=4.08; 95% CI=1.06-15.78), and having history of traditional medicine use (AOR=4.53; 95% CI=1.02-20.22) were the factors contributing to delayed presentation to the Oncology Unit or Hospital. Patients who have ever heard of breast cancer were less likely to delay in presentation (AOR=0.13; 95% CI=0.04-0.44). Conclusion: Breast cancer patients delayed presentation was found to be common in Eastern Ethiopia. Patients lived in rural area, illiterate, having a painless lump, far distance form health facility, have not ever heard about breast cancer, and relay on traditional medicine were associated with delays in presentation. Therefore, concerned stakeholders should strengthen awareness creation to minimize the dalliance of the patients in seeking health care.
| Published in | Medicine and Life Sciences (Volume 2, Issue 1) |
| DOI | 10.11648/j.mls.20260201.12 |
| Page(s) | 10-22 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Breast Cancer, Patient Delay, Contributing Factors, Harar, Ethiopia
Variable | Categories | n | % |
|---|---|---|---|
Age (year) | <40 | 68 | 33 |
≥40 | 138 | 67 | |
Sex | Female | 203 | 98.5 |
Male | 3 | 1.5 | |
Religion | Orthodox | 69 | 33.5 |
Muslim | 106 | 51.5 | |
Protestant | 23 | 11.2 | |
Catholic | 7 | 3.4 | |
Others ⃰ | 1 | 0.5 | |
Marital status | Married | 183 | 88.8 |
Single | 11 | 5.3 | |
Divorced | 5 | 2.4 | |
Widowed | 7 | 3.4 | |
Residence | Urban | 62 | 30.1 |
Rural | 144 | 69.9 | |
Region | Harari | 35 | 17.0 |
Oromiya | 85 | 41.3 | |
Dire Dawa | 64 | 31.1 | |
Somalia | 22 | 10.7 | |
Educational status | Illiterate | 122 | 59.2 |
Able to read & write | 25 | 12.1 | |
Primary education completed | 25 | 12.1 | |
Secondary education completed | 9 | 4.4 | |
Tertiary and above | 25 | 12.1 | |
Occupation | Housewife | 73 | 35.4 |
Private employee | 56 | 27.2 | |
Government employee | 36 | 17.5 | |
Farmer | 38 | 18.4 | |
Other ⃰ ⃰ | 3 | 1.5 | |
Distance to nearby a health facility | <5 km | 103 | 50.0 |
≥5 km | 103 | 50.0 |
Variable Category | n | % | |
|---|---|---|---|
Menopausal status (n=203) | Premenopausal | 117 | 57.6 |
Post-menopausal | 86 | 42.4 | |
Have given birth (n=203) | Yes | 168 | 82.8 |
No | 35 | 17.2 | |
Contraceptive use (n=203) | Yes | 85 | 41.9 |
No | 118 | 58.1 | |
Pregnancy (n=203) | Yes | 3 | 1.5 |
No | 200 | 98.5 | |
Family history of any type of cancer | Yes | 6 | 2.9 |
No | 200 | 97.1 | |
Family history of breast cancer | Yes | 5 | 2.4 |
No | 201 | 97.6 | |
Smoking | Yes | 9 | 4.4 |
No | 197 | 95.6 | |
Alcohol use | Yes | 7 | 3.4 |
No | 199 | 96.6 | |
Traditional treatment use | Yes | 65 | 31.6 |
No | 141 | 68.4 | |
Ever heard of breast cancer | Yes | 75 | 36.4 |
No | 131 | 63.6 | |
Any breast problem before | Yes | 13 | 6.3 |
No | 193 | 93.7 | |
Variables | Category | n | % |
|---|---|---|---|
Comorbidities | Yes | 36 | 17.5 |
No | 170 | 82.5 | |
Type of comorbidity | Hypertension | 22 | 10.7 |
Diabetes Mellitus | 10 | 4.9 | |
Asthma | 2 | 1.0 | |
Heart disease | 3 | 1.5 | |
HIV | 6 | 2.9 | |
Presenting chief complaint | Painful breast | 27 | 13.1 |
Painless Breast lump | 159 | 77.2 | |
Dimpling/skin change | 21 | 10.2 | |
Nipple discharge | 18 | 8.7 | |
Lump in armpit | 19 | 9.2 | |
Breast self-examination (n=203) | Yes | 12 | 5.9 |
No | 191 | 94.1 | |
Clinical breast examination (n=203) | Yes | 12 | 5.9 |
No | 191 | 94.1 | |
Screening mammography, (n=203) | Yes | 9 | 4.4 |
No | 194 | 95.6 | |
Method of detection of symptoms | Accidentally | 194 | 94.2 |
During breastfeeding | 4 | 1.9 | |
During Breast self-examination | 6 | 2.9 | |
Other ⃰ | 2 | 1.0 | |
Duration of presenting complaint | <3 month | 48 | 23.3 |
≥3 month | 158 | 76.7 | |
Patient’s reason for the late presentation | Lack of awareness about early symptoms | 182 | 88.3 |
Relating symptoms with other medical problems | 155 | 75.2 | |
Belief that breast cancer has no medical treatment | 6 | 2.9 | |
Use of traditional and spiritual treatment options | 65 | 31.6 | |
Financial problems | 116 | 56.3 | |
Fear of surgery (loss of breast) | 15 | 7.3 |
Characteristics | Categories | n | % |
|---|---|---|---|
Histologic differentiation of tumor | Non-invasive carcinoma | 11 | 5.3 |
Invasive carcinoma | 195 | 94.7 | |
Axillary lymph node status | Positive | 179 | 86.9 |
Negative | 27 | 13.1 | |
Site of tumor | Right | 93 | 45.1 |
Left | 110 | 53.4 | |
Bilateral | 3 | 1.5 | |
Metastasis to other body site | Yes | 48 | 23.3 |
No | 158 | 76.7 | |
Type of tumor | Ductal | 185 | 89.8 |
Lobular | 11 | 5.3 | |
Other⃰ | 10 | 4.9 | |
Tumor size (in cm) | <5cm | 48 | 23.3 |
≥5cm | 158 | 76.7 | |
Tumor grade | Grade I | 43 | 20.9 |
Grade II | 58 | 28.2 | |
Grade III | 60 | 29.1 | |
Unknown | 45 | 21.8 | |
Treatment started | Yes | 190 | 92.2 |
No | 16 | 7.8 | |
Type of treatment given | Surgery alone | 9 | 4.4 |
Chemotherapy alone | 72 | 35.0 | |
Combination ⃰ ⃰ & Hormonal therapy | 24 | 11.7 | |
Combination & other ⃰⃰⃰⃰ ⃰ ⃰ | 3 | 1.5 |
Characteristics | Patient delay | COR (95% CI) | AOR (95% CI) | P value | |
|---|---|---|---|---|---|
≥3 Months | <3 Months | ||||
Residence | |||||
Urban | 42 (67.7%) | 20 (32.3%) | 1 | 1 | 0.003⃰ |
Rural | 116 (80.6%) | 28 (19.4%) | 1.97 (1.06-3.87) | 7.63 (1.97-29.44) | |
Distance from home to health facility | |||||
<5km | 62 (60.2%) | 41 (39.8%) | 1 | 1 | 0.041⃰ |
≥5km | 96 (93.2%) | 7 (6.8%) | 9.06 (3.82-21.49) | 4.08 (1.06-15.78) | |
Educational status | |||||
Illiterate | 113 (92.6%) | 9 (7.4%) | 7.06 (2.4- 20.4) | 5.23 (1.05-26.18) | 0.044⃰ |
Able to read & write | 13 (52%) | 12 (48%) | 0.60 (0.19-1.89) | 0.44 (0.08-2.29) | 0.328 |
Primary education completed | 13 (52%) | 12 (48%) | 0.60 (0.19-1.89) | 0.53 (0.09-3.16) | 0.483 |
Secondary education completed | 3 (33.3%) | 6 (66.7%) | 0.28 (0.05-1.45) | 0.34 (0.04-3.28) | 0.354 |
Tertiary and above | 16 (64%) | 9 (36%) | 1 | 1 | 1 |
Use of traditional treatment options | |||||
Yes | 61 (93.8%) | 4 (6.2%) | 6.91 (2.36-20.21) | 4.53 (1.02-20.22) | 0.048⃰ |
No | 97 (68.8%) | 44 (31.2%) | 1 | 1 | |
Ever heard of breast cancer | |||||
Yes | 38 (50.6%) | 37 (48.4%) | 0.094 (0.04-0.20) | 0.13 (0.04-0.44) | 0.001⃰ |
No | 120 (91.6%) | 11 (8.4%) | 1 | 1 | |
Swelling in the axilla/armpit | |||||
Yes | 11 (57.9%) | 8 (42.1%) | 0.374 (0.14-0.99) | 1.65 (0.26-10.54) | 0.597 |
No | 147 (78.6%) | 40 (21.4%) | 1 | 1 | |
Painless breast lump | |||||
Yes | 139 (87.4%) | 20 (12.6%) | 10 (4.84-21.63) | 6.83 (1.85-25.14) | 0.004⃰ |
No | 19 (40.4%) | 28 (59.6%) | 1 | 1 | |
Dimpling in the Breast | |||||
Yes | 8 (30%) | 13 (62%) | 0.14 (0.05-0.37) | 0.18 (0.03-1.14) | 0.068 |
No | 150 (81%) | 35 (19%) | 1 | 1 | |
Size of the mass (cm) | |||||
<5 cm | 30 (62.5%) | 18 (37.5%) | 1 | 1 | 0.181 |
≥5 cm | 128 (81%) | 30 (19%) | 2.56 (1.26-5.19) | 2.20 (0.69-7.01) | |
AOR | Adjusted Odds Ratio |
AJCC | American Joint Committee for Cancer |
CI | Confidence Interval |
COR | Crude Odds Ratio |
IQR | Interquartile Range |
LMICs | Low- and Middle-Income Countries |
SPSS | Statistical Package for Social Sciences |
WHO | World Health Organization |
| [1] | A. Tesfaw, S. Demis, T. Munye, and Z. Ashuro, “Patient delay and contributing factors among breast cancer patients at two cancer referral centres in Ethiopia: A cross-sectional study,” J Multidiscip Healthc, vol. 13, pp. 1391–1401, 2020, |
| [2] | N. H. Khan, S. F. Duan, D. D. Wu, and X. Y. Ji, “Better reporting and awareness campaigns needed for breast cancer in Pakistani women,” Cancer Manag Res, vol. 13, pp. 2125–2129, 2021, |
| [3] | H. Sung et al., “Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA Cancer J Clin, vol. 71, no. 3, pp. 209–249, May 2021, |
| [4] | S. O. Azubuike, C. Muirhead, L. Hayes, and R. McNally, “Rising global burden of breast cancer: The case of sub-Saharan Africa (with emphasis on Nigeria) and implications for regional development: A review,” Mar. 22, 2018, BioMed Central Ltd. |
| [5] | S. T. Memirie et al., “Estimates of Cancer Incidence in Ethiopia in 2015 Using Population-Based Registry Data,” J Glob Oncol, no. 4, pp. 1–11, Dec. 2018, |
| [6] | A. F. Awedew, Z. Asefa, and W. B. Belay, “National Burden and Trend of Cancer in Ethiopia, 2010-2019: a systemic analysis for Global burden of disease study,” Sci Rep, vol. 12, no. 1, p. 12736, Jul. 2022, |
| [7] | H. Zhang, G. Wang, J. Zhang, Y. Lu, and X. Jiang, “Patient delay and associated factors among Chinese women with breast cancer: A cross-sectional study.,” Medicine, vol. 98, no. 40, p. e17454, Oct. 2019, |
| [8] | E. Jedy-Agba, V. McCormack, C. Adebamowo, and I. dos-Santos-Silva, “Stage at diagnosis of breast cancer in sub-Saharan Africa: a systematic review and meta-analysis,” Lancet Glob Health, vol. 4, no. 12, pp. e923–e935, Dec. 2016, |
| [9] | A. Shita et al., “Survival and predictors of breast cancer mortality in South Ethiopia: A retrospective cohort study,” PLoS One, vol. 18, no. 3 March, Mar. 2023, |
| [10] | I. C. Umoke and E. S. Garba, “Breast cancer in North-Central Nigeria: challenges to good management outcome,” International Surgery Journal, vol. 6, no. 9, p. 3105, Aug. 2019, |
| [11] | O. S. Agodirin et al., “Prevalence of Themes Linked to Delayed Presentation of Breast Cancer in Africa: A Meta-Analysis of Patient-Reported Studies,” JCO Glob Oncol, no. 6, pp. 731–742, Nov. 2020, |
| [12] | L. E. Pace et al., “Impact of Breast Cancer Early Detection Training on Rwandan Health Workers’ Knowledge and Skills,” J Glob Oncol, no. 4, pp. 1–10, Dec. 2018, |
| [13] | S. Rayne, K. Schnippel, S. Grover, D. Kruger, C. Benn, and C. Firnhaber, “The effect of beliefs about breast cancer on stage and delay to presentation: results from a prospective study in urban South Africa,” South African Journal of Surgery, pp. 12–18, 2019, |
| [14] | A. Donkor et al., “Factors Contributing to Late Presentation of Breast Cancer in Africa: A Systematic Literature Review.” Available: |
| [15] | B. O. Anderson et al., “Optimisation of breast cancer management in low-resource and middle-resource countries: executive summary of the Breast Health Global Initiative consensus, 2010,” Lancet Oncol, vol. 12, no. 4, pp. 387–398, Apr. 2011, |
| [16] | S. C. Hiom, “Diagnosing cancer earlier: reviewing the evidence for improving cancer survival,” Br J Cancer, vol. 112, no. S1, pp. S1–S5, Mar. 2015, |
| [17] | C. Espina, F. McKenzie, and I. Dos-Santos-Silva, “Delayed presentation and diagnosis of breast cancer in African women: a systematic review.,” Ann Epidemiol, vol. 27, no. 10, pp. 659-671. e7, Oct. 2017, |
| [18] | D. Petrova et al., “Duration of the patient interval in breast cancer and factors associated with longer delays in low‐and middle‐income countries: A systematic review with meta‐analysis,” Psychooncology, vol. 32, no. 1, pp. 13–24, Jan. 2023, |
| [19] | F. Dandena Guyassa, T. Dana Darebo, and Y. Suga, “Epidemiology And Clinical Characteristics of Breast Cancer in Ethiopia: A Systematic Review”, |
| [20] | T. Bedada, H. A. Teshale, A. Hailu, and T. Mulugeta, “Prevalence and Factors Contributing to Late Diagnosis of Breast Cancer among Women Attending Tikur Anbessa Specialized Hospital, Oncology Unit, Addis Ababa, Ethiopia, 2017,” J Integr Oncol, vol. 07, no. 03, 2018, |
| [21] | M. Yoseph, A. Gebresadik, and A. Alemayehu, “Late Diagnosis of Breast Cancer and Associated Factors Among Women Attending Hawassa University Comprehensive and Specialized Hospital Southern Ethiopia,” 2021, |
| [22] | A. Gebremariam et al., “Time intervals experienced between first symptom recognition and pathologic diagnosis of breast cancer in Addis Ababa, Ethiopia: a cross-sectional study,” BMJ Open, vol. 9, no. 11, p. e032228, Nov. 2019, |
| [23] | A. M. Hassen, F. M. Hussien, Z. A. Asfaw, and H. E. Assen, “Factors Associated with Delay in Breast Cancer Presentation at the Only Oncology Center in North East Ethiopia: A Cross-Sectional Study,” J Multidiscip Healthc, vol. Volume 14, pp. 681–694, Mar. 2021, |
| [24] | S. B. Edge and C. C. Compton, “The American Joint Committee on Cancer: the 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM,” Ann Surg Oncol, vol. 17, no. 6, pp. 1471–1474, Jun. 2010, |
| [25] | E. Jedy-Agba et al., “Determinants of stage at diagnosis of breast cancer in Nigerian women: sociodemographic, breast cancer awareness, health care access and clinical factors,” Cancer Causes & Control, vol. 28, no. 7, pp. 685–697, Jul. 2017, |
| [26] | D. Weller et al., “The Aarhus statement: Improving design and reporting of studies on early cancer diagnosis,” Mar. 27, 2012. |
| [27] | Z. Bursac, C. H. Gauss, D. K. Williams, and D. W. Hosmer, “Purposeful selection of variables in logistic regression,” Source Code Biol Med, vol. 3, no. 1, p. 17, Dec. 2008, |
| [28] | M. A. Khan, S. Hanif, S. Iqbal, M. F. Shahzad, S. Shafique, and M. T. Khan, “Presentation delay in breast cancer patients and its association with sociodemographic factors in North Pakistan,” Chinese Journal of Cancer Research, vol. 27, no. 3, pp. 288–293, 2015, |
| [29] | M. Gueye et al., “Sociodemographic Factors Associated with Delays in Breast Cancer,” Open J Obstet Gynecol, vol. 07, no. 04, pp. 455–463, 2017, |
| [30] | J. B. Mabula et al., “Stage at diagnosis, clinicopathological and treatment patterns of breast cancer at Bugando Medical Centre in north-western Tanzania.,” Tanzan J Health Res, vol. 14, no. 4, pp. 269–79, Oct. 2012. |
| [31] | A. Tesfaw, W. Alebachew, and M. Tiruneh, “Why women with breast cancer presented late to health care facility in North-west Ethiopia? A qualitative study,” PLoS One, vol. 15, no. 12 December, Dec. 2020, |
| [32] | M. Joffe et al., “Barriers to early presentation of breast cancer among women in Soweto, South Africa,” PLoS One, vol. 13, no. 2, p. e0192071, Feb. 2018, |
| [33] | B. Benbakhta, M. Tazi, N. Benjaafar, A. Khattabi, and A. Maaroufi, “Determinants of patient and health system delays for women with breast cancer in Morocco, 2013,” Review of Epidemiology and Public Health, vol. 63, no. 3, pp. 191–201, Jun. 2015, |
| [34] | S. M. Mousa, I. A. Seifeldin, A. Hablas, E. S. Elbana, and A. S. Soliman, “Patterns of seeking medical care among Egyptian breast cancer patients: Relationship to late-stage presentation,” The Breast, vol. 20, no. 6, pp. 555–561, Dec. 2011, |
| [35] | L. E. Pace et al., “Delays in Breast Cancer Presentation and Diagnosis at Two Rural Cancer Referral Centers in Rwanda,” Oncologist, vol. 20, no. 7, pp. 780–788, Jul. 2015, |
| [36] | E. Ermiah, F. Abdalla, A. Buhmeida, E. Larbesh, S. Pyrhönen, and Y. Collan, “Diagnosis delay in Libyan female breast cancer,” BMC Res Notes, vol. 5, no. 1, p. 452, Dec. 2012, |
| [37] | N. F. Bussa, “Comparative Assessment of Traditional Medicine Utilizations in Three Adjacent Districts of East Hararghe, Ethiopia,” Journal of Ayurvedic and Herbal Medicine, vol. 7, no. 3, pp. 165–175, Sep. 2021, |
APA Style
Atalele, M. A., Assefa, A., Mohammedsani, B., Amentie, E., Semahegn, A. (2026). Delayed Presentation to the Hospital and Its Contributing Factors Among Patients with Breast Cancer in Harar, Eastern Ethiopia: A Facility-based Cross-sectional Study. Medicine and Life Sciences, 2(1), 10-22. https://doi.org/10.11648/j.mls.20260201.12
ACS Style
Atalele, M. A.; Assefa, A.; Mohammedsani, B.; Amentie, E.; Semahegn, A. Delayed Presentation to the Hospital and Its Contributing Factors Among Patients with Breast Cancer in Harar, Eastern Ethiopia: A Facility-based Cross-sectional Study. Med. Life Sci. 2026, 2(1), 10-22. doi: 10.11648/j.mls.20260201.12
AMA Style
Atalele MA, Assefa A, Mohammedsani B, Amentie E, Semahegn A. Delayed Presentation to the Hospital and Its Contributing Factors Among Patients with Breast Cancer in Harar, Eastern Ethiopia: A Facility-based Cross-sectional Study. Med Life Sci. 2026;2(1):10-22. doi: 10.11648/j.mls.20260201.12
@article{10.11648/j.mls.20260201.12,
author = {Mezgebu Abiye Atalele and Askual Assefa and Burka Mohammedsani and Eyobel Amentie and Agumasie Semahegn},
title = {Delayed Presentation to the Hospital and Its Contributing Factors Among Patients with Breast Cancer in Harar, Eastern Ethiopia: A Facility-based Cross-sectional Study},
journal = {Medicine and Life Sciences},
volume = {2},
number = {1},
pages = {10-22},
doi = {10.11648/j.mls.20260201.12},
url = {https://doi.org/10.11648/j.mls.20260201.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.mls.20260201.12},
abstract = {Background: Breast cancer has remained as a major cause of death and a growing public health challenge in developing countries. Nevertheless, there is a paucity of research evidence on breast cancer patients’ presentation and contributing factors for the delay in Eastern Ethiopia. Hence, this study aimed to assess delay in presentation and contributing factors among patients with breast cancer who visited Oncology Unit at tertiary Hospital in Harar, Eastern Ethiopia. Methods: An institution-based cross-sectional study was conducted with newly diagnosed breast cancer patients at the Oncology Units of Hiwot-Fana Comprehensive Specialized University Hospital from January 2022 to June 2023. Data were collected from July 5 to October 30, 2023, using a structured tool, and entered into SPSS version 26 for cleaning and analysis. Descriptive statistics were applied to compute the socio-demographic and clinical characteristics of the patients. Logistic regression was carried out to examine factors associated with patient delay in presentation. AOR at a 95% confidence interval and P-value <0.05 was used to declare a significant association. Results: From the total of 206 patients included in the study, 98.5% of them were females and 1.5% were males with the median age of 43 years. Three-fourth (76.7%) of the study participants were presented after 3 months of experiencing sign and symptoms which ranged from 3-15 months and a median time of presentation was 6 months. Of these, 84% of the patients diagnosed advanced-stage breast cancer. among Being residents of rural setting of Ethiopia (AOR=7.63; 95% CI=1.97-29.44), being illiterate (AOR=5.23; 95% CI=1.05-26.18), having a painless lump (AOR=6.83; 95% CI=1.85-25.14), travel distance ≥5 km from the Hospital (AOR=4.08; 95% CI=1.06-15.78), and having history of traditional medicine use (AOR=4.53; 95% CI=1.02-20.22) were the factors contributing to delayed presentation to the Oncology Unit or Hospital. Patients who have ever heard of breast cancer were less likely to delay in presentation (AOR=0.13; 95% CI=0.04-0.44). Conclusion: Breast cancer patients delayed presentation was found to be common in Eastern Ethiopia. Patients lived in rural area, illiterate, having a painless lump, far distance form health facility, have not ever heard about breast cancer, and relay on traditional medicine were associated with delays in presentation. Therefore, concerned stakeholders should strengthen awareness creation to minimize the dalliance of the patients in seeking health care.},
year = {2026}
}
TY - JOUR T1 - Delayed Presentation to the Hospital and Its Contributing Factors Among Patients with Breast Cancer in Harar, Eastern Ethiopia: A Facility-based Cross-sectional Study AU - Mezgebu Abiye Atalele AU - Askual Assefa AU - Burka Mohammedsani AU - Eyobel Amentie AU - Agumasie Semahegn Y1 - 2026/01/19 PY - 2026 N1 - https://doi.org/10.11648/j.mls.20260201.12 DO - 10.11648/j.mls.20260201.12 T2 - Medicine and Life Sciences JF - Medicine and Life Sciences JO - Medicine and Life Sciences SP - 10 EP - 22 PB - Science Publishing Group UR - https://doi.org/10.11648/j.mls.20260201.12 AB - Background: Breast cancer has remained as a major cause of death and a growing public health challenge in developing countries. Nevertheless, there is a paucity of research evidence on breast cancer patients’ presentation and contributing factors for the delay in Eastern Ethiopia. Hence, this study aimed to assess delay in presentation and contributing factors among patients with breast cancer who visited Oncology Unit at tertiary Hospital in Harar, Eastern Ethiopia. Methods: An institution-based cross-sectional study was conducted with newly diagnosed breast cancer patients at the Oncology Units of Hiwot-Fana Comprehensive Specialized University Hospital from January 2022 to June 2023. Data were collected from July 5 to October 30, 2023, using a structured tool, and entered into SPSS version 26 for cleaning and analysis. Descriptive statistics were applied to compute the socio-demographic and clinical characteristics of the patients. Logistic regression was carried out to examine factors associated with patient delay in presentation. AOR at a 95% confidence interval and P-value <0.05 was used to declare a significant association. Results: From the total of 206 patients included in the study, 98.5% of them were females and 1.5% were males with the median age of 43 years. Three-fourth (76.7%) of the study participants were presented after 3 months of experiencing sign and symptoms which ranged from 3-15 months and a median time of presentation was 6 months. Of these, 84% of the patients diagnosed advanced-stage breast cancer. among Being residents of rural setting of Ethiopia (AOR=7.63; 95% CI=1.97-29.44), being illiterate (AOR=5.23; 95% CI=1.05-26.18), having a painless lump (AOR=6.83; 95% CI=1.85-25.14), travel distance ≥5 km from the Hospital (AOR=4.08; 95% CI=1.06-15.78), and having history of traditional medicine use (AOR=4.53; 95% CI=1.02-20.22) were the factors contributing to delayed presentation to the Oncology Unit or Hospital. Patients who have ever heard of breast cancer were less likely to delay in presentation (AOR=0.13; 95% CI=0.04-0.44). Conclusion: Breast cancer patients delayed presentation was found to be common in Eastern Ethiopia. Patients lived in rural area, illiterate, having a painless lump, far distance form health facility, have not ever heard about breast cancer, and relay on traditional medicine were associated with delays in presentation. Therefore, concerned stakeholders should strengthen awareness creation to minimize the dalliance of the patients in seeking health care. VL - 2 IS - 1 ER -
School of Medicine and Health Sciences, Haramaya University, Harar, Ethiopia
School of Medicine and Health Sciences, Haramaya University, Harar, Ethiopia
School of Medicine and Health Sciences, Haramaya University, Harar, Ethiopia
School of Medicine and Health Sciences, Haramaya University, Harar, Ethiopia
School of Public Health, Haramaya University, Harar, Ethiopia;School of Public Health, University of Ghana, Accra, Ghana
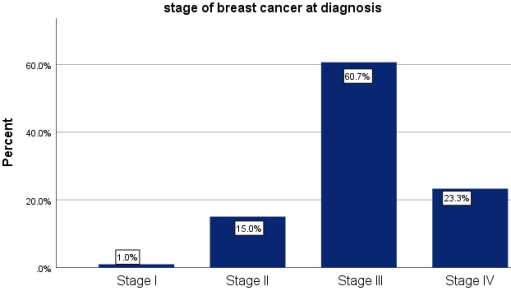
Figure 1. Stage at Diagnosis of Breast Cancer Patients in Hiwot Fana Specialized Hospital, 2023 (n=206).
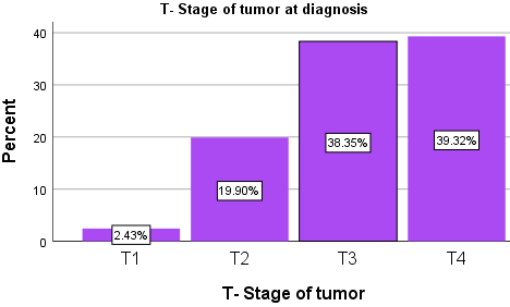
Figure 2. Tumor Size at Diagnosis of Breast Cancer Patients in Hiwot Fana Specialized Hospital, 2023.
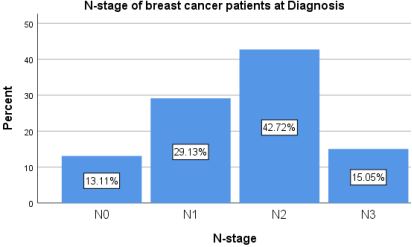
Figure 3. N (Lymph Node) Status at Diagnosis of Breast Cancer Patients in Hiwot Fana Specialized Hospital, 2023.
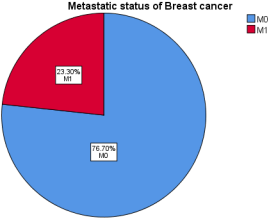
Figure 4. Metastatic Status at Diagnosis of Breast Cancer Patients in Hiwot Fana Specialized Hospital, 2023.
Information

