3. Literature Review
3.1. Global Overview
3.1.1. Prevalence of Child and Adolescent Mental Health Disorders
Global research shows that mental health conditions among children and adolescents are increasing, with an estimated one in seven young people affected each year
| [2] | WHO. (2022). World mental health report 2022: Transforming mental health for all. World Health Organization. |
[2]
. Depression, anxiety, and behavioural disorders remain the most common diagnoses, although many conditions go unrecognised due to limited awareness. Studies highlight that even in high-income countries, around 50% of child mental health cases do not receive treatment, reflecting gaps in screening and early intervention
| [6] | Patel, V., Saxena, S., & Lund, C. (2021). Adolescent mental health and global stressors: A cross-country analysis. Global Psychiatry Review, 12(2), 88–104. |
[6]
. These trends demonstrate that youth mental health challenges are widespread and not restricted to specific regions or socioeconomic groups.
3.1.2. School-related Stress and Academic Pressure
One consistent global finding is that school-related stress contributes significantly to youth mental health problems. International studies in Europe, Asia, and North America indicate rising anxiety linked to academic competition, continuous assessment, and high expectations from parents and teachers
| [7] | Anderson, R., & Cooper, L. (2022). Academic stress and wellbeing among adolescents: A global review. International Journal of School Health, 9(2), 45–59. |
[7]
. Exam pressure often leads to sleep disturbances, concentration problems, and emotional exhaustion. These stressors affect adolescents particularly, as they navigate identity formation and social expectations simultaneously. Though these patterns arise in different cultural contexts, they provide useful parallels for understanding pressures faced by learners in Zimbabwean schools.
3.1.3. Effects of Global Poverty and Social Inequality
In low- and middle-income countries, poverty is a dominant determinant of youth mental health
| [1] | UNICEF. (2023). Child and adolescent mental health in low-resource settings: A situational analysis. UNICEF Publications. |
[1]
. A UNICEF report notes that children living in poor households face chronic stress that undermines emotional stability, including irregular meals, unstable housing, and exposure to conflict. The cumulative effect of these stressors increases vulnerability to depression, anxiety, and behavioural problems. Global evidence suggests that children in impoverished communities often internalise family stress, especially when they witness guardians struggling to meet basic needs
| [8] | Kieling, C., Baker-Henningham, H., Belfer, M., & Erskine, H. (2021). Global child mental health: Evidence, challenges, and opportunities. The Lancet Global Health, 9(1), 32–40. |
[8]
. These patterns are essential for understanding mental health in rural and peri-urban settings like Bindura District.
3.1.4. Technology, Social Media, and Emerging Global Stressors
In the global context, social media has become a significant factor affecting child and adolescent mental health. Studies from the USA, South Korea, and the UK show that excessive screen time, cyberbullying, and comparison with peers online increase anxiety and negative self-image
| [6] | Patel, V., Saxena, S., & Lund, C. (2021). Adolescent mental health and global stressors: A cross-country analysis. Global Psychiatry Review, 12(2), 88–104. |
[6]
. Although internet penetration rates differ across countries, digital stressors are becoming more common even in African and Zimbabwean contexts as smartphone access expands.
3.1.5. Global Gaps in Early Detection and Access to Care
Globally, early detection remains one of the weakest points in child mental health systems.
| [2] | WHO. (2022). World mental health report 2022: Transforming mental health for all. World Health Organization. |
[2]
A WHO reports notes that most countries lack sufficient child psychologists and rely on general health workers who may not identify early signs of distress. Rural communities face additional barriers, including long distances to health services and lack of mental health literacy. These global patterns closely mirror challenges in Zimbabwe, where child-focused mental health support remains limited.
3.2. African and Regional Overview
3.2.1. Mental Health Trends Among African Children and Adolescents
Across Africa, research shows increasing rates of depression, anxiety, and emotional disorders among young people. A multi-country study in East Africa recorded a rise in psychological distress linked to school pressure, bullying, and community stressors
| [9] | Mboya, B., Otiende, T., & Muriuki, S. (2021). Adolescent mental health in East Africa: Emerging trends and concerns. East African Child Development Review, 3(1), 21–36. |
[9]
. Schools with limited resources, overcrowded classrooms, and strict disciplinary cultures have been shown to contribute to anxiety among learners. These findings resonate with Zimbabwean schools, particularly in districts like Bindura where guidance and counselling structures are often stretched.
3.2.2. School Stress, Bullying, and Academic Expectations in African Schools
Many African schooling systems place strong emphasis on examinations, which often creates high levels of anxiety among learners. In Kenya and Uganda, studies indicate that exam periods are associated with increased headaches, irritability, and physiological symptoms of stress
| [10] | Wamuyu, J., & Muriithi, F. (2021). Examination anxiety and academic pressure in East African secondary schools. African Research Journal of Education, 9(1), 27–39. |
[10]
. Bullying, both physical and verbal, remains a persistent issue in African schools, contributing significantly to emotional disorders and behavioural problems
| [11] | Simbayi, L., Zwane, N., & Khumalo, T. (2022). School bullying and emotional outcomes among South African learners. African Journal of Educational Development, 6(2), 43–59. |
[11]
. These dynamics are relevant for Bindura District, where school counsellors often report cases of stress linked to exam pressure and peer conflicts.
3.2.3. Impact of Socio-economic Adversity on African Youth
Poverty remains one of the most influential determinants of child mental health across Africa. Children living in unstable households or food-insecure environments are more likely to experience emotional distress and behavioural challenges
| [12] | Chilimampunga, C., Banda, F., & Zimba, G. (2022). Household poverty and youth emotional distress in rural Malawi. African Journal of Social Work, 12(4), 15–26. |
[12]
. When parents struggle financially, children may internalise guilt or fear, which increases anxiety symptoms. Economic insecurity also affects schooling, with learners in impoverished settings frequently missing classes due to lack of fees or materials, thereby increasing academic pressure once they return.
3.2.4. Cultural Beliefs, Stigma, and Mental Health in African Contexts
Cultural interpretations of mental illness play a powerful role in shaping help-seeking behaviour in Africa. Mental health symptoms are often attributed to spiritual or supernatural causes, leading families to rely on spiritual healers rather than medical professionals
| [13] | Ngoma, M., & Thwala, S. (2023). Stigma, beliefs, and help-seeking behaviour among African families experiencing mental illness. African Mental Health Review, 11(4), 60–72. |
[13]
. Stigma remains widespread, making it difficult for children to express emotional distress. Adolescents may feel pressure to “be strong” or hide emotional challenges, which delays treatment and worsens outcomes. This cultural silence is similar to patterns observed in Zimbabwe.
3.2.5. Trauma, Violence, and Community Instability
Exposure to trauma, whether from domestic violence, corporal punishment, or community conflict, is associated with high rates of PTSD, depression, and behavioural disorders among African youth
| [14] | Sikazwe, M., & Mudenda, S. (2021). Violence exposure and psychological distress among youth in mining communities. Southern African Journal of Child and Adolescent Mental Health, 29(1), 19–30. |
[14]
. Many children in low-income communities face repeated exposure to violence, which undermines emotional resilience. These patterns echo reports from Bindura District, where social workers have observed rising behavioural challenges among children exposed to unstable home environments.
3.2.6. Gaps in African Mental Health Infrastructure
Across the continent, mental health systems remain under-resourced. Most countries have fewer than one psychiatrist per 500,000 people, and child psychologists are even rarer
| [15] | UNICEF Africa. (2022). Strengthening child mental health systems in Sub-Saharan Africa. UNICEF Regional Office. |
[15]
. School-based counselling is limited, and most interventions are reactive rather than preventive. These systemic gaps closely resemble Zimbabwe’s challenges.
3.3. Local Overview
3.3.1. Child and Adolescent Mental Health in Zimbabwe
Zimbabwean literature consistently shows that mental health conditions among children and adolescents are increasing, yet early detection remains weak. Studies in urban and peri-urban districts such as Harare and Mutare report rising symptoms of anxiety, depression, and behavioural disorders among school-going youth
| [4] | Chikwanha, T., Muchenje, L., & Taderera, C. (2023). Exam stress and mental wellbeing among Zimbabwean learners. Journal of Educational Psychology in Africa, 5(1), 33–47. |
[4]
. These conditions often remain undiagnosed due to stigma and limited psychosocial support in schools and clinics.
3.3.2. Effects of Economic Challenges on Youth Mental Health
Zimbabwe’s prolonged economic instability has far-reaching implications for child and adolescent mental health. High unemployment and income instability create stressful home environments where children absorb emotional strain from adults. Research shows that economic pressure leads to increased family conflict, parental stress, and weakened emotional support for children
| [3] | Mupambireyi, Z., & Musonza, T. (2021). Effects of economic hardship on child and adolescent wellbeing in Zimbabwe. Journal of Community Psychology in Africa, 7(2), 55–68. |
[3]
. In Bindura District, many households depend on informal mining, vending, or casual labour, which increases insecurity and emotional distress for children.
3.3.3. School-related Stress in Zimbabwean Schools
School stress is one of the most documented contributors to mental health problems among Zimbabwean learners. Overcrowded classrooms, high teacher-student ratios, frequent assessments, and pressure to pass Grade Seven, O-Level, and A-Level exams create sustained anxiety
| [4] | Chikwanha, T., Muchenje, L., & Taderera, C. (2023). Exam stress and mental wellbeing among Zimbabwean learners. Journal of Educational Psychology in Africa, 5(1), 33–47. |
[4]
. Learners often fear disappointing teachers or parents, leading to withdrawal, irritability, or sleep problems. Guidance and counselling departments, where they exist, are often understaffed and under-resourced.
3.3.4. Family Dynamics, Parental Absence, and Parenting Challenges
Family conditions significantly influence mental health. Zimbabwean studies highlight that parental migration, marital conflict, substance abuse, and illness leave children vulnerable to emotional instability
| [16] | Makurira, L., Mandiyanike, D., & Mhlanga, S. (2021). Parenting challenges and child wellbeing in Zimbabwe: A social-work perspective. Zimbabwe Journal of Social Sciences, 14(2), 44–56. |
[16]
. In households affected by chronic illness or death, children may assume caregiving roles, leading to emotional exhaustion. Bindura District has reported increasing cases of children presenting with stress linked to parental absence, especially in mining areas where adults work long hours.
3.3.5. Substance Abuse Trends Among Zimbabwean Adolescents
There is growing evidence of substance use among Zimbabwean adolescents, particularly marijuana, mutoriro (crystal meth), inhalants, and homemade alcohol
| [17] | Muziri, T., & Zinyemba, T. (2022). Substance abuse trends among adolescents in Mashonaland Central Province. Zimbabwe Public Health Journal, 3(1), 17–29. |
[17]
. Substance use is linked to peer pressure, limited recreational spaces, and emotional distress. In Bindura’s artisanal mining communities, access to substances is relatively easy, placing children and adolescents at heightened risk of addiction and associated mental health disorders.
3.3.6. Cultural Silence and Mental Health Perceptions in Zimbabwe
Stigma around mental illness remains widespread in Zimbabwe. Many families interpret symptoms such as anxiety, depression, or hallucinations through cultural or spiritual lenses, leading to delayed medical intervention
| [18] | Nyatsanza, T., & Chingono, A. (2020). Cultural perceptions and stigma towards mental illness in Zimbabwean communities. Journal of African Mental Health, 8(3), 71–85. |
[18]
. Children are often discouraged from speaking about emotional struggles, reinforcing silence and internal emotional suffering. This cultural dynamic significantly affects early detection in Bindura District.
3.3.7. Resource Shortages in Zimbabwe's Mental Health System
Zimbabwe faces critical shortages of mental health professionals, with only a handful of child psychologists serving large populations
| [1] | UNICEF. (2023). Child and adolescent mental health in low-resource settings: A situational analysis. UNICEF Publications. |
[1]
. School counsellors often juggle multiple roles and lack specialised training in child mental health. In rural districts like Bindura, these shortages mean emotional and behavioural disorders frequently go undiagnosed or misinterpreted as misbehaviour.
3.3.8. Evidence Gaps in Rural and Peri-Urban Communities
Despite increasing attention to youth mental health, research remains heavily urban-centric. There is a notable lack of studies focusing specifically on Bindura District or similar peri-urban and rural communities, where stressors differ significantly from those in large cities. This creates a gap that the current study aims to fill.
4. Research Methodology
4.1. Research Design
This study employed a qualitative research design to explore mental health challenges among children and adolescents in Bindura District. A qualitative approach was chosen because emotional and behavioural challenges are best understood through lived experiences and social interactions rather than numerical trends
| [19] | Creswell, J. W. (2021). Qualitative inquiry and research design: Choosing among five approaches (4th ed.). Sage Publications. |
[19]
. The design enabled participants to explain how school pressure, family stress, cultural beliefs, and community conditions shape mental wellbeing.
4.2. Study Area and Population
The research was conducted in four communities within Bindura District: Manhenga, Chireka, Nyava, and Musana. Data were collected from four schools (two primary and two secondary), one rural health clinic, and one community child-care centre. The study population consisted of adults who interact with children daily and could identify emotional or behavioural changes.
4.3. Sampling
A total of 24 participants took part in the study. These included:
1) 8 teachers (4 primary, 4 secondary)
2) 3 school counsellors
3) 3 community health workers
4) 4 social workers from the District Social Welfare Office
5) 6 caregivers (parents/guardians)
The sample size was adequate because participants were selected based on their direct experience with children’s mental health issues.
Purposive sampling was used to select participants who met three inclusion criteria
| [19] | Creswell, J. W. (2021). Qualitative inquiry and research design: Choosing among five approaches (4th ed.). Sage Publications. |
[19]
.
1) minimum one year of experience working with children,
2) previous exposure to cases of emotional or behavioural distress,
3) willingness to participate in open-ended discussions,
| [20] | Etikan, I. (2020). Purposeful sampling and its relevance in qualitative research. American Journal of Social Science Research, 8(3), 100–106. |
[20]
.
This ensured that only knowledgeable and experienced individuals were included.
4.4. Data Collection Methods
Data were collected over four weeks using three strategies:
4.4.1. Semi-structured Interviews
18 interviews were conducted (30–45 minutes each). Interviewees included teachers (8), counsellors (3), health workers (3), and social workers (4). Interviews followed a flexible guide with prompts on school stress, behavioural signs, and family challenges.
4.4.2. Observations
6 classroom observations (45–60 minutes each) were conducted across two primary and two secondary schools. Observations focused on learner behaviour, engagement, signs of anxiety or withdrawal, and teacher–learner interactions.
4.4.3. Informal Conversations
10 informal conversations with caregivers and community members were held, lasting 10–20 minutes each. These captured community-level perceptions, cultural interpretations, and barriers to help-seeking. No audio recordings were used but instead, detailed field notes were written to maintain participant trust.
4.5. Data Analysis
Thematic analysis was used the following six steps
| [21] | Braun, V., & Clarke, V. (2021). Thematic analysis: A practical guide for understanding qualitative data. Qualitative Research in Psychology, 18(3), 248–271. |
[21]
. Interview notes and observation records were transcribed manually the same day they were collected. Coding was done using coloured highlighters to group similar ideas (e.g., school pressure, stigma, family conflict). Codes were then merged into broader themes representing school, family, peer, and community influences.
4.6. Ethical Considerations
Ethical approval was obtained from Bindura District Education Office and the Ministry of Public Service, Labour and Social Welfare. Participants were informed about the study’s purpose, confidentiality measures, and their right to withdraw. All identifying details were anonymised. Parental consent and child assent were obtained before discussing any issues relating to minors.
5. Findings
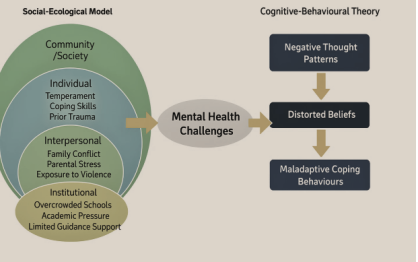
The findings presented in this section draw from interviews, classroom observations, and informal conversations conducted with teachers, counsellors, caregivers, social workers, and community health workers across Bindura District. The purpose of this section is to capture the lived realities of children and adolescents experiencing mental health challenges and to provide a clear, grounded picture of the factors shaping those challenges. The themes are organised according to individual, family, school, community, and service-related influences, consistent with the social-ecological perspective guiding the study.
5.1. Themes Emerging from the Data
1) Emotional, behavioural, and cognitive distress among children
2) Family instability and economic pressure as major triggers
3) School stress and classroom dynamics as daily sources of anxiety
4) Community-level factors such as poverty, violence, and stigma
5) Significant service gaps and reluctance to seek professional help
These themes consistently appeared across interviews and observations, suggesting that mental health challenges in Bindura District arise from a combination of structural hardship, stressful school environments, strained family conditions, and limited access to support.
5.2. Individual-level Experiences of Mental Health Challenges
Findings revealed that many children and adolescents in Bindura District demonstrate clear emotional, behavioural, and cognitive indicators of psychological distress. Teachers, counsellors, and caregivers were able to point out specific signs that they had observed repeatedly.
5.2.1. Emotional Symptoms
Teachers from both primary and secondary schools described a growing number of learners showing withdrawal, sadness, irritability, and emotional numbness. One Grade Seven teacher explained:
“Some children come to school looking tired and emotionally drained. They sit quietly for long periods, and even when spoken to, they answer in very soft voices.”
(Primary school teacher, Manhenga)
Health workers similarly noted frequent presentations of unexplained headaches and stomach aches, common physical expressions of emotional distress among children. Several adolescents were reported to cry privately during break time or after lessons, particularly during examination periods.
5.2.2. Behavioural Symptoms
Behavioural changes were another recurring pattern. Social workers highlighted increased cases of aggressive behaviour, defiance, or sudden outbursts at home. In observations, some learners struggled with attention, displayed hyperactivity, or frequently left their desks without permission.
One secondary school teacher shared:
“We are seeing more learners who just walk out of class when overwhelmed. Some throw chairs, some shout. For many, this behaviour only started recently.”
(Secondary school teacher, Nyava)
Conversely, some children responded to stress through extreme compliance and silence, avoiding eye contact and refraining from participating in class discussions.
5.2.3. Cognitive Symptoms
Teachers frequently reported concentration problems among learners. During classroom observations, it was common to see students staring at their books without engaging with the content. Counsellors mentioned memory lapses, especially around exam season, where learners reported “blanking out.”
A counsellor explained:
“Some students tell us they read the same page ten times and still cannot remember anything. They panic and then lose confidence.”
(School counsellor, Chireka)
Cognitive strain was particularly pronounced among adolescents preparing for O-Level and A-Level examinations, where expectations are high and failure carries serious academic consequences.
5.2.4. Personal Coping Responses
Many children adopted coping strategies that were either ineffective or harmful. Younger children often resorted to avoidance: skipping school, hiding homework, or pretending to be ill. Adolescents were more likely to seek escape through peer groups, substance use, or long hours on their phones.
A social worker noted:
“Some teenagers isolate themselves. Others join risky peer groups because they feel understood there.”
(Bindura District Social Welfare Office)
Healthy coping strategies, such as talking to a trusted adult, were rare, mainly due to stigma and fear of being labeled “weak.”
5.3. Family and Home Environment Influences
Family conditions emerged as one of the strongest determinants of children’s mental health in Bindura District.
5.2.1. Family Conflict and Instability
Teachers and social workers consistently described cases where children were emotionally affected by ongoing parental conflict, separation, or domestic violence. Caregivers admitted that arguments at home often took place in the presence of children, who reacted with fear, anxiety, or withdrawal.
One caregiver shared:
“When their father and I argue, the children stop eating. They just sit quietly. One of them cries at night.”
(Caregiver, Musana)
Children exposed to unstable family environments displayed higher levels of aggression, poor concentration, or emotional distress.
5.2.2. Parental Stress and Economic Strain
Economic hardship was a recurring theme. Many households rely on vending, casual labour, or artisanal mining, creating financial instability that affects children indirectly and directly.
A teacher noted:
“Learners come to school without lunch. Some have not eaten since the previous night. How can you expect concentration under those conditions?”
(Primary school teacher, Chireka)
Economic stress also led to reduced emotional availability from parents, who often spent long hours searching for income.
5.2.3. Parenting Styles and Emotional Support
Findings revealed that many parents struggled to provide emotional support due to stress, time constraints, or limited understanding of child mental health.
Counsellors explained that some parents dismissed their children’s emotional concerns as “attention seeking,” while others used harsh punishment in response to behavioural changes.
This reinforced silence among children, who feared being misunderstood or punished if they expressed distress.
5.2.4. Caregiver Migration or Absence
In several families, one or both parents migrated for work to Harare, Mazowe, or South Africa. Children left behind under the care of relatives or older siblings expressed feelings of abandonment, loneliness, and responsibility overload.
A social worker summarised:
“Children in these homes take on adult duties. They cook, clean, and look after younger siblings. It is too much pressure for their age.”
(Social worker, Bindura)
These situations often resulted in behavioural challenges, reduced academic performance, and emotional withdrawal.
5.4. School-related Pressures and Experiences
The school environment played a major role in shaping mental wellbeing.
5.3.1. Exam Pressure and Academic Expectations
Across all four schools visited, teachers reported heightened exam pressure, especially in Grades Seven, Form Four, and Form Six. Learners expressed fear of disappointing parents or failing national examinations.
A Form Four student told a counsellor (reported indirectly):
“If I fail, my parents will say I didn’t try. But I am trying. Sometimes I just panic.”
Observations showed tension during morning lessons, where teachers repeatedly emphasised exam preparedness, sometimes unintentionally increasing anxiety.
5.3.2. Teacher–learner Interactions
Most teachers were supportive, but some adopted strict or punitive approaches that contributed to fear and stress. In one observed class, a teacher’s loud scolding caused several learners to freeze and stop participating.
Teachers themselves acknowledged being under pressure:
“We are overwhelmed. Too many students, limited materials, too many deadlines. Sometimes we shout out of frustration, not because we want to.”
(Secondary school teacher, Manhenga)
5.3.3. Bullying and Peer Dynamics
Bullying emerged as a serious concern. Cases included name-calling, teasing, exclusion, and in some instances, physical aggression. Adolescents reported being mocked for their clothes, socio-economic background, academic performance, or physical appearance.
A counsellor shared:
“Most children do not report bullying. They fear being targeted again.”
Victims of bullying exhibited signs of anxiety, withdrawal, and declining grades.
5.3.4. School Counselling Limitations
All schools had at least one designated counsellor, but the counsellors also taught full timetables and lacked specialised training in mental health.
One counsellor said:
“We want to help, but there is no private room for counselling, no materials, no training workshops. It is difficult.”
This limited the schools’ ability to identify and support learners struggling with emotional or behavioural problems.
5.5. Community and Social Influences
Beyond the family and school, community conditions significantly shaped mental health.
5.4.1. Poverty and Insecure Livelihoods
The communities visited rely heavily on informal jobs. Children absorb the stress of unstable livelihoods, sometimes witnessing parents borrow money or argue over expenses.
One health worker commented:
“Poverty affects the whole household atmosphere. Children sense when there is no money.”
Many children work after school, selling vegetables, helping in markets, or caring for siblings, which increases exhaustion and reduces time for rest or homework.
5.4.2. Exposure to Violence
Some households and neighbourhoods experience frequent shouting, fighting, or substance-related conflicts. Adolescents in mining communities reported seeing adults intoxicated or engaging in violent outbursts.
A teacher revealed:
“Learners describe situations that clearly show they witness violence at home. It affects how they relate with peers.”
Exposure to violence contributed to fear, aggression, and trauma-related symptoms.
5.4.3. Cultural Silence Around Mental Health
Across all communities, mental health remained a sensitive topic. Many families preferred not to discuss emotional struggles for fear of appearing weak or being judged by neighbours.
A caregiver explained:
“In our community, if you say your child has stress, people will gossip.”
This silence delays recognition and treatment.
5.4.4. Community Beliefs and Stigma
Mental health concerns were sometimes attributed to supernatural or spiritual causes. Families often sought help from prophets or traditional healers before considering clinical services.
While some families found comfort in spiritual guidance, help-seeking delays often worsened symptoms.
5.6. Service Gaps and Barriers to Help-seeking
5.5.1. Shortage of Mental Health Professionals
Bindura District has very few mental health specialists. Teachers and caregivers reported long referral routes to Bindura Hospital, with some children waiting months to be seen by a psychologist.
5.5.2. Weak Referral Pathways
Schools lacked clear referral systems. Cases were sometimes reported to social workers, but follow-up was inconsistent due to workload and transport challenges.
5.5.3. Dependence on Spiritual or Traditional Explanations
Some caregivers preferred spiritual interpretations, believing emotional distress to be caused by curses, “evil spirits,” or witchcraft, which diverted children away from clinical support.
5.5.4. Fear of Discrimination and Labelling
Adolescents avoided seeking help due to fear of being called “mentally disturbed” or being isolated by peers.
This stigma created an environment where suffering often went unnoticed or unaddressed.
5.7. Case Illustrations from Bindura District
To further illuminate the findings, several anonymised case narratives are presented below.
5.6.1. Case 1: The Silent Boy in Grade Seven
A 13-year-old boy showed increasing withdrawal during lessons. Teachers reported he stopped answering questions and rarely interacted with peers. Interviews revealed his father had recently lost his job, and the family struggled to afford food. The boy felt responsible for helping at home and reported headaches and stomach pain whenever exams were mentioned.
5.6.2. Case 2: The Overwhelmed Form Four Girl
A 16-year-old girl began showing panic during mock exams. Her counsellor said she often cried before tests. She explained that her parents had told her she must pass or risk being sent to relatives in Harare to work as a domestic helper. She studied late into the night, slept poorly, and felt constantly anxious.
5.6.3. Case 3: The Bullying Victim
A 14-year-old boy was repeatedly teased for wearing torn shoes. He became withdrawn and avoided break times. Observations confirmed he sat alone daily. When interviewed, he said other students mocked his mother, who sells vegetables at the market. His self-esteem declined significantly, affecting participation and grades.
5.6.4. Case 4: The Child Left in Relatives’ Care
Two siblings aged 10 and 12 lived with their grandmother after both parents migrated to South Africa. They woke early to cook, fetch water, and prepare for school. Teachers reported they were often tired, struggled to concentrate, and sometimes fell asleep in class. They expressed fear of disappointing their grandmother, who was also overwhelmed.
5.6.5. Case 5: The Substance-exposed Teenager
A 15-year-old boy began using marijuana with older youths in the mining area. His caregiver said he often came home late, avoided chores, and became irritable. The teenager told a counsellor he used drugs “to forget problems.” He showed signs of mild addiction and emotional instability.
5.6.6. Case 6: The Girl Caring for a Sick Parent
A 12-year-old girl cared for her chronically ill mother and two younger siblings. She missed school frequently and reported feelings of hopelessness. Teachers observed she cried when asked about homework. The burden of caregiving created consistent emotional distress.
5.6.7. Summary of Key Patterns
The findings reveal a complex interplay of emotional distress, family instability, school pressure, community poverty, and cultural silence, all shaping mental health outcomes among children and adolescents in Bindura District. Mental health challenges were visible across all age groups and school levels, and patterns were remarkably consistent across communities.