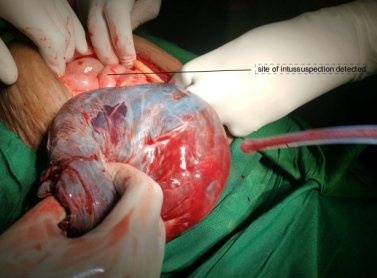
Background: Colonic intussusception during pregnancy is an extremely rare case that may have occurred due to various factors like colon cancer, fibroma, colonic leiomyoma and lipoma. It requires a multidisciplinary approach to managing parturient presented with those cases, especially during labour. Colonic intussusception has no specific symptoms to differentiate it from labour induced pain and is also difficult to image during this period. This is a case report of colonic intussusception managed with spinal anesthesia combined with controlled general anesthesia for both maternal and foetal outcomes. Case presentation: A 32-year-old gravida IV para III, 38-week gestational age female patients with a history of severe abdominal pain, nausea, and vomiting presented to our institution. She has had pushing-down pain for six hours’ duration, sweating, abdominal cramping, and fever for 2 days’ duration. Immediately after she entered the gynecology department, she was diagnosed with obstructed labour and prepared for an emergency caesarean section. After the cesarean section was conducted, the baby was delivered, and uterine contractility was checked. A palpable tubular mass on the mesenteric side of the ischemic colon was appeared. The ischemic colon was packed with warm water until peristalsis regains. The abdomen was washed thoroughly, and a biopsy was taken from the mass. Conclusion: Anesthesia management for unexpected cases during pregnancy is very challenging and requires caution for both intraoperative maternal life and postoperative morbidity. There is no gold standard and safe anesthesia technique for pregnancy patients presented with a non-obstetric emergency like bowel obstruction. Therefore, risks and benefits of the technique, and the perioperative patient condition should be considered. Our case was managed with spinal anesthesia with controlled general anesthesia for both the mother and neonate with good outcomes.
| Published in | Science Discovery Medicine (Volume 1, Issue 2) |
| DOI | 10.11648/j.sdmed.20260102.15 |
| Page(s) | 99-103 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Bowel Obstruction, Controlled General Anesthesia, Intussusception, Pregnancy, Spinal Anesthesia
Vital sign/Time | 05:00 | 05:10 | 05:20 | 05:30 | 05:40 | 05:50 | 06:00 | 06:10 | 06:20 | 06:30 | 06:40 |
|---|---|---|---|---|---|---|---|---|---|---|---|
BP | 120/70 | 120/70 | 90/59 | 90/59 | 110/67 | 90/65 | 110/54 | 110/54 | 110/54 | 110/55 | 130/80 |
PR | 85 | 90 | 96 | 96 | 96 | 90 | 80 | 85 | 80 | 98 | 87 |
SPO2 | 99 | 99 | 100 | 99 | 98 | 96 | 98 | 96 | 100 | 99 | 99 |
ECG | SR | SR | SR | SR | SR | SR | SR | SR | SR | SR | SR |
Vital sign/Time | 06:50 | 07:00 | 07:10 | 07:20 | 07:30 | 07:40 | 07:50 | 08:00 | 08:10 | 08:20 |
|---|---|---|---|---|---|---|---|---|---|---|
BP | 130/80 | 136/80 | 110/83 | 120/75 | 115/75 | 120/67 | 120/75 | 110/54 | 120/85 | 110/75 |
PR | 86 | 76 | 75 | 70 | 80 | 84 | 75 | 90 | 90 | 95 |
SPO2 | 99 | 99 | 99 | 99 | 99 | 99 | 99 | 99 | 99 | 100 |
ECG | SR | SR | SR | SR | SR | SR | SR | SR | SR | SR |
ASA | American Societies of Anaesthesiologist |
Apgar | Appearance, Pulse, Grimace, Activity, Respiration |
BP | Blood Pressure |
I:E | Inspiration to Expiration Ratio |
ID | Internal Diameter |
Hgb | Haemoglobin |
Hct | Haematocrit |
ML | Millilitre |
MRI | Magnetic Resonance Imaging |
Plt | Platelet |
PR | Pulse Rate |
VT | Tidal Volume |
WBC | White Blood Cell |
| [1] | R. Achour, S. Harabi, and K. Neji, “Case Reports in Women ’ s Health Spontaneous acute intussusception in a pregnant woman,” Case Reports Women’s Heal., vol. 13, pp. 6–8, 2017, |
| [2] | R. Kr, C. Shekhar, R. Yadav, A. Bajracharya, and P. Lal, “Intussusception in adults : Institutional review,” Int. J. Surg., vol. 9, no. 1, pp. 91–95, 2011, |
| [3] | P. Soma-pillay, C. Nelson-piercy, H. Tolppanen, and A. Mebazaa, “Physiological changes in pregnancy,” vol. 27, no. 2, pp. 89–94, 2016, |
| [4] | E. O. Nwasor, “ANAESTHETIC MANAGEMENT OF INTUSSUSCEPTION IN PREGNANCY,” vol. 4, no. 4, pp. 185–187, 2005. |
| [5] | R. E. Wilson and D. Reali-marini, “VISUAL em VISUAL em,” vol. 5, no. 1, pp. 5–8, 2020. |
| [6] | A. Manuscript, “NIH Public Access,” vol. 218, no. 0, pp. 247–248, 2015, |
| [7] | M. O. Sungur, M. Karaden, M. Kili, and Z. Seyhan, “Spinal anesthesia for elective cesarean section is associated with shorter hospital stay compared to general anesthesia,” vol. 25, no. April, pp. 55–63, 2013, |
| [8] | A. Mustafa, L. Azzam, and H. M. Azzam, “A Case Report of a Primary Intususseption in Pregnancy,” vol. 4, no. 11, pp. 357–360, 2016, |
| [9] | A. Luhmann, R. Tait, and A. Hassn, “Case report Intussusception in a 20 weeks pregnant woman : a case report,” vol. 3, pp. 3–5, 2009, |
| [10] | K. Sudabattula, R. Gattani, T. Panchagnula, T. Dahmiwal, and N. Thatipalli, “Submucosal Lipoma-Induced Small Bowel Intussusception : A Case Study of Surgical Intervention and Management in an Adult Female,” vol. 16, no. 6, 2024, |
| [11] | F. Hayati, A. M. Zuki, M. C. Lim, and K. A. Karim, “A peculiar case of intususception in a pregnant woman : A diagnostic challenge,” vol. 18, pp. 2836–2839, 2023, |
| [12] | O. Oc, J. Onakewhor, and I. Oo, “Intussusception in Pregnancy - A Rarely Considered Diagnosis,” vol. 14, no. 1, pp. 145–148, 2010. |
| [13] | M. Bayoumi, “Effect of General Anesthesia versus Spinal Anesthesia in Cesarean Section on Regain of Gastrointestinal Motility,” vol. 68, no. July, pp. 1332–1338, 2017, |
| [14] | M. M. Wonte, A. T. Bantie, and M. Tadesse, “A pregnant lady with compound bowel obstruction managed with thoracic epidural as sole anesthesia in a resource-restricted setting: a case report,” J. Med. Case Rep., vol. 17, no. 1, pp. 1–5, 2023, |
APA Style
Hordofa, T. A., Ahmed, A. A., Woldemariam, B. B., Nerso, K. M. (2026). Spinal Anesthesia with Controlled General Anesthesia Management for Unexpected Colonic Intussusception During Cesarean Section in Resource Limited Area: A Rare Case Report. Science Discovery Medicine, 1(2), 99-103. https://doi.org/10.11648/j.sdmed.20260102.15
ACS Style
Hordofa, T. A.; Ahmed, A. A.; Woldemariam, B. B.; Nerso, K. M. Spinal Anesthesia with Controlled General Anesthesia Management for Unexpected Colonic Intussusception During Cesarean Section in Resource Limited Area: A Rare Case Report. Sci. Discov. Med. 2026, 1(2), 99-103. doi: 10.11648/j.sdmed.20260102.15
AMA Style
Hordofa TA, Ahmed AA, Woldemariam BB, Nerso KM. Spinal Anesthesia with Controlled General Anesthesia Management for Unexpected Colonic Intussusception During Cesarean Section in Resource Limited Area: A Rare Case Report. Sci Discov Med. 2026;1(2):99-103. doi: 10.11648/j.sdmed.20260102.15
@article{10.11648/j.sdmed.20260102.15,
author = {Tesfaye Asefa Hordofa and Abdurjebar Abdurrahman Ahmed and Bizuayehu Betemariam Woldemariam and Kelil Musa Nerso},
title = {Spinal Anesthesia with Controlled General Anesthesia Management for Unexpected Colonic Intussusception During Cesarean Section in Resource Limited Area: A Rare Case Report},
journal = {Science Discovery Medicine},
volume = {1},
number = {2},
pages = {99-103},
doi = {10.11648/j.sdmed.20260102.15},
url = {https://doi.org/10.11648/j.sdmed.20260102.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdmed.20260102.15},
abstract = {Background: Colonic intussusception during pregnancy is an extremely rare case that may have occurred due to various factors like colon cancer, fibroma, colonic leiomyoma and lipoma. It requires a multidisciplinary approach to managing parturient presented with those cases, especially during labour. Colonic intussusception has no specific symptoms to differentiate it from labour induced pain and is also difficult to image during this period. This is a case report of colonic intussusception managed with spinal anesthesia combined with controlled general anesthesia for both maternal and foetal outcomes. Case presentation: A 32-year-old gravida IV para III, 38-week gestational age female patients with a history of severe abdominal pain, nausea, and vomiting presented to our institution. She has had pushing-down pain for six hours’ duration, sweating, abdominal cramping, and fever for 2 days’ duration. Immediately after she entered the gynecology department, she was diagnosed with obstructed labour and prepared for an emergency caesarean section. After the cesarean section was conducted, the baby was delivered, and uterine contractility was checked. A palpable tubular mass on the mesenteric side of the ischemic colon was appeared. The ischemic colon was packed with warm water until peristalsis regains. The abdomen was washed thoroughly, and a biopsy was taken from the mass. Conclusion: Anesthesia management for unexpected cases during pregnancy is very challenging and requires caution for both intraoperative maternal life and postoperative morbidity. There is no gold standard and safe anesthesia technique for pregnancy patients presented with a non-obstetric emergency like bowel obstruction. Therefore, risks and benefits of the technique, and the perioperative patient condition should be considered. Our case was managed with spinal anesthesia with controlled general anesthesia for both the mother and neonate with good outcomes.},
year = {2026}
}
TY - JOUR T1 - Spinal Anesthesia with Controlled General Anesthesia Management for Unexpected Colonic Intussusception During Cesarean Section in Resource Limited Area: A Rare Case Report AU - Tesfaye Asefa Hordofa AU - Abdurjebar Abdurrahman Ahmed AU - Bizuayehu Betemariam Woldemariam AU - Kelil Musa Nerso Y1 - 2026/04/16 PY - 2026 N1 - https://doi.org/10.11648/j.sdmed.20260102.15 DO - 10.11648/j.sdmed.20260102.15 T2 - Science Discovery Medicine JF - Science Discovery Medicine JO - Science Discovery Medicine SP - 99 EP - 103 PB - Science Publishing Group UR - https://doi.org/10.11648/j.sdmed.20260102.15 AB - Background: Colonic intussusception during pregnancy is an extremely rare case that may have occurred due to various factors like colon cancer, fibroma, colonic leiomyoma and lipoma. It requires a multidisciplinary approach to managing parturient presented with those cases, especially during labour. Colonic intussusception has no specific symptoms to differentiate it from labour induced pain and is also difficult to image during this period. This is a case report of colonic intussusception managed with spinal anesthesia combined with controlled general anesthesia for both maternal and foetal outcomes. Case presentation: A 32-year-old gravida IV para III, 38-week gestational age female patients with a history of severe abdominal pain, nausea, and vomiting presented to our institution. She has had pushing-down pain for six hours’ duration, sweating, abdominal cramping, and fever for 2 days’ duration. Immediately after she entered the gynecology department, she was diagnosed with obstructed labour and prepared for an emergency caesarean section. After the cesarean section was conducted, the baby was delivered, and uterine contractility was checked. A palpable tubular mass on the mesenteric side of the ischemic colon was appeared. The ischemic colon was packed with warm water until peristalsis regains. The abdomen was washed thoroughly, and a biopsy was taken from the mass. Conclusion: Anesthesia management for unexpected cases during pregnancy is very challenging and requires caution for both intraoperative maternal life and postoperative morbidity. There is no gold standard and safe anesthesia technique for pregnancy patients presented with a non-obstetric emergency like bowel obstruction. Therefore, risks and benefits of the technique, and the perioperative patient condition should be considered. Our case was managed with spinal anesthesia with controlled general anesthesia for both the mother and neonate with good outcomes. VL - 1 IS - 2 ER -
Anesthesia Department, Madda Walabu University, Bale Robe, Ethiopia
Anesthesia Department, Madda Walabu University, Bale Robe, Ethiopia
Anesthesia Department, Madda Walabu University, Bale Robe, Ethiopia
Anesthesia Department, Madda Walabu University, Bale Robe, Ethiopia
Information