Introduction: The success of kidney transplantation depend on the effectiveness in certain key factors including excellent donor compatibility, immunosuppression and good surgical techniques. Exciting prospects in kidney transplantation is envisaged especially with the launching of standards and guidelines for the establishment and coordinating organ/tissue transplantation services by the Federal Government of Nigeria in March, 2025. We have come a long way with our five year experience in kidney transplantation. The use of branded immunosuppressive agents, excellent HLA/DSA typing and compatibility as well as ‘top notch’ surgical and medical team of experts have exponentially achieved a favorable outcome. Challenges are not unusual but we are hopeful that the future is promising and will offer more advancement in ‘tips and tricks’ of successful lifelong kidney transplantation. We report our experience in kidney transplantation over a 5 year period in our center. Methodology: This is a retrospective cohort study involving patients who had kidney transplantation in our facility over a 5 year period from January 2020 to December 2024. A proforma was designed to obtain existing records from our data base. Data analysis was conducted using Python with its libraries including Pandas, Numpy and Matplotib. P value of less than 0.05 was considered statistically significant. Results: Descriptive Statistics showed that a total of 104 patients had kidney transplantation surgery over the prescribed period. 66.35% were males while 33.65% were females. The average age of recipients was 46.27 years with a range of 24 to 72 years while the average age donors was 26.12 years with a range of 18 to 50 years. The average length of hospital stay after donor nephrectomy was 4.14 days while the average length of hospital stay for recipients post-surgery was 9.50 days with a range of 7-12 days. The etiology of renal failure were mainly long-term hypertension in 38.46%, diabetic mellitus in 29.81%, combination of both comorbid condition in 28.85%, autoimmune disease in 1.92% and genetic factor in 0.96%. Prognosis six months post-surgery was good in 82.69% and only 17.31% had unfavorable outcome. No donor mortality was observed. Conclusion: We have come a long way with our 5 years experience in management of end stage kidney disease in tropical Africa with excellent outcome. Though challenges are inevitable, the future still hold a promising exiting prospects as we envisage progressive experience and welcome new innovations including the use of minimal access techniques to achieve improved results.
| Published in | Science Journal of Clinical Medicine (Volume 14, Issue 2) |
| DOI | 10.11648/j.sjcm.20251402.11 |
| Page(s) | 12-19 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Kidney Transplantation, End Stage Kidney Disease, Chronic Kidney Disease, Hypertension, Diabetes Mellitus, Donor, Recipient
KTP | Kidney Transplantation |
ESKD | End Stage Kidney Disease |
CKD | Chronic Kidney Disease |
eGFR | Estimated Glomerular Filtration Rate |
DM | Diabetes Mellitus |
PRO | Patient Reported Outcome |
QoL | Quality of Life |
| [1] | Adam D. Barlow, Ahmed S. Ghoneima. Kidney Transplantation: Surgery (Oxford), 2023; Volume 41(9): 596-602, ISSN 02639319, |
| [2] | Harasyko C. Kidney transplantation. Nurs Clin North Am. 1989 Dec; 24(4): 851-63. PMID: 2685775. |
| [3] | Standards and Guidelines for Establishing and Coordinating Organ/Tissue Transplantatio Services in Nigeria. The Federal Ministry of Health and Social Welfare, March 2025. |
| [4] | Belitsky P, MacDonald AS, Lawen J, McAlister V, Bitter-Suermann H, Kiberd B, West K, Sketris I. Kidney transplantation, the Halifax experience. Clin Transpl. 1996: 231-40. PMID: 9286572. |
| [5] | Jamilya Saparbay, Mels Assykbayev, Saitkarim Abdugafarov, Gulnur Zhakhina, Saniya Abdrakhmanova, Aida Turganbekova, Zhuldyz Zhanzakova, Kulkayeva Gulnara, Kidney transplantation outcomes: Single center experience. ScienceDirect, 2022, 7(3), 100105, ISSN 2451-9596, |
| [6] |
Legendre C, Canaud G, Martinez F. Factors Influencing Long-term Outcome after Kidney Transplantation. Transpl Int. 2014 Jan; 27(1): 19-27.
https://doi.org/10.1111/tri.12217 Epub 2013 Nov 8. |
| [7] |
Akoh JA, Mathuram Thiyagarajan U. Renal Transplantation from Elderly Living Donors. J Transplant. 2013; 2013: 475964.
https://doi.org/10.1155/2013/475964 Epub 2013 Sep 12. |
| [8] | Nyengaard JR, Bendtsen TF. Glomerular number and size in relation to age, kidney weight, and body surface in normal man. Anatomical Record. 1992; 232(2): 194–201. |
| [9] | Burrows NR, Koyama A, Pavkov ME. Reported Cases of End-Stage Kidney Disease - United States, 2000-2019. MMWR Morb Mortal Wkly Rep. 2022 Mar 18; 71(11): 412-415. |
| [10] | United States Renal Data System. 2021 USRDS annual data report: epidemiology of kidney disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2021. Accessed March 7, 2022. |
| [11] |
Lim WH, Johnson DW, McDonald SP, Hawley C, Clayton PA, Jose MD, Wong G. Impending challenges of the burden of end-stage kidney disease in Australia. Med J Aust. 2019 Oct; 211(8): 374-380. e3.
https://doi.org/10.5694/mja2.50354 Epub 2019 Oct 8. PMID: 31595516. |
| [12] |
Vijay K, Neuen BL, Lerma EV. Heart Failure in Patients with Diabetes and Chronic Kidney Disease: Challenges and Opportunities. Cardiorenal Med. 2022; 12(1): 1-10.
https://doi.org/10.1159/000520909 Epub 2021 Nov 19. |
| [13] | Wang Y, Snoep JD, Hemmelder MH, van der Bogt KEA, Bos WJW, van der Boog PJM, Dekker FW, de Vries APJ, Meuleman Y. Outcomes after Kidney Transplantation, Let's Focus on the Patients' Perspectives. Clin Kidney J. 2021 Jan 20; 14(6): 1504-1513. |
| [14] |
Foroncewicz B, Mucha K, Florczak M, Szymańska A, Ciszek M, Durlik M, Górski A, Kieszek R, Kosieradzki M, Nazarewski S, Gałązka Z, Pączek L. Long-term Outcome of Renal Transplantation: A 10-year Follow-up of 765 Recipients. Pol Arch Intern Med. 2019 Aug 29; 129(7-8): 476-483.
https://doi.org/10.20452/pamw.14914 Epub 2019 Jul 30. |
| [15] | Khan, I., Wani, M., Wani, I. et al. Incidence of complications and outcome in live kidney transplant recipients at 1 year—a single center experience. Egypt J Intern Med 37, 30 (2025). |
| [16] |
Carrero JJ, Hecking M, Chesnaye NC, Jager KJ. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat Rev Nephrol. 2018 Mar; 14(3): 151-164.
https://doi.org/10.1038/nrneph.2017.181 Epub 2018 Jan 22. |
| [17] | Guillermo García GarcíaS, Arpana Iyengar, François Kaze, Ciara Kierans, Cesar Padilla-Altamira, Valerie A. Luyckx. Sex and Gender Differences in Chronic Kidney Disease and Access to Care around the Globe, Seminars in Nephrology, 2022, 42(2): 101-113, ISSN 0270-9295, |
| [18] |
Neri F, Furian L, Cavallin F, Ravaioli M, Silvestre C, Donato P, La Manna G, Pinna AD, Rigotti P. How Does Age Affect the Outcome of Kidney Transplantation in Elderly Recipients? Clin Transplant. 2017 Oct; 31(10).
https://doi.org/10.1111/ctr.13036 Epub 2017 Aug 20. |
| [19] |
Ruch B, Tsering D, Bhati C, Kumar D, Saeed M, Lee SD, Khan A, Imai D, Bruno D, Levy M, Cotterell A, Sharma A. Right versus left fully robotic live donor nephrectomy and open kidney transplantation: Does the laterality of the donor kidney really matter? Asian J Urol. 2023 Oct; 10(4): 453-460.
https://doi.org/10.1016/j.ajur.2023.08.004 Epub 2023 Aug 26. |
| [20] | Minjur Dorji, Yeshey Penjore, Tshokey, Gyem Dorji. Aetiology of End-stage Renal Disease at the National Referral Hospital of Bhutan. Bhutan Health Journal; 2023, 9(1): 1-5 |
| [21] | Hashmi MF, Benjamin O, Lappin SL. End-Stage Renal Disease. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2025 Jan-. Available from: |
APA Style
Kenenna, O., Christoper, O., Kumar, A. R., Felix, M., Abayomi, A., et al. (2025). Kidney Transplantation: Our Experience in a Private Tertiary Center in Abuja. Science Journal of Clinical Medicine, 14(2), 12-19. https://doi.org/10.11648/j.sjcm.20251402.11
ACS Style
Kenenna, O.; Christoper, O.; Kumar, A. R.; Felix, M.; Abayomi, A., et al. Kidney Transplantation: Our Experience in a Private Tertiary Center in Abuja. Sci. J. Clin. Med. 2025, 14(2), 12-19. doi: 10.11648/j.sjcm.20251402.11
AMA Style
Kenenna O, Christoper O, Kumar AR, Felix M, Abayomi A, et al. Kidney Transplantation: Our Experience in a Private Tertiary Center in Abuja. Sci J Clin Med. 2025;14(2):12-19. doi: 10.11648/j.sjcm.20251402.11
@article{10.11648/j.sjcm.20251402.11,
author = {Obiatuegwu Kenenna and Otabor Christoper and Agrawal Rajesh Kumar and Magnus Felix and Aremu Abayomi and Aniede Ernest and Olawoye Olatunde and Odinenu Theodora and Chikodili Ugochukwu},
title = {Kidney Transplantation: Our Experience in a Private Tertiary Center in Abuja
},
journal = {Science Journal of Clinical Medicine},
volume = {14},
number = {2},
pages = {12-19},
doi = {10.11648/j.sjcm.20251402.11},
url = {https://doi.org/10.11648/j.sjcm.20251402.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjcm.20251402.11},
abstract = {Introduction: The success of kidney transplantation depend on the effectiveness in certain key factors including excellent donor compatibility, immunosuppression and good surgical techniques. Exciting prospects in kidney transplantation is envisaged especially with the launching of standards and guidelines for the establishment and coordinating organ/tissue transplantation services by the Federal Government of Nigeria in March, 2025. We have come a long way with our five year experience in kidney transplantation. The use of branded immunosuppressive agents, excellent HLA/DSA typing and compatibility as well as ‘top notch’ surgical and medical team of experts have exponentially achieved a favorable outcome. Challenges are not unusual but we are hopeful that the future is promising and will offer more advancement in ‘tips and tricks’ of successful lifelong kidney transplantation. We report our experience in kidney transplantation over a 5 year period in our center. Methodology: This is a retrospective cohort study involving patients who had kidney transplantation in our facility over a 5 year period from January 2020 to December 2024. A proforma was designed to obtain existing records from our data base. Data analysis was conducted using Python with its libraries including Pandas, Numpy and Matplotib. P value of less than 0.05 was considered statistically significant. Results: Descriptive Statistics showed that a total of 104 patients had kidney transplantation surgery over the prescribed period. 66.35% were males while 33.65% were females. The average age of recipients was 46.27 years with a range of 24 to 72 years while the average age donors was 26.12 years with a range of 18 to 50 years. The average length of hospital stay after donor nephrectomy was 4.14 days while the average length of hospital stay for recipients post-surgery was 9.50 days with a range of 7-12 days. The etiology of renal failure were mainly long-term hypertension in 38.46%, diabetic mellitus in 29.81%, combination of both comorbid condition in 28.85%, autoimmune disease in 1.92% and genetic factor in 0.96%. Prognosis six months post-surgery was good in 82.69% and only 17.31% had unfavorable outcome. No donor mortality was observed. Conclusion: We have come a long way with our 5 years experience in management of end stage kidney disease in tropical Africa with excellent outcome. Though challenges are inevitable, the future still hold a promising exiting prospects as we envisage progressive experience and welcome new innovations including the use of minimal access techniques to achieve improved results.
},
year = {2025}
}
TY - JOUR T1 - Kidney Transplantation: Our Experience in a Private Tertiary Center in Abuja AU - Obiatuegwu Kenenna AU - Otabor Christoper AU - Agrawal Rajesh Kumar AU - Magnus Felix AU - Aremu Abayomi AU - Aniede Ernest AU - Olawoye Olatunde AU - Odinenu Theodora AU - Chikodili Ugochukwu Y1 - 2025/05/26 PY - 2025 N1 - https://doi.org/10.11648/j.sjcm.20251402.11 DO - 10.11648/j.sjcm.20251402.11 T2 - Science Journal of Clinical Medicine JF - Science Journal of Clinical Medicine JO - Science Journal of Clinical Medicine SP - 12 EP - 19 PB - Science Publishing Group SN - 2327-2732 UR - https://doi.org/10.11648/j.sjcm.20251402.11 AB - Introduction: The success of kidney transplantation depend on the effectiveness in certain key factors including excellent donor compatibility, immunosuppression and good surgical techniques. Exciting prospects in kidney transplantation is envisaged especially with the launching of standards and guidelines for the establishment and coordinating organ/tissue transplantation services by the Federal Government of Nigeria in March, 2025. We have come a long way with our five year experience in kidney transplantation. The use of branded immunosuppressive agents, excellent HLA/DSA typing and compatibility as well as ‘top notch’ surgical and medical team of experts have exponentially achieved a favorable outcome. Challenges are not unusual but we are hopeful that the future is promising and will offer more advancement in ‘tips and tricks’ of successful lifelong kidney transplantation. We report our experience in kidney transplantation over a 5 year period in our center. Methodology: This is a retrospective cohort study involving patients who had kidney transplantation in our facility over a 5 year period from January 2020 to December 2024. A proforma was designed to obtain existing records from our data base. Data analysis was conducted using Python with its libraries including Pandas, Numpy and Matplotib. P value of less than 0.05 was considered statistically significant. Results: Descriptive Statistics showed that a total of 104 patients had kidney transplantation surgery over the prescribed period. 66.35% were males while 33.65% were females. The average age of recipients was 46.27 years with a range of 24 to 72 years while the average age donors was 26.12 years with a range of 18 to 50 years. The average length of hospital stay after donor nephrectomy was 4.14 days while the average length of hospital stay for recipients post-surgery was 9.50 days with a range of 7-12 days. The etiology of renal failure were mainly long-term hypertension in 38.46%, diabetic mellitus in 29.81%, combination of both comorbid condition in 28.85%, autoimmune disease in 1.92% and genetic factor in 0.96%. Prognosis six months post-surgery was good in 82.69% and only 17.31% had unfavorable outcome. No donor mortality was observed. Conclusion: We have come a long way with our 5 years experience in management of end stage kidney disease in tropical Africa with excellent outcome. Though challenges are inevitable, the future still hold a promising exiting prospects as we envisage progressive experience and welcome new innovations including the use of minimal access techniques to achieve improved results. VL - 14 IS - 2 ER -
Department of Surgery, Alliance Hospital and Service Limited Abuja, Nigeria;Department of Surgery, Baze University Abuja, Abuja Nigeria
Department of Surgery, Alliance Hospital and Service Limited Abuja, Nigeria
Department of Surgery, Alliance Hospital and Service Limited Abuja, Nigeria;Department of Surgery, National Kidney Hospital, SAS Nagar Jalandhar, India
Department of Surgery, Alliance Hospital and Service Limited Abuja, Nigeria
Department of Surgery, Alliance Hospital and Service Limited Abuja, Nigeria
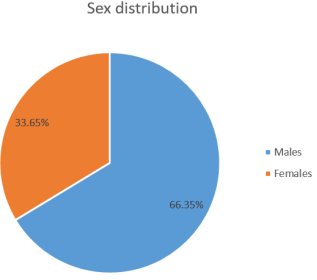
Figure 1. Sex distribution of recipients.
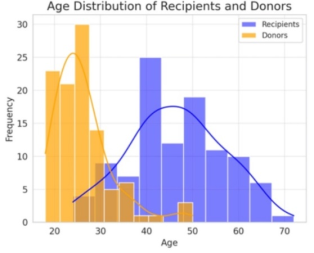
Figure 2. Showings age distribution of both donors and recipients.
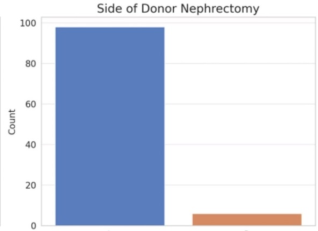
Figure 3. Site of donor nephrectomy.
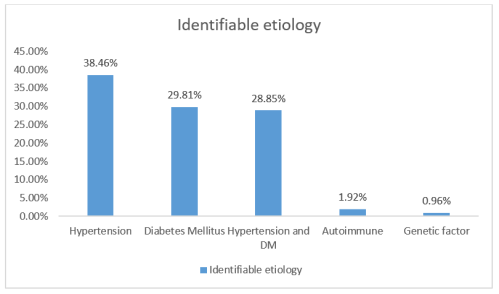
Figure 4. Identifiable etiology of ESKD in our patients.
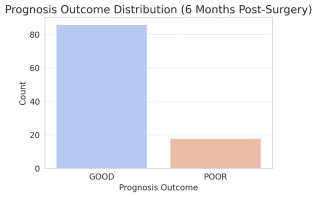
Figure 5. Prognosis outcome after 6 months.
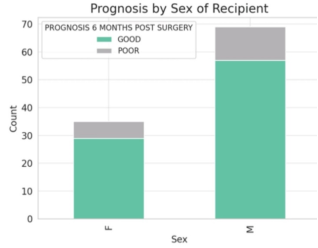
Figure 6. Prognosis by sex.
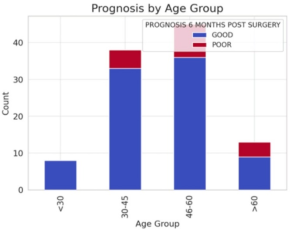
Figure 7. Prognosis by age group.
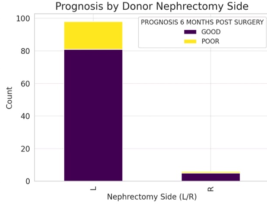
Figure 8. Prognosis based on side of kidney received by recipients.
Information

