1. Introduction
Psychosocial disability refers to the difficulties that a person with severe and persistent mental illness (SPMI) has performing daily tasks because of their impairments, which often prevents them from participating in society through education, employment, recreation, relationships, and having a decent place to live
| [9] | Harvey, C., Brophy, L., Parsons, S., Moeller-Saxone, K., Grigg, M., and Siskind, D. (2016). People living with psychosocial disability: Rehabilitation and recovery- informed service provision within the second Australian national survey of psychosis. Australian & New Zealand Journal of Psychiatry, 50(6): 534-547. https://doi.org/10.1177/0004867415610437 |
[9]
. In the 2010 Global Burden of Disease research, mental illness was the largest cause of years spent disabled, with most of those affected living in poor and middle-income nations (LMIC). People who have received a mental health diagnosis or identified that they have limitations in basic psychological and social activities, as well as those who have experienced the negative social consequences of psychological or social disability, such as discrimination and exclusion, are referred to as people with psychosocial disability
| [5] | Drew, N., Funk, M., Tang, S., Lamichhane, J., Cha´vez, E., Katontoka, S., Pathare, S., Lewis, O., Gostin, L., and Saraceno, B. (2011). Human rights violations of people with mental and psychosocial disabilities: an unresolved global crisis. The Lancet, 378(9803): 1664-1675. https://doi.org/10.1016/S0140-6736(11)61458-X |
| [15] | Mathias, K., Pant, H., Marella, M., Singh, L., Murthy, G., and Grills, N. (2018). Multiple barriers to participation for people with psychosocial disability in Dehradun district, north India: a cross-sectional study. BMJ open, 8(2): e019443. https://doi.org/10.1136/bmjopen-2017-019443 |
[5, 15]
. Anxiety, depression, and a variety of other mental health issues are classified as psychosocial disabilities because of the actual or perceived impairment they cause in daily life
| [19] | Ringland, K. E., Nicholas, J., Kornfield, R., Lattie, E. G., Mohr, D. C., and Reddy, M. (2019). Understanding mental ill-health as psychosocial disability: Implications for assistive technology. In Proceedings of the 21st International ACM SIGACCESS Conference on Computers and Accessibility, pages 156-170. https://doi.org/10.1145/3308561.3353785 |
[19]
. Psychosocial impairment has traditionally been studied using diagnostic classification and prescription regimens, resulting in a medicalization of the experience
| [7] | Fernandes, H., Cantrill, S., Kamal, R., and Shrestha, R. (2017). Inclusion of people with psychosocial disability in low and middle income contexts: a practice review. Christian J Global Health, 4(3): 72-81. |
[7]
. Schizophrenia and psychotic diseases are integrated (ICD-10) in the mhGAP Intervention Guide and Chapter F2 of the International Classification of Diseases, according to the World Health Organization
| [17] | Organisation, W. H. et al. (2016). mhgap intervention guide mental health gap action program version 2.0 for mental, neurological and substance use disorders in non- specialized health settings. World Health Organization, pages 1-173. |
| [20] | Ro¨ssler, W., Salize, H. J., Van Os, J., and Riecher- Ro¨ssler, A. (2005). Size of burden of schizophrenia and psychotic disorders. European neuropsychopharmacology, 15(4): 399-409. https://doi.org/10.1016/j.euroneuro.2005.04.009 |
[17, 20]
. At the turn of the twentieth century, Jaspers pioneered the phenomenological technique in psychiatry, providing the framework for empirically-based diagnoses and nosology, which have now pervaded modern classification systems. In low and middle-income countries (LMICs), the focus of the study has been on the treatment gap, the inequities in mental health systems, and scaling up access to medical knowledge and treatment through task shifting
| [17] | Organisation, W. H. et al. (2016). mhgap intervention guide mental health gap action program version 2.0 for mental, neurological and substance use disorders in non- specialized health settings. World Health Organization, pages 1-173. |
[17]
. During the Middle Ages, patients with insanity were imprisoned alongside criminals in dungeons or insane asylums. The most popular forms of treatment were physical punishment and torture. Psychosis and other mental diseases were commonly accused and tried as witches
. Even though most patients have remissions and relapses, psychotic disorders can appear as a single episode of illness; for many patients, the condition becomes chronic and severe. People with mental and psychosocial disabilities face infringement of their civil, cultural, economic, political, and social rights all around the world
| [5] | Drew, N., Funk, M., Tang, S., Lamichhane, J., Cha´vez, E., Katontoka, S., Pathare, S., Lewis, O., Gostin, L., and Saraceno, B. (2011). Human rights violations of people with mental and psychosocial disabilities: an unresolved global crisis. The Lancet, 378(9803): 1664-1675. https://doi.org/10.1016/S0140-6736(11)61458-X |
[5]
. Regardless of income level, human rights violations against people with mental and psychosocial disorders occur in all nations
| [5] | Drew, N., Funk, M., Tang, S., Lamichhane, J., Cha´vez, E., Katontoka, S., Pathare, S., Lewis, O., Gostin, L., and Saraceno, B. (2011). Human rights violations of people with mental and psychosocial disabilities: an unresolved global crisis. The Lancet, 378(9803): 1664-1675. https://doi.org/10.1016/S0140-6736(11)61458-X |
[5]
, including Sierra Leone. People who suffer from severe psychosocial disabilities because of their mental illness face a shared set of challenges that lead to complex demands
| [9] | Harvey, C., Brophy, L., Parsons, S., Moeller-Saxone, K., Grigg, M., and Siskind, D. (2016). People living with psychosocial disability: Rehabilitation and recovery- informed service provision within the second Australian national survey of psychosis. Australian & New Zealand Journal of Psychiatry, 50(6): 534-547. https://doi.org/10.1177/0004867415610437 |
[9]
. Psychosocial disorders, such as schizophrenia, are unquestionably chronic and severe mental illnesses with a substantial global disease burden. It was named one of the top 15 leading causes of disability worldwide in 2016
| [3] | Castillejos, M., Mart´ın-Pe´rez, C., and Moreno-Ku¨stner, B. (2019). Incidence of psychotic disorders and its association with methodological issues. a systematic review and meta- analyses. |
[3]
. Moreover, a psychotic illness characterized by relapses that have substantial consequences for patients’ quality of life, including professional, emotional, and financial burdens on patients and their families
| [22] | Tan, W., Lin, H., Lei, B., Ou, A., He, Z., Yang, N., Jia, F., Weng, H., and Hao, T. (2020). The psychosis analysis in real-world on a cohort of large-scale patients with schizophrenia. BMC Medical Informatics and Decision Making, 20: 1-19. |
[22]
. Persons with these disorders make up a sizable section of the population, with one out of every four people diagnosed with a mental illness worldwide. Furthermore, many people may not meet the medical threshold for mental health disorders but have mental health symptoms that interfere with their daily activities. Psychosocial difficulties commonly coexist with physical health disorders and disabilities, resulting in a more complex disability experience than people who just have mental or physical health issues
| [19] | Ringland, K. E., Nicholas, J., Kornfield, R., Lattie, E. G., Mohr, D. C., and Reddy, M. (2019). Understanding mental ill-health as psychosocial disability: Implications for assistive technology. In Proceedings of the 21st International ACM SIGACCESS Conference on Computers and Accessibility, pages 156-170. https://doi.org/10.1145/3308561.3353785 |
[19]
. Nonetheless, comprehensive care for both physical and psychosocial disability is underdeveloped and understudied. It has been shown that people with mental and psychosocial disorders are often excluded from their communities due to stigma and misinformation. Stigma and discrimination make it difficult for people to work, get out of poverty, and get the treatment and assistance/support they need to integrate or reintegrate into their communities and heal from their illnesses
| [5] | Drew, N., Funk, M., Tang, S., Lamichhane, J., Cha´vez, E., Katontoka, S., Pathare, S., Lewis, O., Gostin, L., and Saraceno, B. (2011). Human rights violations of people with mental and psychosocial disabilities: an unresolved global crisis. The Lancet, 378(9803): 1664-1675. https://doi.org/10.1016/S0140-6736(11)61458-X |
| [15] | Mathias, K., Pant, H., Marella, M., Singh, L., Murthy, G., and Grills, N. (2018). Multiple barriers to participation for people with psychosocial disability in Dehradun district, north India: a cross-sectional study. BMJ open, 8(2): e019443. https://doi.org/10.1136/bmjopen-2017-019443 |
[5, 15]
.
Many Sierra Leoneans have been through traumatic incidents that have been linked to poor mental health. A decade- long civil war that ended in 2002, the 2014 Ebola outbreak, and recurring floods that resulted in a devastating mudslide in August 2017 that killed or left 1141 people missing. Furthermore, alcohol consumption is substantially greater than the area norm, and substance abuse, particularly marijuana and tramadol, is becoming increasingly problematic
| [22] | Tan, W., Lin, H., Lei, B., Ou, A., He, Z., Yang, N., Jia, F., Weng, H., and Hao, T. (2020). The psychosis analysis in real-world on a cohort of large-scale patients with schizophrenia. BMC Medical Informatics and Decision Making, 20: 1-19. |
[22]
. The treatment gap, disparities in mental health systems, and scaling up access to medical knowledge and treatment through task shifting have been the focus of study in low- and middle- income countries (LMICs). While these are crucial factors, the challenges must be viewed in the context of the family, community, and socioeconomic determinants of health, as well as cultural contexts
| [7] | Fernandes, H., Cantrill, S., Kamal, R., and Shrestha, R. (2017). Inclusion of people with psychosocial disability in low and middle income contexts: a practice review. Christian J Global Health, 4(3): 72-81. |
[7]
. The most crippling aspect is the shame that individuals must endure. Because if you are called mentally ill, you lose your work, your access to chances, your integrity in society, and others will treat you negatively. No matter how much you can accomplish, people won’t believe you can. You are so handled as though you don’t even exist. People with psychosocial disabilities have been imprisoned, tortured, confined, and shunned due to the perceived “deviance” associated with psychosocial disability
| [14] | Mahomed, F. (2016). Stigma based on psychosocial disability: A structural human rights violation. South African Journal on Human Rights, 32(3): 490-509. |
[14]
. Many nations lack reliable data about the overall prevalence of disability, and those that have conducted disability-inclusive census surveys may not have adequately or successfully gathered data on psychosocial disability if they have at all. This restricts the ability of development organizations and governments to meet the needs of and gauge the inclusion of individuals with psychosocial disabilities
| [2] | Carroll, A., Davar, B., Eaton, J., Catherine, R., Cambri, J., Devine, A., and Vaughan, C. (2016). Promoting the rights of people with psychosocial disability in development research and programming. Development Bulletin, 77: 25-30. |
[2]
. Based on the above, this study seeks to describe the prevalence of psychosocial disability and unmet need for access and utilization of services in Sierra Leone in addressing the burden of PD.
1.1. Overview of Psychosocial Disability
Historically, prejudices about people with psychosocial disabilities’ entitlement to full citizenship and their capacity to make significant contributions to issues that affect their lives have kept them outside of mainstream society. Participation in political, legal, clinical, and personal decisions that affect the lives of people with psychosocial disabilities has been violated due to prejudiced perceptions that these individuals cannot make reasoned and informed judgements
| [12] | Kleintjes, S., Lund, C., and Swartz, L. (2013). Barriers to the participation of people with psychosocial disability in mental health policy development in south africa: a qualitative study of perspectives of policy makers, professionals, religious leaders and academics. BMC International Health and Human Rights, 13: 1-10. https://doi.org/10.1186/1472-698X-13-17 |
[12]
. All human rights accords, programs, and laws are based on the idea that all people are equal in dignity and have a right to the same fundamental freedoms. One persistent mental condition that can be quite debilitating is schizophrenia. The impairment that comes with it can seriously impair a person’s capacity to interact socially. Of all the illnesses examined, schizophrenia had the highest disability rating in the 2010 Global Burden of Disease study
| [1] | Brooke-Sumner, C., Petersen, I., and Lund, C. (2014). Perceptions of psychosocial disability amongst psychiatric service users and caregivers in south Africa. African Journal of Disability, 3(1): 1-10. |
[1]
. When someone is denied the opportunity to fully exercise their rights because of their country, location of residence, sex, national or ethnic origin, color, religion, language, disability, or any other status, it is discrimination
| [23] | Temple, J. B. and Kelaher, M. (2018). Is disability exclusion associated with psychological distress? Australian evidence from a national cross-sectional survey. BMJ open, 8(5): e020829. https://doi.org/10.1136/bmjopen-2017-020829 |
[23]
. According to the 2010 Global Burden of Disease survey, mental illness was the main factor contributing to years spent disabled, and the majority of those affected were residents of low- and middle-income countries (LMIC). The term “psychosocial disability” describes individuals who have been diagnosed with a mental illness or who have recognized that they have difficulties engaging in basic psychological and social activities. Additionally, individuals who have experienced the negative social effects of psychological or social disability, such as exclusion and discrimination, are included in this category
| [15] | Mathias, K., Pant, H., Marella, M., Singh, L., Murthy, G., and Grills, N. (2018). Multiple barriers to participation for people with psychosocial disability in Dehradun district, north India: a cross-sectional study. BMJ open, 8(2): e019443. https://doi.org/10.1136/bmjopen-2017-019443 |
[15]
. Even while mental and physical illnesses sometimes coexist, the systems that provide social services and treatment for mental and physical illnesses are distinct. As a result, alternatives for both mental and physical health care are sometimes fragmented and separated from one another, making it possible for someone to receive treatment for a physical ailment but not a mental one
| [19] | Ringland, K. E., Nicholas, J., Kornfield, R., Lattie, E. G., Mohr, D. C., and Reddy, M. (2019). Understanding mental ill-health as psychosocial disability: Implications for assistive technology. In Proceedings of the 21st International ACM SIGACCESS Conference on Computers and Accessibility, pages 156-170. https://doi.org/10.1145/3308561.3353785 |
[19]
. Psychosocial disability has been conceptualized in diverse ways: from a continuum of tension, stress and distress, to a biomedical understanding associated with mental health conditions including schizophrenia, bipolar disorder, depression and substance misuse. In this paper, the term ‘psychosocial disability’ has been used to refer to people who self-identify and/or have received a diagnosis of a mental health condition and who have experienced negative social effects including prejudice and discrimination and, in many cases, negative impacts from interactions with health and justice systems
| [2] | Carroll, A., Davar, B., Eaton, J., Catherine, R., Cambri, J., Devine, A., and Vaughan, C. (2016). Promoting the rights of people with psychosocial disability in development research and programming. Development Bulletin, 77: 25-30. |
[2]
. Individuals who suffer from psychosocial disabilities must choose whether to reveal their status. Nonetheless, not much research has been done on this conundrum. Making this decision is difficult because there could be advantages and disadvantages. Students who wish to request a reasonable accommodation because of their impairment must, like students with other disabilities, disclose their psychosocial disability to their educational institutions. When compared to peers without disabilities, university students with psychosocial difficulties have a significantly higher dropout rate and typically perform worse academically
| [24] | Vergunst, R. and Swartz, L. (2021). ‘He doesn’t understand that he’s struggling with the way I felt’- university students, psychosocial disability and disclosure in the western cape, south africa. Disability & Society, 36(2): 226-239. |
[24]
.
1.2. Prevalence of PD
These days, psychological problems like stress, worry, and depression are more common. It was discovered that over 450 million people worldwide suffered from mental health issues. Mental health disorders are becoming more widely acknowledged as a serious public health concern that has an impact on physical health and has a variety of social and economic ramifications. To lower the mortality and morbidity associated with mental illness, the Mental Health Action Plan 2013-2020 promoted four main goals: effective leadership and governance for mental health; the provision of comprehensive mental health and social care services in community-based settings; the implementation of promotion and prevention strategies; and the strengthening of information systems, evidence, and research. The National Health and Morbidity Survey 2015 in Malaysia found that mental health issues impact one in three persons (29.2%), an increase from the 10.7% prevalence rate in 1996
| [11] | Ismail, M., Lee, K. Y., Sutrisno Tanjung, A., Ahmad Jelani, I. A., Abdul Latiff, R., Abdul Razak, H., and Ahmad Shauki, N. I. (2021). The prevalence of psychological distress and its association with coping strategies among medical interns in Malaysia: A national- level cross-sectional study. Asia-Pacific Psychiatry, 13(2): e12417. https://doi.org/10.1111/appy.12417 |
[11]
. Unfounded presumptions about the aptitude and potential of people with psychological disabilities, as well as the general debate surrounding the causes of mental impairment, frequently contribute to discrimination and the exclusion that follows. The degree of disability caused by mental health issues varies depending on how long they last and how frequently they relapse and remit. It’s crucial to remember that not everyone with a mental health diagnosis would be seen as having a psychosocial disability, identify as such, or adhere to the medical paradigm of mental disease or impairment
| [2] | Carroll, A., Davar, B., Eaton, J., Catherine, R., Cambri, J., Devine, A., and Vaughan, C. (2016). Promoting the rights of people with psychosocial disability in development research and programming. Development Bulletin, 77: 25-30. |
[2]
. Mental disease develops because of a variety of causes, including biological, psychological, socioeconomic, and lifestyle factors. High job demand, little job control, and inadequate work support are examples of occupation- related characteristics that have been connected to detrimental consequences on one’s physical and mental health, including exhaustion, anxiety, and depression. Due to their lengthy work hours and heavy patient load, healthcare professionals (HCPs) in medical practice are more likely to experience stress, anxiety, and depression. In extreme circumstances, some people may even turn to drug addiction and abuse. According to research, stress, anxiety, and depression were prevalent among interns; the incidence of these illnesses was significantly higher among female and younger interns (29.7%, 39.9%, and 26.2%, respectively). Of these, 75.1% employed problem-focused solutions as their primary coping mechanism. While avoidance-based coping methods were strongly correlated with all three of these outcomes, emotion- focused coping strategies only displayed a slight but significant correlation with stress, anxiety, and depression
| [11] | Ismail, M., Lee, K. Y., Sutrisno Tanjung, A., Ahmad Jelani, I. A., Abdul Latiff, R., Abdul Razak, H., and Ahmad Shauki, N. I. (2021). The prevalence of psychological distress and its association with coping strategies among medical interns in Malaysia: A national- level cross-sectional study. Asia-Pacific Psychiatry, 13(2): e12417. https://doi.org/10.1111/appy.12417 |
[11]
.
1.3. Need for Individuals with and Without PD
Unmet needs are those in a specific area of a person’s life where there is either no support available or insufficient support offered. Unmet requirements are multifaceted and vary depending on a person’s living situation, disease severity, and demographic traits
| [16] | Minyo, M. J. and Judge, K. S. (2022). Perceived unmet need and need-related distress of people living with dementia. Gerontology and Geriatric Medicine, 8: 23337214221092886. https://doi.org/10.1177/23337214221092886 |
[16]
. People with mental illnesses and related psychosocial disabilities are among the most marginalized groups in society all around the world. The phrase “psychological disabilities,” which is increasingly extensively used in the disability movement, refers to disabilities that result from obstacles to social engagement faced by those who have or are thought to have mental health issues
| [6] | Eaton, J., Carroll, A., Scherer, N., Daniel, L., Njenga, M., Sunkel, C., Thompson, K., Kingston, D., Khanom, G. A., and Dryer, S. (2021). Accountability for the rights of people with psychosocial disabilities: an assessment of country reports for the convention on the rights of persons with disabilities. Health and human rights, 23(1): 175. |
[6]
. Actual or perceived impairment brought on by a range of mental, emotional, or cognitive experiences is referred to as psychosocial disability. In comparison to people who just have mental or physical health issues, people with psychosocial disabilities also typically co-occur with physical health disorders and disabilities. This co-occurrence might result in a more complex disability experience. Individuals with these disabilities also represent a sizable portion of the population, with 1 in 4 people diagnosed with a mental health condition worldwide. Furthermore, many people may not meet the medical “threshold” for mental health conditions but may still find their daily living activities impaired by mental health symptoms. Anxiety, depression, and many other mental health concerns can be classified as psychosocial disabilities, recognizing the actual or perceived impairment these concerns produce in daily life
| [19] | Ringland, K. E., Nicholas, J., Kornfield, R., Lattie, E. G., Mohr, D. C., and Reddy, M. (2019). Understanding mental ill-health as psychosocial disability: Implications for assistive technology. In Proceedings of the 21st International ACM SIGACCESS Conference on Computers and Accessibility, pages 156-170. https://doi.org/10.1145/3308561.3353785 |
[19]
. Research shows that psychologically distressed individuals often have unmet mental health needs. These criteria may include serious dysfunction in day-to-day functioning as well as issues with substance addiction, anxiety, or hopelessness. According to studies carried out by
| [16] | Minyo, M. J. and Judge, K. S. (2022). Perceived unmet need and need-related distress of people living with dementia. Gerontology and Geriatric Medicine, 8: 23337214221092886. https://doi.org/10.1177/23337214221092886 |
[16]
on clinically assessed and perceived unmet mental health needs, health care use, and barriers to care for mental health problems in a Belgian general population sample, a significant portion of people who experience psychological distress do not seek or receive appropriate mental health care, which results in unmet needs in this population.
1.4. Barriers/Limitations to Access and Utilization of PD Services
At every stage of life, the availability of healthcare services has a noteworthy influence on general health. When healthcare services are used to their full potential, health issues can be identified and diagnosed earlier and treated more aggressively. Positive impacts on chronic illness and life expectancy follow from this. Most healthcare systems globally prioritize reducing obstacles to healthcare accessibility for their populace; nonetheless, numerous obstacles methodically impede the achievement of this goal. Several noteworthy obstacles include the insufficiency of accessibility, affordability, or physical availability of services. More complexity arises from the fact that “access” has not been uniformly defined within or across health systems, which frequently influences policy without considering all pertinent factors. Access is based on a range of factors, all of which must be considered to assess an individual’s level of access appropriately. This entails integrating features of health systems, organizations, and healthcare providers with features of people, homes, and social and physical settings. It encompasses both supply and demand elements with the goal of meeting healthcare demands
| [4] | Coombs, N. C., Meriwether, W. E., Caringi, J., and Newcomer, S. R. (2021). Barriers to healthcare access among us adults with mental health challenges: A population-based study. SSM-population health, 15: 100847. https://doi.org/10.1016/j.ssmph.2021.100847 |
[4]
. People with psychological disabilities are increasingly acknowledged as a marginalized minority that has endured ongoing abuse of their human rights during the past ten years. Historically, the majority of low- and middle-income countries’ (LMIC) disability and development movements, as well as their health agendas, have excluded people with psychological disabilities. The most significant obstacle to inclusion is the widespread discrimination and negative attitudes toward psychosocial disabilities. When combined with other obstacles such as physical, informational, socioeconomic, and legal, this leads to exclusion in all spheres of development, including health, education, and livelihoods, social inclusion, legal capacity, and the limitation of civil and political rights, including the ability to participate in the development of mental health policies. International development actors are becoming more aware of the necessity of making focused effort to remove barriers and discrimination so that individuals with psychosocial disabilities can participate in and benefit from development initiatives
| [2] | Carroll, A., Davar, B., Eaton, J., Catherine, R., Cambri, J., Devine, A., and Vaughan, C. (2016). Promoting the rights of people with psychosocial disability in development research and programming. Development Bulletin, 77: 25-30. |
[2]
. According to
| [2] | Carroll, A., Davar, B., Eaton, J., Catherine, R., Cambri, J., Devine, A., and Vaughan, C. (2016). Promoting the rights of people with psychosocial disability in development research and programming. Development Bulletin, 77: 25-30. |
[2]
, the “first comprehensive and legally binding international framework for psychosocial disability” was the United Nations Convention on the Rights of Persons with Disability (CRPD), which offered a framework for analyzing the conditions that facilitate or impede the inclusion of individuals with psychosocial disabilities in development policies and programs. Even while some nations have seen improvements since the CRPD was adopted, several issues still make it difficult to include people with psychosocial disabilities in development
| [2] | Carroll, A., Davar, B., Eaton, J., Catherine, R., Cambri, J., Devine, A., and Vaughan, C. (2016). Promoting the rights of people with psychosocial disability in development research and programming. Development Bulletin, 77: 25-30. |
[2]
. One major cause of exclusion is discrimination and ignorance about psychosocial disabilities. Human rights violations suffered by individuals with psychosocial disabilities include being detained against their will in their homes, communities, or institutions, as well as being neglected during times of distress or crisis. Although it is often known that negative attitudes are the main obstacle to the inclusion of individuals with psychosocial disabilities, there is little research on the effectiveness of techniques for changing attitudes and minimizing exclusion and discrimination. The rights mentioned in the CRPD are still in conflict with numerous laws and practices. In certain cases, mental health laws may even work to restrict the rights of those who suffer from psychosocial disabilities. Lack of “legal capacity” can prevent people from exercising their right to “associate,” hinder the formation of self-help organizations, and, in certain cases, foster an atmosphere in which people are too scared to speak up or stand up for themselves for fear of facing consequences from the law. People with psychosocial disabilities who experience persistent exclusion are more likely to become impoverished. On the other hand, social injustice, poverty, violence, and limited access to social and medical services raise the likelihood of poor mental health and the susceptibility of those with psychosocial disabilities. People with distinct kinds of disabilities have varying employment rates; those with intellectual and/or psychosocial disabilities have the lowest rates. Comparing people with disabilities to those without, early studies revealed that ninety per cent of those with psychosocial disabilities were unemployed
| [2] | Carroll, A., Davar, B., Eaton, J., Catherine, R., Cambri, J., Devine, A., and Vaughan, C. (2016). Promoting the rights of people with psychosocial disability in development research and programming. Development Bulletin, 77: 25-30. |
[2]
. Getting and using help for psychological discomfort may be difficult when there are limitations and restrictions. These barriers may keep people from seeking the proper care for their mental health issues or from asking for assistance. Language and cultural barriers, financial constraints, limited access to resources, treatment anxiety, a dearth of social support, and stigma are a few typical roadblocks
| [4] | Coombs, N. C., Meriwether, W. E., Caringi, J., and Newcomer, S. R. (2021). Barriers to healthcare access among us adults with mental health challenges: A population-based study. SSM-population health, 15: 100847. https://doi.org/10.1016/j.ssmph.2021.100847 |
[4]
.
2. Methodology
2.1. Study Design
The researcher used a cross-sectional study design and analytic by type. The cross-sectional design was used to describe the factors influencing the delivery of quality healthcare at the Makeni regional. A cross-sectional study is an example of an observational study design. In a cross-sectional study, the researcher looks at data at a particular point in time. The participants are only chosen based on the inclusion and exclusion criteria established for the investigation. Cross-sectional designs are used for population-based surveys and provide a 1-time measurement of the prevailing characteristics of a population. Although a cross-sectional study cannot establish cause and effect, it can efficiently identify potential correlations at a specific point in time. Descriptive research studies aim to collect accurate and relevant data about how a problem or phenomenon is currently manifesting, providing insights into its characteristics and, where appropriate, informing broader inferences based on the study’s design and sampling. A descriptive research design was chosen because it allows data collection without altering the environment, aligning with the research goals of observing the phenomenon in its natural context.
2.2. Study Location and Population
Sierra Leone is located on Africa’s west coast, bordered by Liberia and Guinea and flanked by the Atlantic Ocean. 7,092,113 people (50.8% female, 40.8% 15 years, 41% urban, 51% literacy, 78% Muslim) make up the country’s young and quickly rising population. The country is divided into 16 districts, the most populous of which is the Western Area Urban District (Freetown), which has 1.1 million residents. Sierra Leone is divided into 20 dialects, each with its own set of cultural beliefs and behaviors. More than half of Sierra Leoneans (52.9%) live in poverty
| [8] | Harris, D., Endale, T., Lind, U. H., Sevalie, S., Bah, A. J., Jalloh, A., and Baingana, F. (2020). Mental health in sierra leone. BJPsych International, 17(1): 14-16. https://doi.org/10.1192/bji.2019.17 |
[8]
. Specifically, the research will be conducted in Makeni which is the largest city in the northern province of Sierra Leone. This study will involve residents in Bombali district. Bombali has a population of 605,741
| [10] | Isiaka Jimmy, A., Anarfi Boateng, K., Twum, P., Larbie, D., Bangura, A., Milton Conteh, H., and Agyei-Baffour, P. (2021). Population characteristics and their implications on the benefit basket of national social health insurance scheme in sierra leone: A prospective view. Advances in Public Health, 2021(1): 5522384. https://doi.org/10.1155/2021/5522384 |
| [13] | Leone, S. S. (2017). Sierra Leone 2015 population and housing census thematic report on Agriculture. |
| [18] | Peters, K. (2015). Sierra Leone. In Africa Yearbook Volume 11, pages 158-163. Brill. |
[10, 13, 18]
. The inclusion and exclusion criteria are: you should be within the age bracket of 15 years and above.
2.3. Sampling and Sampling Technique
The Yamane formula was used for attaining the sample size for the quantitative part of this study (95% confidence level and 0.08 Margin of error). The formula for calculating the sample size is given by:
where:
n: Sample size
N: Study population
e: Margin of error
2.4. Example Calculation
Example Calculation
For a study population N = 605741 and a margin of error e = 0.08, the sample size is calculated as follows:
(2)
(3)
Therefore, at 95 percent confidence level and 0.08 precision rate, the sample size for this study is 156. A probability sampling technique (balloting without replacement) was used for this study. Using probability proportion to size sampling is an approach that is useful when the units are of unequal sizes and ensures the likelihood of a unit being selected is proportionate to the size of the represented population.
2.5. Data Collection
Data collection for this will be attained with the use of structured questionnaire and for the psychological distress component, the K10 scale which is a screening tool for both severe and common mental disorders will be use. Research assistants were trained in how to administer the questionnaire and data collection procedures. Successive study participants were identified by the principal researcher following the inclusion and exclusion criteria. Following the selection of the responders, each study participant was given a personalized explanation of the study in a language they could understand preferably Krio.
2.6. Data Analysis
Statistical packages such as STATA V.14.0 was used to conduct the statistical analysis. To investigate the relationship between psychosocial disability and socio-demographic factors, logistic regression was used to obtain crude and adjusted Odd Ratios. The met and unmet needs of PD individuals were assessed using descriptive statistics. Furthermore, findings for the study will be presented in the form of tables and graphs. The initial phase of data management encompasses thorough data cleaning procedures. This involves a meticulous review of the dataset to identify and rectify any missing data or inconsistencies. By addressing these issues, the dataset’s quality and integrity are upheld, ensuring the reliability of subsequent analyses. Following data cleaning, a systematic coding process was implemented. This entails assigning appropriate codes or labels to variables and responses, creating a structured and organized dataset. The coded data facilitates streamlined and efficient analysis, enabling the research team to draw meaningful insights from the information collected during the study. To transition from paper-based questionnaires to a digital format, a comprehensive data entry process was undertaken. This ensures that the data was accurately and securely transferred, minimizing the risk of errors associated with manual entry. The subsequent analytical phase involves summarizing and describing the demographic characteristics of the study population. Descriptive statistics, such as frequency distributions, percentages and chi-square, are calculated for variables related to PD. These statistical measures provide a clear overview of the central tendencies and distributions within the dataset, aiding in the interpretation of key findings.
3. Findings
3.1. Socio-demographic Characteristics
In the table below, the socio-demographic characteristics of the respondents for this research is presented. The total number of respondents is equal to one hundred and fifty-six (156). Most respondents are aged 18-24, with a smaller percentage falling into the 25-34 age group, 35-44 age group, and older age groups. The gender distribution is slightly more women than men. A higher percentage are currently enrolled in school, while the rest do not attend. Many respondents belong to the middle class, with the poor and wealthy closely following. A substantial fraction is married or single, with separated/divorced/widowed making up a smaller percentage.
Table 1. Socio-demographic Characteristics of the Respondents.
Variable Frequency | (n=156) | Percentage (%) |
Age of respondent |
18 - 24 years | 40 | 25.64 |
25 - 34 years | 26 | 16.67 |
35 - 44 years | 32 | 20.51 |
45 - 54 years | 29 | 18.59 |
55 years and above | 29 | 18.59 |
Gender of Respondents |
Female | 83 | 53.21 |
Male | 73 | 46.79 |
Schooling |
No | 70 | 44.87 |
Yes | 86 | 55.13 |
Socioeconomic status of Respondents |
Poor | 45 | 28.85 |
Middle | 91 | 58.33 |
Rich | 20 | 12.82 |
Marital status of Respondents |
Single | 60 | 38.46 |
Married | 65 | 41.67 |
Separated/divorced/widowed | 31 | 19.87 |
Occupation of Respondents |
Employed | 52 | 33.33 |
Unemployed | 35 | 22.44 |
Others | 69 | 44.23 |
3.2. Prevalence of PD (Using Kessler Psychological Distress Scale (K10)
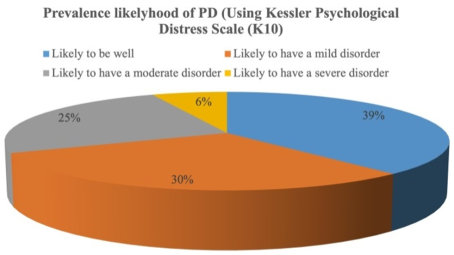
According to the K10 model of the psychological distress scale, the
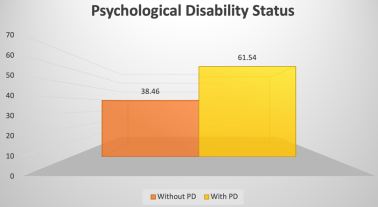
Figure 1 below shows that 39% of the respondents were likely to be well, 30% of them were likely to have a mild disorder, 25% were likely to have a moderate disorder and the remaining 6% were likely to have a severe disorder. In summary, as is presented in
Figure 2, the findings show that more than half of the respondents were discovered to be psychologically distressed.
Figure 1. Prevalence likelihood of PD (Using Kessler Psychological Distress Scale - K10).
Figure 2. Psychological Disability Status (with and without PD).
Furthermore, the table below shows the cross-tabulation (Chi-square analysis) of PD by a few demographic characteristics to ascertain any relationship. The analysis (with a P-value ¡ 0.05), shows that there is a significant relationship between the likelihood of having a PD and that of socioeconomic status (P-value=0.003), and Occupation (P-value=0.001) of respondents.
Table 2. Chi-square analysis between Prevalence of Psychological Distress and Demographic indicators.
Prevalence of Psychological distress (PD) | Gender of respondents | P-value | Socioeconomic status of Respondents | P-value | Occupation of Respondents | P-value |
Female | Male | Poor | Middle | Rich | Employed | Unemployed | Others |
Likely to be well | 34 | 26 | 0.089 | 22 | 34 | 4 | 0.003* | 18 | 10 | 32 | 0.001* |
21.79 | 16.67 | | 14.1 | 21.79 | 2.56 | | 11.54 | 6.41 | 20.51 | |
Likely to have a mild disorder | 30 | 17 | | 11 | 28 | 8 | | 21 | 16 | 10 | |
19.23 | 10.9 | | 7.05 | 17.95 | 5.13 | | 13.46 | 10.26 | 6.41 | |
Likely to have a moderate disorder | 15 | 24 | | 9 | 27 | 3 | | 9 | 4 | 26 | |
9.62 | 15.38 | | 5.77 | 17.31 | 1.92 | | 5.77 | 2.56 | 16.67 | |
Likely to have a severe disorder | 4 | 6 | | 3 | 2 | 5 | | 4 | 5 | 1 | |
2.56 | 3.85 | | 1.92 | 1.28 | 3.21 | | 2.56 | 3.21 | 0.64 | |
3.3. Interpretation of the Chi-Square
The p-value for gender = 0.089 suggests that there is no statistically significant correlation between the gender of respondents and the occurrence of psychological distress. Stated differently, the data analyzed has not demonstrated a significant difference in psychological distress between the sexes, which are male and female. This result has not demonstrated the much-needed significance of the relationship between gender and psychological distress that is because of factors such as cultural effects, sample size, or the tools employed to assess psychological distress.
3.4. Economic Status and Psychological Distress
With a p-value for economic status = 0.003, the results demonstrate a statistically significant relationship between the prevalence of psychological distress and socioeconomic position. This implies that people from different socioeconomic origins may feel psychological distress to varying degrees. This research has demonstrated that a person’s psychological distress is directly associated with their socioeconomic status. Differences in stressor exposure, social support networks, healthcare facilities, and resource availability are linked with disparities in socioeconomic position. An individual’s socioeconomic status has a major impact on their psychological distress. Several significant factors can explain the relationship between psychological distress and socioeconomic status. Greater socioeconomic position frequently corresponds to greater access to services like education, first-class healthcare, and social support networks. These resources are crucial for promoting mental wellness and preventing stress. However, those with lower socioeconomic positions may find it difficult to access these facilities, which puts them at a higher risk of psychological distress. Challenging situations in life such as lower socioeconomic position are typically associated with exposure to more stressful living conditions, such as financial difficulties, unstable housing arrangements, and fewer opportunities for social mobility. These constant pressures may result in psychological distress and mental health challenges. Socioeconomic position can also impact psychosocial components like social status, self-worth, and a sense of control over one’s life. Reduced financial status can worsen psychological distress by causing emotions of helplessness and social alienation. Social aspects that affect health could be another risk factor. Numerous aspects of a person’s life, including their living situation, career opportunities, and accessibility to social support networks, influence their socioeconomic status. It is an important social determinant of health. Variations in the outcomes linked to mental health may arise from unequal opportunities and resource allocation brought about by differences in socioeconomic status. Prolonged exposure to socioeconomic inequalities can eventually result in poor mental health and chronic stress. Socioeconomic position often has a cumulative effect on psychological pain. The importance of addressing socioeconomic disparities at an early age to prevent long-term repercussions on mental health is highlighted by this compounding effect. In summary, socioeconomic status influences psychological distress in a variety of ways. These include being in stressful situations, having resources available, socioeconomic determinants of health, psychosocial aspects, and long-term cumulative effects. It is necessary to address socioeconomic disparities and ensure fair access to opportunities and resources to mitigate the impact of these disparities on psychological discomfort.
3.5. Occupation (p-value = 0.001)
In the table above the statistical significance of the relationship between the work of the respondents and the frequency of psychological distress is demonstrated by the p-value of 0.001. This implies that the type of work that people do can have a considerable influence on their psychological well-being. The strong correlation seen between occupation and psychological distress could be explained by factors such as job-related stress, workplace features, job insecurity, or demands specific to a given profession that affect mental health outcomes. Furthermore, a person’s occupation can greatly impact their psychological discomfort due to several factors unique to diverse types of jobs. Certain jobs include a lot of pressure, stress, and responsibilities, which can hasten the onset of psychological anguish. A lack of social support, low income, low status, high job expectations mixed with insufficient control over work procedures, or any combination of these factors may increase the risk of mental health problems. These components are commonly included in the Job-Demand- Control-Support Model, which highlights the need to create a balance between job demands, control, and support in the workplace. In Longitudinal Studies, Research has shown that workers in high-risk occupations are more likely to experience psychological discomfort than workers in low- risk occupations. Longitudinal studies have demonstrated that in high-risk occupations, distress levels increase with the duration of service, showing a cumulative impact of occupational exposures on mental health. There is a correlation between little social support, high job demands, limited control over work, and psychological suffering at work. Research indicates that workers in regulated fields have less psychological distress than workers in unregulated fields. This is particularly true for regulated professions, where law by professional groups sets titles and practices. This suggests that the regulatory framework and standards set by professional associations may affect lowering the prevalence of mental health issues among workers in these industries. People’s psychological distress is greatly influenced by their workplace conditions. Numerous elements, such as the application of skills, psychological demands, job insecurity, and social support at work, can have an impact on mental well-being. Positive features like skill usage and social support have been linked to lower levels of distress, while negative aspects like low social support and high job demands may raise the chance of psychological discomfort.
3.6. Needs of Individuals with and Without PD
The study comparing the needs of individuals with and without psychological distress (PD) reveals that 65.38% of PD patients have their work access needs met, while 34.62% do not. Medical care needs were met by 77.56% of PD patients, while 45.51% believe their needs have been met. Social activities were met by 60.26% of PD patients, while 60.49% disagreed. Access to safe drinking water and sanitation was satisfactory by 75.64% of PD patients. Religious needs were addressed by 82.05% of PD patients, while 52.56% believed their needs were met in rehabilitation services. The percentages of met needs and unmet requirements for assistive equipment and legal aid were comparable, with 50% reporting equal rates and 50% reporting unmet needs. Disaster management needs were met by a smaller percentage of respondents. The research shows that psychological distress patients’ desire for fulfilment varies across diverse groups, with gaps in areas like disaster management, religion, and safe drinking water, indicating varying levels of fulfilment.
Table 3. Needs of individuals with and without PD.
Variable | Frequency (n=156) | Percentage (%) |
Access to Work |
Met need | 102 | 65.38 |
Unmet need | 54 | 34.62 |
Healthcare Service |
Met need | 121 | 77.56 |
Unmet needs | 35 | 22.44 |
Community consultations |
Met need | 71 | 45.51 |
Unmet need | 85 | 54.49 |
Social activities |
Met need | 94 | 60.26 |
Unmet need | 62 | 39.74 |
Sanitation |
Met need | 116 | 74.36 |
Unmet need | 40 | 25.64 |
Safe drinking water |
Met need | 118 | 75.64 |
Unmet need | 38 | 24.36 |
Religion |
Met need | 128 | 82.05 |
Unmet need | 28 | 17.95 |
Rehabilitation services |
Met need | 82 | 52.56 |
Unmet need | 74 | 47.44 |
Legal assistance |
Met need | 78 | 50 |
Unmet need | 78 | 50 |
Assistive devices |
Met need | 77 | 49.36 |
Unmet need | 79 | 50.64 |
Disaster management |
Met need | 58 | 37.18 |
Unmet need | 98 | 62.82 |
3.7. Barriers to Access and Utilization of PD Services
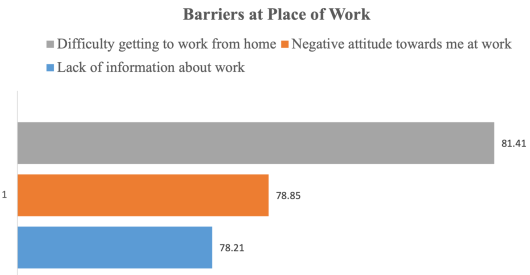
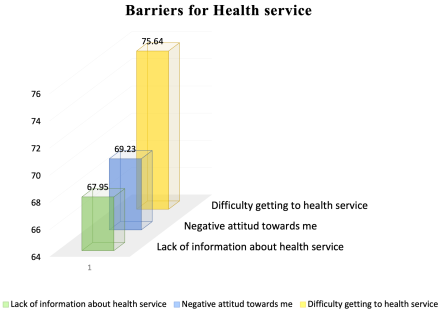
These barriers are presented into distinct categories, on the issue of access and use of community services based on a multiple choice. As per the data, a considerable proportion of participants (60.3%) reported difficulties in obtaining family support during their need for help, whereas 39.7% reported no difficulties. In this instance, 78.2% of respondents claimed that their insufficient job knowledge was a difficulty, whereas just 21.8% did not encounter this barrier. Similarly, a considerable proportion (78.9%) reported experiencing negative attitudes towards them at work, compared to 21.1% who did not experience this problem. The majority (81.4%) of respondents to the study said that they had this difficulty when traveling from home to work, compared to just 18.6% who did not. A sizable percentage (67.9%) of respondents reported having issues with health services because of their lack of understanding, whereas 32.1%. A significant percentage of those who sought health services (69.2%) said they encountered negative attitudes toward them, whereas just 30.8% did not encounter such behavior. Furthermore, the data reveals that while 75.6% of individuals had no difficulties receiving healthcare, just 24.4% of people reported having no trouble at all. The information provided is the result of many challenges people have while attempting to use services and resources provided by the community, with a focus on community consultation. The data show that a sizable proportion of respondents (73.08%) think there is a lack of information on community consultation, whereas a smaller percentage (26.92%) do not think this is an issue. In this case, 32.69% of respondents claimed not to have experienced a negative attitude, but most respondents (67.31%) claimed to have. Of those who said they were having difficulties travelling from home to community gatherings, 65.38% said they were having difficulties, while 34.62% said they were not. The study indicates that a significant percentage (61.54%) feel they do not know enough about programs for rehabilitation; this is a concern not shared by the rest 38.46%). The majority (63.46%) reported having self-defeating thoughts during their recovery treatment. Similar to social events, a considerable proportion (65.38%) had difficulties obtaining home rehabilitation assistance. The majority, (71.79%) expressed concern about the lack of awareness of safe drinking water. A significant percentage (64.1%) reported having formed negative thoughts about clean drinking water. A significant percentage (70.51%) reported having problems accessing pure drinking water from their homes. The research result shows how people react to various challenges that they face when engaging in social activities. These barriers have to do with ignorance, negative feelings about them, and difficulties traveling from home to social settings. Most respondents (59.62%) said that not knowing enough about social events is one of their main challenges. This suggests that enhanced communication and promotion may be necessary for social events and gatherings to ensure greater involvement and inclusivity. A significant majority of respondents (60.9%) stated that negative feelings about them discouraged them from engaging in social activities. This highlights how important it is to foster a more hospitable and inclusive environment in social circles to encourage participation from all individuals. The overwhelming majority (66.67%) said they had problems traveling from their homes to areas of social interaction. This can suggest that to motivate more individuals to take part in social events, accessibility or transportation infrastructure must be improved. The information also addresses concerns about barriers that individuals have when practicing their religion, such as ignorance, animosity, and difficulty traveling from home to places of worship. A significant issue expressed by a considerable number of respondents (68.59%) was ignorance about religious practices. This highlights how important it is for religious organizations to communicate openly to inform their members of the variety of services and activities that are available to them. A significant percentage (67.95%) reported that they have experienced antagonism in religious environments.
Addressing stereotypes and encouraging acceptance is crucial in religious settings to create an environment that welcomes all participants. The majority (69.23%) spoke of the challenges they had traveling from their homes to places of worship. Improving transportation accessibility or providing alternatives might help overcome this barrier and boost religious activity participation. Responses to this poll were gathered about the challenges people had while trying to use government social assistance programs, such as informational gaps, negative attitudes, and challenging entrance points. A substantial portion of respondents (64.1%) cited ignorance about government social services as one compelling cause. Enhancing lines of communication and launching public awareness initiatives might help resolve this issue and ensure that people are aware of the options at their disposal. 62% of respondents claimed that when they asked for government social assistance programs, they were met with hostility from others. Building empathy and understanding among caregivers is essential to creating a welcoming environment for those who require assistance. Many (60.26%) reported difficulty accessing government- funded social assistance programs. Streamlining service delivery processes or offering mobile outreach programs might help reduce this barrier and improve access for underprivileged populations. 67.95 percent of respondents, a sizable chunk of the sample, cited ignorance of Disabled Person Organizations (DPO) services as a barrier, according to the statistics. For better serving the needs of people with disabilities, it is imperative that information about the services offered by DPOs be widely known and easily accessible. Significantly influencing their desire to interact with DPOs is the alarming discovery that 62.18% of respondents said they encountered unfavorable views about them. Encouraging inclusivity and support for people with disabilities requires addressing and countering these negative beliefs. Additionally, 65.38% of the respondents find it difficult to go from their residences to DPO locations. This emphasizes how accessible DPO services must be for everyone, which calls for better transportation choices or other arrangements. Comparable to the dearth of knowledge regarding DPO services, a sizable percentage (62.18%) mentioned that one obstacle was the dearth of knowledge regarding education or training. Improving means of communication and resources for learning can enable people with disabilities to pursue their educational or professional goals. According to 61.54% of respondents, there is a high frequency of unfavorable attitudes toward disabled people in educational settings. This suggests discriminatory practices exist, which impede the development of inclusive learning environments. Raising awareness and providing sensitivity training helps lessen these prejudices and improve the climate in classrooms. Furthermore, a sizable portion (62.18%) encounter difficulties getting to training or educational facilities because of physical or transportation limitations. Enhancing facilities and accommodations can help ensure that people with disabilities have equal opportunities to engage in educational programs.
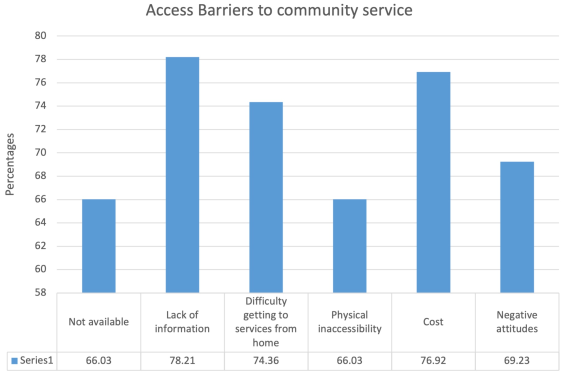
Figure 3. Access Barriers to Community Service.
Figure 4. Barriers at Place of Work.
Figure 5. Barriers for Health Service.