Post- myocardial infarction ventricular septal rupture is a rare but very fatal complication if early and appropriate management is not provided or is delayed. Despite medical advances in treatment, the mortality rate associated with ventricular septal rupture following myocardial infarction remains very high. We report the case of a 65-year-old woman with a history of alcohol abuse, hospitalized in the cardiology department of Kara Teaching Hospital for an anteroseptal ST elevation myocardial infarction that was not treated with thrombolysis. The patient's condition was marked by the occurrence of a ventricular septal rupture on the third day, followed by death on the fourth day, without surgical repair of the septum. This case illustrates the severity of the mechanical complications of myocardial infarction. The lack of cardiac surgery in Togo constitutes a fatal obstacle to the management of certain cardiac pathologies, such as post-myocardial infarction ventricular septal rupture. Hence the need to improve the local technical platform to ensure better patient care.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Post- myocardial infarction ventricular septal rupture is a rare but serious complication, as it is life-threatening if early and appropriate treatment is not provided or is delayed. This ventricular septal rupture occurs at the junction between healthy and infarcted tissue
[1]
Crenshaw BS, Granger CB, Birnbaum Y, Pieper KS, Morris DC, Kleiman NS, et al. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction: GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators. Circulation. 2000 Jan 4-11; 101(1): 27-32.
[2]
Menon V, Webb JG, Hillis LD, Sleeper LA, Abboud R, Dzavik V, et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: a report from the SHOCK Trial Registry: Should we emergently revascularize Occluded Coronaries in cardiogenic shock? J Am CollCardiol. 2000; 36(3): 1110-6. PubMed | Google Scholar.
[1, 2]
. It is an extreme medical-surgical emergency requiring multidisciplinary management involving emergency physicians, cardiologists, and cardiovascular surgeons
[3]
Asmaa Ameur, Rim Raissouni, Houda Souilk, Chaimae Rhemimet et coll. Post-myocardial infarction ventricular septal defect: a case report and literature review. Int. J. Adv. Res. 2023 feb; 11, 2: 155-9.
[3]
. Before the era of thrombolysis, the reported incidence of post-myocardial infarction septal rupture was 11% in histopathological series and 1 to 2% of patients hospitalized for myocardial infarction. Today, the incidence rate is 0.2%, thanks to various early recanalization techniques
[1]
Crenshaw BS, Granger CB, Birnbaum Y, Pieper KS, Morris DC, Kleiman NS, et al. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction: GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators. Circulation. 2000 Jan 4-11; 101(1): 27-32.
[2]
Menon V, Webb JG, Hillis LD, Sleeper LA, Abboud R, Dzavik V, et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: a report from the SHOCK Trial Registry: Should we emergently revascularize Occluded Coronaries in cardiogenic shock? J Am CollCardiol. 2000; 36(3): 1110-6. PubMed | Google Scholar.
[1, 2]
. Despite medical advances in management, the mortality rate associated with ventricular septal defects following myocardial infarction remains very high exceeding 90% without surgical or interventional treatment
[4]
Kalyani R, Trivedi A, Philippe Aldebertb, Alberto Riberi C, Julien Mancinid E, Gilles Levyf, Jean-Christophe Maciag, Jacques Quilicci C, Gilbert Habibc, Alain Fraisse B. Sequential management of post-myocardial infarction ventricular septal defect. Archives of Cardiovascular Disease. 2015; 108(5): 321-330. Google Scholar.
[4]
. After surgical or percutaneous closure, mortality rate is approximately 30 to 40% at 30 days
[3]
Asmaa Ameur, Rim Raissouni, Houda Souilk, Chaimae Rhemimet et coll. Post-myocardial infarction ventricular septal defect: a case report and literature review. Int. J. Adv. Res. 2023 feb; 11, 2: 155-9.
[3]
. In Togo, as in most African countries, data on ventricular septal rupture complicating myocardial infarction are scarce
[5]
Sacca-Vehounkpe J, Houenassi M, Tchabi Y, Dossou-Yovo Akindes R, Dade A, Massougbodi M, Agboton H. Complications and mortality of myocardial infarction. Tropical cardiology. 2005; 31, 124: 51-3.
[5]
. Thus, we report the case of a post-myocardial infarction ventricular septal rupture observed in the cardiology department of the Kara Teaching Hospital.
2. Clinical Observation
This was a 65-year-old female homemaker admitted to the cardiology department of the Kara teaching Hospital for chest pain. The onset of symptoms dated back approximately six days prior to admission, marked by the sudden onset of angina-like chest pain that occurred intermittently. This initial episode was treated unsuccessfully at a peripheral health facility with gastric protectants, analgesics, and non-steroidal anti-inflammatory drugs. Due to the persistence of the chest pain, the patient was transferred to the cardiology department of the Kara teaching Hospital for more appropriate management. She had no major cardiovascular risk factors or known medical history. She was a known alcoholic.
The clinical examination on admission revealed: good hemodynamic status (blood pressure 125/67 mmHg, heart rate 80 bpm, respiratory rate 19 breaths per minute, oxygen saturation 98% on room air); good level of consciousness (Glasgow Coma Scale score 15/15); and no signs of heart failure. There was no heart murmur on auscultation.
The electrocardiogram showed a baseline sinus rhythm with a heart rate of 78 bpm, an isolated atrial premature beat, left ventricular hypertrophy, and ST elevation in the anteroseptal and inferior leads (anteroseptal and inferior STEMI) with reciprocal changes in the superior lateral leads.
Cardiac Doppler ultrasound revealed dilation of the left heart chambers (LVEDD = 58.3 mm; LAA = 22.11 cm²) with good left ventricular systolic function (LVEF = 69% on the biplan). There was akinesis of the mid and apical segments of the septal and inferoseptal walls. Left ventricular filling pressures were elevated (E/A = 2.03, E/E' = 14). The right ventricle had normal morphology with good systolic function (TAPSE = 21 mm). There was pulmonary hypertension (SPAP = 60 mmHg).
The frontal chest X-ray had revealed cardiomegaly with a cardiothoracic index of 0.74, associated with straightness of the left middle arch, lengthening of the left lower arch with the apex subdiaphragmatic and overhang with double contour appearance of the right lower arch.
Laboratory tests revealed that troponin I was elevated at 4979 ng/ml, 248 times the normal level; urea was 1.73 g/l; creatinine was 0,043 g/l with a glomerular filtration rate of 17 ml/min; random blood glucose was 2.66 g/l; a complete blood count showed leukocytosis of 15,450/mm³ with neutrophilia of 13.97 G/l and normochromic microcytic anemia of 104 g/l; serum electrolytes were within normal limits; and C-reactive protein was elevated at 0,214 g/l. Neither primary angioplasty nor thrombolysis was performed due to a lack of funding. She only received treatment consisting of: therapeutic dose anticoagulation (sodium heparin), dual antiplatelet therapy (aspirin + clopidogrel), statin (atorvastatin), antibiotic therapy (ceftriaxone), insulin therapy (actrapid), diuretic (furosemide).
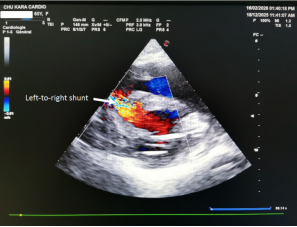
The patient's condition was marked by the onset, on the third day, of cardiogenic shock with a blood pressure of 80/56 mmHg. Cardiac auscultation revealed a loud harsh pansystolic murmur. Doppler cardiac ultrasound showed a ventricular septal defect (Figure 1) in the mid-ventricular segment with a left-to-right shunt (Figure 2). Since repair of the ventricular septal defect (surgery or angioplasty) was not possible in the department, the patient received only treatment for shock (vasopressors), with no success. On the fourth day of her admission, she experienced a cardiorespiratory arrest, which was unsuccessfully resuscitated.
Myocardial infarction is a serious and potentially fatal cardiovascular emergency due to its complications, including septal or free wall rupture of the left ventricle. It is a formidable complication because in-hospital mortality remains high, despite advances in early management
[3]
Asmaa Ameur, Rim Raissouni, Houda Souilk, Chaimae Rhemimet et coll. Post-myocardial infarction ventricular septal defect: a case report and literature review. Int. J. Adv. Res. 2023 feb; 11, 2: 155-9.
[3]
. The overall incidence remains difficult to assess, as many patients die in the pre-hospital phase without confirmation of the cause of death
[6]
Reeder GS. Identification and treatment of complications of myocardial infarction. Mayo Clin Proc. 1995 Sep; 70(9): 880-884. PubMed | Google Scholar.
[7]
Pohjola-Sintonen S, Muller JE, Stone PH et al. Ventricular septal and free wall rupture complication acute myocardial infarction: experience in the Multicenter Investigation of Limitation of Infarction Size. Am Heart J. 1989 Apr; 117(4): 809-818. PubMed | Google Scholar.
[6, 7]
.
Post-myocardial infarction ventricular septal rupture occurs in approximately 0.5% of ST elevation myocardial infarction, on average within 3 to 5 days post-myocardial infarction. It is most often the initial, extensive defect and is caused in most cases by a single-vessel lesion of the culprit coronary artery, with a small collateral network
[8]
Skehan JD, Carey C, Norrell MS, et al. Patterns of coronary artery disease in post-infarction ventricular septal rupture. Br Heart J 1989; 62: 268-72.
[8]
. Doppler echocardiography, performed as soon as a diffuse pansystolic murmur appears, allows for a definitive diagnosis, highlighting the defect in two-dimensional mode and the left-to-right shunt on color Doppler. Transesophageal echocardiography also allows for a definitive diagnosis in patients with poor echocardiographic images
[9]
Braunwald E, Zipes DP, Libby P. Acute Myocardial Infarction. In: Antman EM, Braunwald E, ed. Heart Disease, a text book of cardiovascular medicine. 6e ed. Philadelphia: WB Saunders. 2001: 1114-218. Google Scholar.
[9]
. In our patient, the septal rupture occurred on the third day of hospitalization, suspected due to a pansystolic murmur again associated with shock, and confirmed by Doppler echocardiography, which visualized the lesion.
The main factors implicated in the occurrence of septal rupture in this clinical case were: advanced age related to senescence and the loss of the myocardium's self-protective capacity; female sex, which is thought to be more susceptible to rupture due to the presence of structural collagen more often found in women
[10]
Ledakowicz-Polak A, Polak L, Zielinskra M. Ventricular septal defect complicating acute myocardial infarction-still an unsolved problem in the invasive treatment era. Cardiovasc Pathol. 2011 Mar-Apr; 20(2): 93-8. PubMed | Google Scholar.
[10]
; the absence of a history of angina or myocardial infarction
[2]
Menon V, Webb JG, Hillis LD, Sleeper LA, Abboud R, Dzavik V, et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: a report from the SHOCK Trial Registry: Should we emergently revascularize Occluded Coronaries in cardiogenic shock? J Am CollCardiol. 2000; 36(3): 1110-6. PubMed | Google Scholar.
[11]
Ilham M’hamdi, Halima Benjelloune. Circumferential ventricular septal defect following myocardial infarction: a case report and literature review. Pan African Medical Journal. 2015; 20: 310.
, explaining the lack of development of collateral circulation, and especially the complete occlusion of the responsible artery and the creation of extensive necrosis exposing to septal rupture
[2]
Menon V, Webb JG, Hillis LD, Sleeper LA, Abboud R, Dzavik V, et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: a report from the SHOCK Trial Registry: Should we emergently revascularize Occluded Coronaries in cardiogenic shock? J Am CollCardiol. 2000; 36(3): 1110-6. PubMed | Google Scholar.
[10]
Ledakowicz-Polak A, Polak L, Zielinskra M. Ventricular septal defect complicating acute myocardial infarction-still an unsolved problem in the invasive treatment era. Cardiovasc Pathol. 2011 Mar-Apr; 20(2): 93-8. PubMed | Google Scholar.
[2, 10]
; and finally the absence of early reperfusion, which remains the main risk factor
[11]
Ilham M’hamdi, Halima Benjelloune. Circumferential ventricular septal defect following myocardial infarction: a case report and literature review. Pan African Medical Journal. 2015; 20: 310.
Treatment of a septal defect is surgical and consists of closure with a prosthetic patch. Ideally, the patient is presented to the surgeon in optimal hemodynamic conditions with appropriate resuscitation management (intra-aortic balloon pump, positive inotropic agents) as soon as possible
[12]
Cummings RG, Califf R, Jones RN, Reimer KA, Kong YH, Lowe JE. Correlates of survival in patients with post infarction ventricular septal defect. Ann Thorac Surg. 1989 Jun; 47(6): 824-830. PubMed | Google Scholar.
[12]
. As in most sub-Saharan countries, the technical infrastructure is insufficient, and such treatments are impossible. Indeed, the lack of cardiac surgery in Togo constitutes an obstacle to the management of certain cardiac pathologies, such as post-myocardial infarction septal rupture. The main prognostic factors for septal rupture identified in the literature are the severity of global systolic dysfunction secondary to the infarction and the extent of the septal defect, the main clinical manifestation of which is hemodynamic instability. Once shock develops, the prognosis is even worse, with very high mortality
[12]
Cummings RG, Califf R, Jones RN, Reimer KA, Kong YH, Lowe JE. Correlates of survival in patients with post infarction ventricular septal defect. Ann Thorac Surg. 1989 Jun; 47(6): 824-830. PubMed | Google Scholar.
[12]
. This was the case for the patient in the clinical case, who died in less than 24 hours after the onset of shock.
4. Conclusion
We have illustrated one of the rare complications of myocardial infarction: post-myocardial infarction septal rupture. This complication is primarily associated with inadequate treatment of myocardial infarction, particularly thrombolysis. Hence the importance of optimizing the management of myocardial infarction in the acute phase.
Crenshaw BS, Granger CB, Birnbaum Y, Pieper KS, Morris DC, Kleiman NS, et al. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction: GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators. Circulation. 2000 Jan 4-11; 101(1): 27-32.
[2]
Menon V, Webb JG, Hillis LD, Sleeper LA, Abboud R, Dzavik V, et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: a report from the SHOCK Trial Registry: Should we emergently revascularize Occluded Coronaries in cardiogenic shock? J Am CollCardiol. 2000; 36(3): 1110-6. PubMed | Google Scholar.
[3]
Asmaa Ameur, Rim Raissouni, Houda Souilk, Chaimae Rhemimet et coll. Post-myocardial infarction ventricular septal defect: a case report and literature review. Int. J. Adv. Res. 2023 feb; 11, 2: 155-9.
[4]
Kalyani R, Trivedi A, Philippe Aldebertb, Alberto Riberi C, Julien Mancinid E, Gilles Levyf, Jean-Christophe Maciag, Jacques Quilicci C, Gilbert Habibc, Alain Fraisse B. Sequential management of post-myocardial infarction ventricular septal defect. Archives of Cardiovascular Disease. 2015; 108(5): 321-330. Google Scholar.
[5]
Sacca-Vehounkpe J, Houenassi M, Tchabi Y, Dossou-Yovo Akindes R, Dade A, Massougbodi M, Agboton H. Complications and mortality of myocardial infarction. Tropical cardiology. 2005; 31, 124: 51-3.
[6]
Reeder GS. Identification and treatment of complications of myocardial infarction. Mayo Clin Proc. 1995 Sep; 70(9): 880-884. PubMed | Google Scholar.
[7]
Pohjola-Sintonen S, Muller JE, Stone PH et al. Ventricular septal and free wall rupture complication acute myocardial infarction: experience in the Multicenter Investigation of Limitation of Infarction Size. Am Heart J. 1989 Apr; 117(4): 809-818. PubMed | Google Scholar.
[8]
Skehan JD, Carey C, Norrell MS, et al. Patterns of coronary artery disease in post-infarction ventricular septal rupture. Br Heart J 1989; 62: 268-72.
[9]
Braunwald E, Zipes DP, Libby P. Acute Myocardial Infarction. In: Antman EM, Braunwald E, ed. Heart Disease, a text book of cardiovascular medicine. 6e ed. Philadelphia: WB Saunders. 2001: 1114-218. Google Scholar.
[10]
Ledakowicz-Polak A, Polak L, Zielinskra M. Ventricular septal defect complicating acute myocardial infarction-still an unsolved problem in the invasive treatment era. Cardiovasc Pathol. 2011 Mar-Apr; 20(2): 93-8. PubMed | Google Scholar.
[11]
Ilham M’hamdi, Halima Benjelloune. Circumferential ventricular septal defect following myocardial infarction: a case report and literature review. Pan African Medical Journal. 2015; 20: 310.
Cummings RG, Califf R, Jones RN, Reimer KA, Kong YH, Lowe JE. Correlates of survival in patients with post infarction ventricular septal defect. Ann Thorac Surg. 1989 Jun; 47(6): 824-830. PubMed | Google Scholar.
Tcherou, T., Sem, F. O. T., Abena, C. P. Z., Allarangue, D., Lakpa, O., et al. (2026). Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital. Cardiology and Cardiovascular Research, 10(1), 7-10. https://doi.org/10.11648/j.ccr.20261001.12
Tcherou, T.; Sem, F. O. T.; Abena, C. P. Z.; Allarangue, D.; Lakpa, O., et al. Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital. Cardiol. Cardiovasc. Res.2026, 10(1), 7-10. doi: 10.11648/j.ccr.20261001.12
Tcherou T, Sem FOT, Abena CPZ, Allarangue D, Lakpa O, et al. Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital. Cardiol Cardiovasc Res. 2026;10(1):7-10. doi: 10.11648/j.ccr.20261001.12
@article{10.11648/j.ccr.20261001.12,
author = {Tchaa Tcherou and Fiacre Odilon Tolmbaye Sem and Clementine Pascale Zoalang Abena and Djindimadje Allarangue and Olga Lakpa and John Michael Ngalle Mbondjo and Ayao Sergio Spero De Souza and Gottara Winigah Soga and Doguensaga Borgatia Atta and Abalo Mario Bakai and Komlavi Yayehd and Machihude Pio},
title = {Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital},
journal = {Cardiology and Cardiovascular Research},
volume = {10},
number = {1},
pages = {7-10},
doi = {10.11648/j.ccr.20261001.12},
url = {https://doi.org/10.11648/j.ccr.20261001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20261001.12},
abstract = {Post- myocardial infarction ventricular septal rupture is a rare but very fatal complication if early and appropriate management is not provided or is delayed. Despite medical advances in treatment, the mortality rate associated with ventricular septal rupture following myocardial infarction remains very high. We report the case of a 65-year-old woman with a history of alcohol abuse, hospitalized in the cardiology department of Kara Teaching Hospital for an anteroseptal ST elevation myocardial infarction that was not treated with thrombolysis. The patient's condition was marked by the occurrence of a ventricular septal rupture on the third day, followed by death on the fourth day, without surgical repair of the septum. This case illustrates the severity of the mechanical complications of myocardial infarction. The lack of cardiac surgery in Togo constitutes a fatal obstacle to the management of certain cardiac pathologies, such as post-myocardial infarction ventricular septal rupture. Hence the need to improve the local technical platform to ensure better patient care.},
year = {2026}
}
TY - JOUR
T1 - Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital
AU - Tchaa Tcherou
AU - Fiacre Odilon Tolmbaye Sem
AU - Clementine Pascale Zoalang Abena
AU - Djindimadje Allarangue
AU - Olga Lakpa
AU - John Michael Ngalle Mbondjo
AU - Ayao Sergio Spero De Souza
AU - Gottara Winigah Soga
AU - Doguensaga Borgatia Atta
AU - Abalo Mario Bakai
AU - Komlavi Yayehd
AU - Machihude Pio
Y1 - 2026/03/27
PY - 2026
N1 - https://doi.org/10.11648/j.ccr.20261001.12
DO - 10.11648/j.ccr.20261001.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 7
EP - 10
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20261001.12
AB - Post- myocardial infarction ventricular septal rupture is a rare but very fatal complication if early and appropriate management is not provided or is delayed. Despite medical advances in treatment, the mortality rate associated with ventricular septal rupture following myocardial infarction remains very high. We report the case of a 65-year-old woman with a history of alcohol abuse, hospitalized in the cardiology department of Kara Teaching Hospital for an anteroseptal ST elevation myocardial infarction that was not treated with thrombolysis. The patient's condition was marked by the occurrence of a ventricular septal rupture on the third day, followed by death on the fourth day, without surgical repair of the septum. This case illustrates the severity of the mechanical complications of myocardial infarction. The lack of cardiac surgery in Togo constitutes a fatal obstacle to the management of certain cardiac pathologies, such as post-myocardial infarction ventricular septal rupture. Hence the need to improve the local technical platform to ensure better patient care.
VL - 10
IS - 1
ER -
Tcherou, T., Sem, F. O. T., Abena, C. P. Z., Allarangue, D., Lakpa, O., et al. (2026). Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital. Cardiology and Cardiovascular Research, 10(1), 7-10. https://doi.org/10.11648/j.ccr.20261001.12
Tcherou, T.; Sem, F. O. T.; Abena, C. P. Z.; Allarangue, D.; Lakpa, O., et al. Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital. Cardiol. Cardiovasc. Res.2026, 10(1), 7-10. doi: 10.11648/j.ccr.20261001.12
Tcherou T, Sem FOT, Abena CPZ, Allarangue D, Lakpa O, et al. Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital. Cardiol Cardiovasc Res. 2026;10(1):7-10. doi: 10.11648/j.ccr.20261001.12
@article{10.11648/j.ccr.20261001.12,
author = {Tchaa Tcherou and Fiacre Odilon Tolmbaye Sem and Clementine Pascale Zoalang Abena and Djindimadje Allarangue and Olga Lakpa and John Michael Ngalle Mbondjo and Ayao Sergio Spero De Souza and Gottara Winigah Soga and Doguensaga Borgatia Atta and Abalo Mario Bakai and Komlavi Yayehd and Machihude Pio},
title = {Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital},
journal = {Cardiology and Cardiovascular Research},
volume = {10},
number = {1},
pages = {7-10},
doi = {10.11648/j.ccr.20261001.12},
url = {https://doi.org/10.11648/j.ccr.20261001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20261001.12},
abstract = {Post- myocardial infarction ventricular septal rupture is a rare but very fatal complication if early and appropriate management is not provided or is delayed. Despite medical advances in treatment, the mortality rate associated with ventricular septal rupture following myocardial infarction remains very high. We report the case of a 65-year-old woman with a history of alcohol abuse, hospitalized in the cardiology department of Kara Teaching Hospital for an anteroseptal ST elevation myocardial infarction that was not treated with thrombolysis. The patient's condition was marked by the occurrence of a ventricular septal rupture on the third day, followed by death on the fourth day, without surgical repair of the septum. This case illustrates the severity of the mechanical complications of myocardial infarction. The lack of cardiac surgery in Togo constitutes a fatal obstacle to the management of certain cardiac pathologies, such as post-myocardial infarction ventricular septal rupture. Hence the need to improve the local technical platform to ensure better patient care.},
year = {2026}
}
TY - JOUR
T1 - Septal Rupture Complicating a Myocardial Infarction:
A Case Report from the Cardiology Department of the Kara Teaching Hospital
AU - Tchaa Tcherou
AU - Fiacre Odilon Tolmbaye Sem
AU - Clementine Pascale Zoalang Abena
AU - Djindimadje Allarangue
AU - Olga Lakpa
AU - John Michael Ngalle Mbondjo
AU - Ayao Sergio Spero De Souza
AU - Gottara Winigah Soga
AU - Doguensaga Borgatia Atta
AU - Abalo Mario Bakai
AU - Komlavi Yayehd
AU - Machihude Pio
Y1 - 2026/03/27
PY - 2026
N1 - https://doi.org/10.11648/j.ccr.20261001.12
DO - 10.11648/j.ccr.20261001.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 7
EP - 10
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20261001.12
AB - Post- myocardial infarction ventricular septal rupture is a rare but very fatal complication if early and appropriate management is not provided or is delayed. Despite medical advances in treatment, the mortality rate associated with ventricular septal rupture following myocardial infarction remains very high. We report the case of a 65-year-old woman with a history of alcohol abuse, hospitalized in the cardiology department of Kara Teaching Hospital for an anteroseptal ST elevation myocardial infarction that was not treated with thrombolysis. The patient's condition was marked by the occurrence of a ventricular septal rupture on the third day, followed by death on the fourth day, without surgical repair of the septum. This case illustrates the severity of the mechanical complications of myocardial infarction. The lack of cardiac surgery in Togo constitutes a fatal obstacle to the management of certain cardiac pathologies, such as post-myocardial infarction ventricular septal rupture. Hence the need to improve the local technical platform to ensure better patient care.
VL - 10
IS - 1
ER -