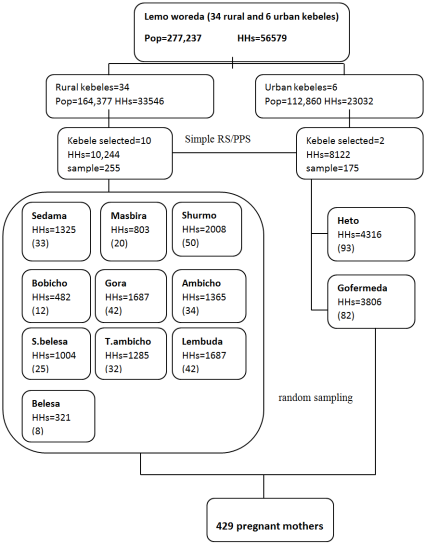
During pregnancy, a woman needs good nutrition for a healthy birth outcome. Besides, the need for nutrients dramatically increases more during pregnancy than at any other stage in the woman’s life. However, nutrient deficiencies and imbalanced dietary intake occur during the reproductive period in urban and rural women in both developing and developed nations. Nevertheless, there is a lack of information on dietary diversity among urban and rural pregnant women in Ethiopia. Therefore, this study was designed with the objectives of comparing the dietary diversity among pregnant women between urban and rural areas, and to identify associated factors in Lemo Woreda, Hadiya Zone, Central Ethiopia. A community-based comparative cross-sectional study was conducted on 429 pregnant women in urban and rural areas of Lemo Woreda, Hadiya Zone in July 2021. The collected data was entered in Epi data version 3.1, and exported to SPSS version 20 for analysis. Binary and multivariable logistic regression analyses were conducted to identify factors associated with the dietary diversity practice of pregnant mothers. P-value ≤0.05 was considered as statically significant. The proportion of pregnant women who had adequate dietary diversity practice was 35.9%. There was no statistical difference between urban and rural pregnant women in dietary diversity practice. Age (AOR=0.44, 95% CI: 0.20-0.98), family size (AOR=1.886, 95%CI: 1.094-3.250), occupation (AOR=3.30, 95%CI: 1.002-10.873) and household food security (AOR=5.0, 95%CI: 2.919-8.594) independently predicted dietary diversity practice. The prevalence of adequate dietary diversity among pregnant women was low. Therefore, interventions on household food security, women's occupations, and promoting family planning may improve the dietary diversity among pregnant women in the study areas.
| Published in | International Journal of Food Science and Biotechnology (Volume 11, Issue 1) |
| DOI | 10.11648/j.ijfsb.20261101.12 |
| Page(s) | 8-21 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Dietary Diversity, Hadiya Zone, Lemo Woreda, Pregnant Women, Central Ethiopia, Urban and Rural Areas
Variables | DDP No | DDP Yes | CI | Power | 1:1 Ratio | OR | Total Sample size | Source |
|---|---|---|---|---|---|---|---|---|
ANC visit | 20.2% | 36.6 | 95% | 80 | 1:1 | 2.8 | 260 | [12] |
Educational status | 15.8% | 48.9 | 95% | 80 | 1:1 | 5.0 | 72 | [13] |
Nutrition information | 12% | 57.7% | 95% | 80 | 1:1 | 4.8 | 40 | [14] |
Variables | Category | Residence | |
|---|---|---|---|
Urban N (%) | Rural N (%) | ||
Religion | Protestant | 119 (69.6) | 159 (61.6) |
Muslim | 18 (10.5) | 53 (20.5) | |
Catholic | 3 (1.8) | 13 (5) | |
Orthodox | 31 (18.1) | 33 (12.8) | |
Ethnicity | Hadiya | 105 (61.4) | 159 (61.6) |
Kembata | 14 (8.2) | 27 (10.5) | |
Siltea | 20 (11.7) | 51 (19.8) | |
Gurage | 14 (8.2) | 5 (1.9%) | |
Others | 18 (10.5) | 16 (6.2) | |
Educational level of the women | Illeterate | 5 (2.9) | 44 (17.1) |
Read and write | 12 (7) | 35 (13.6) | |
Primary | 45 (26.3) | 78 (30.2) | |
Secondary | 64 (37.4) | 64 (24.8) | |
Collage and above | 45 (26.3) | 37 (14.3) | |
Educational level of husband | Illeterate | 12 (7) | 31 (12) |
Read and write | 8 (4.7) | 40 (15.5) | |
Primary | 30 (17.5) | 47 (18.2) | |
Secondary | 54 (31.6) | 77 (29.8) | |
Collage and above | 67 (39.2) | 63 (24.4) | |
Occupation of woman | Housewife | 87 (50.9) | 177 (68.6) |
Daily labor | 6 (3.5) | 11 (4.3) | |
Merchant | 24 (14) | 30 (11.6) | |
Private employee | 13 (7.65) | 11 (4.3) | |
Government employee | 41 (24) | 29 (4.3) | |
Occupation of husband | Daily labor | 15 (8.8) | 90 (34.9) |
Merchant | 18 (10.5) | 16 (6.2) | |
Private employee | 72 (42.1) | 86 (33.3) | |
Government employee | 55 (32.2) | 51 (19.8) | |
Others specify | 11 (6.4) | 15 (5.8) | |
Family size | 1-3 | 48 (28.1) | 45 (17.4) |
4-6 | 65 (38) | 100 (38.8) | |
>=7 | 58 (33.9) | 113 (43.8) | |
Age category | <20 | 47 (27.5) | 80 (31) |
21-30 | 59 (34.5) | 91 (35.3) | |
31-40 | 42 (24.6) | 68 (26.4) | |
>40 | 23 (13.5) | 19 (7.4) | |
Wealth index | Low | 53 (31) | 112 (43.4) |
Medium | 69 (40.4) | 91 (35.3) | |
High | 49 (28.7) | 55 (21.3) | |
HHFI | Food secure | 49 (28.7) | 47 (18.2) |
Food insecure | 122 (71.3) | (81.8) | |
Variables | Category | Residence | |
|---|---|---|---|
Urban N (%) | Rural N (%) | ||
Gravidity | Prim gravida | 121 (70.8) | 144 (55.8) |
Multigravida | 45 (26.3) | 100 (38.8) | |
Grand gravida | 5 (2.9) | 14 (5.4) | |
Parity | Null parity | 101 (84.9) | 146 (68.5) |
Prime-parity | 17 (14.3) | 63 (29.6) | |
Multi parity | 19 (0.8) | 4 (1.9) | |
Gestational age | Frist trimester | 6 (3.5) | 12 (4.7) |
Second trimester | 99 (57.9) | 167 (64.7) | |
Third trimester | 66 (38.6) | 79 (30.6) | |
Anemic in current pregnancy | Yes | 74 (43.3) | 113 (43.8) |
Did ANC visit | Yes | 112 (65.5) | 159 (61.6) |
Place of ANC follow up | Hospital | 65 (38) | 60 (23.3) |
Health center | 44 (25.7) | 108 (41.9) | |
Health post | 3 (1.8) | 3 (1.2) | |
Private clinic | 20 (11.7) | 13 (5) | |
No follow up | 39 (22.8) | 74 (28.7) | |
Frequency of ANC visit | One times | 25 (14.6) | 55 (21.3) |
Two times | 38 (22.2) | 52 (20.2) | |
Three times | 28 (16.4) | 51 (19.8) | |
Four times and more | 23 (13.5) | 25 (9.7) | |
No follow up | 57 (33.3) | 75 (29.1) | |
Recieved iron supplement | Yes | 68 (39.8) | 95 (36.8) |
History of chronic disease | Yes | 14 (8.2) | 14 (5.4) |
History of abortion | Yes | 30 (17.5) | 39 (15.1) |
History of preterm delivery | Yes | 6 (3.5) | 13 (5) |
Obtained nutritional counseling | Yes | 24 (14) | (16.7) |
Variables | Category | Residence | |
|---|---|---|---|
Urban N (%) | Rural N (%) | ||
Sources of food | Own production | 21 (12.3) | 126 (48.8) |
Purchase | 150 (87.7) | 127 (49.2) | |
Relief | 0 (0) | 5 (1.9) | |
Home garden | Yes | 36 (21.9) | 121 (46.9) |
No | 135 (78.9) | 137 (53.4) | |
Eating pattern | ≤ 2 times/day | 71 (41.5) | 122 (47.3) |
3-5 times/day | 100 (58.5) | 136 (52.7) | |
Drunk alcohol in the last 7-days | Yes | 5 (2.9) | 8 (3.1) |
No | 166 (97.1) | 250 (96.9) | |
Drink coffee/tea immediately after meal | Yes | 119 (69.6) | 180 (69.8) |
No | 52 (30.4) | 78 (30.2) | |
Chewing chat | Yes | 5 (2.9) | 4 (1.6) |
No | 166 (97.1) | 254 (98.4) | |
Smoking | Yes | 1 (0.6) | 1 (100) |
No | 170 (99.4) | 257 (99.6) | |
Any food taboo for pregnant women | Yes | 87 (50.9) | 120 (46.5) |
No | 84 (49.1) | 138 (53.5) | |
Food groups consumed | Residence | p-value | |
|---|---|---|---|
Urban N (%) | Rural N (%) | ||
Grains, white roots and tubers, and plantains | 78 (45.6) | 120 (46.5) | 0.856 |
Pulses (beans, peas and lentils) | 55 (32.2) | 48 (18.6) | 0.001* |
Nuts and seeds | 106 (62) | 154 (59.7) | 0.634 |
Dairy | 60 (35.1) | 100 (38.8) | 0.442 |
Meat, poultry and fish | 93 (54.4) | 117 (45.3) | 0.067 |
Eggs | 72 (42.1) | 97 (37.6) | 0.351 |
Dark green leafy vegetables | 30 (17.5) | 38 (14.7) | 0.436 |
Other vitamin A-rich fruits and vegetables | 31 (18.1) | 19 (7.4) | 0.001* |
Other vegetables | 81 (47.4) | 127 (49.2) | 0.707 |
Mean WDDS | 0.3977 | 0.333 | |
Adeqaute DDS | 68 (39.8) | 86 (33.3) | 0.175 |
Independent variables | WDDS | COR (95% CI) | AOR (95% CI) | P-value | |
|---|---|---|---|---|---|
Adequate | Inadequate | ||||
N (%) | N (%) | ||||
Educational status of women | |||||
Illiterate | 17 (11.0) | 32 (11.6) | 1.21 (0.57, 2.57) | 0.83 (0.26, 2.57) | 0.97 |
Read and write | 16 (10.4) | 31 (11.3) | 1.17 (0.55, 2.53) | 0.88 (0.29, 2.62) | 0.65 |
Primary | 47 (30.5) | 76 (27.6) | 1.41 (0.78, 2.56) | 0.74 (0.29, 1.88) | 0.28 |
Secondary | 49 (31.8) | 79 (28.7) | 1.41 (0.79, 2.56) | 0.80 (0.34, 1.89)* | 0.60 |
Higher level | 25 (16.1) | 57 (20.7) | 1 | 1 | |
Occupation of the husband | |||||
Daily laborer | 35 (22.7) | 70 (25.5) | 2.10 (0.73, 6.04) | 2.07 (0.60, 7.17) | 0.25 |
Merchant | 14 (9.1) | 20 (7.3) | 2.94 (0.89, 9.67) | 2.34 (0.58, 9.39) | 0.23 |
Private | 67 (43.5) | 91 (33.1) | 3.09 (1.11\, 8.62)* | 2.45 (0.78, 7.73) | 0.12 |
Government | 33 (21.4) | 73 (26.5) | 1.89 (0.66-5.47) | 2.31 (0.69-7.69) | 0.172 |
Others | 5 (3.2) | 21 (7.6) | 1 | 1 | |
Age category | |||||
<20 years | 38 (24.7) | 89 (32.4) | 0.35 (0.17, 0.72)* | 0.44 (0.20, 0.98)* | 0.04 |
21-30 years | 61 (39.6) | 89 (32.4) | 0.57 (0.28, 1.13) | 0.79 (0.36, 1.72) | 0.52 |
31-40 years | 32 (20.8) | 78 (28.4) | 0.34 (0.16, 0.71)* | 0.57 (0.24, 1.31) | 0.17 |
>40 years | 23 (14.9) | 19 (6.9) | 1 | 1 | |
Family size | |||||
1-3 | 36 (23.4) | 57 (20.7) | 1.49 (0.87, 2.53) | 1.45 (0.76, 2.78) | 0.24 |
4-6 | 67 (43.5) | 98 (35.6) | 1.61 (1.02, 2.53)* | 1.89 (1.09, 3.25)* | 0.43 |
>7 | 51 (33.1) | 120 (43.6) | 1 | 1 | |
MUAC | |||||
Undernourished | 64 (41.6) | 101 (36.7) | 1.225 (0.82-1.83) | 1.083 (0.68-1.73) | 0.74 |
Normal | 90 (58.4) | 174 (63.3) | 1 | 1 | |
Husband's educational status | |||||
Illiterate | 14 (9.1) | 29 (10.5) | 1.17 (0.56, 2.45) | 1.24 (0.41, 3.73) | 0.07 |
Read and write | 22 (14.3) | 26 (9.5) | 2.05 (1.04, 4.05)* | 2.52 (0.93, 6.84) | 0.26 |
Primary level | 32 (20.8) | 45 (16.4) | 1.72 (0.95, 3.11) | 1.65 (0.6, 3.25) | 0.34 |
Secondary level | 48 (31.2) | 83 (30.2) | 1.40 (0.83, 2.35) | 1.21 (0.74, 3.25) | 0.38 |
Higher | 38 (24.7) | 92 (33.5) | 1 | 1 | |
Residence | |||||
Urban | 68 (44.2) | 103 (37.5) | 0.76 (0.51, 1.13) | 1.21 (0.74, 1.98) | 0.44 |
Rural | 86 (55.6) | 172 (62.5) | 1 | ||
Occupation status of women | |||||
Housewife | 98 (63.6) | 166 (60.4) | 1.71 (0.94, 3.08) | 2.05 (0.80, 5.25) | 0.13 |
Daily laborer | 6 (3.9) | 11 (4) | 1.58 (0.51, 4.88) | 1.39 (0.30, 6.36) | 0.67 |
Merchant | 21 (13.6) | 33 (12) | 1.84 (0.86, 3.95) | 1.74 (0.57, 5.32) | 0.33 |
Government | 11 (7.1) | 13 (4.7) | 2.44 (0.93, 6.42)* | 3.30 (1.00, 10.87)* | 0.05 |
Private | 18 (11.7) | 52 (18.9) | 1 | 1 | |
ANC visit | |||||
1 time | 22 (14.3) | 58 (21.1) | 0.79 (0.43, 1.45) | 1.02 (0.52, 1.99) | 0.96 |
2 times | 36 (23.4) | 54 (19.6) | 1.38 (0.79, 2.41) | 1.35 (0.71, 2.55) | 0.35 |
3 times | 37 (24.0) | 42 (15.3) | 1.82 (1.03, 3.23)* | 1.79 (0.92, 3.49) | 0.08 |
≥ 4 times | 16 (10.4) | 32 (11.6) | 1.04 (0.51, 2.09) | 1.06 (0.48, 2.35) | 0.89 |
No follow up | 43 (27.9) | 89 (32.4) | 1 | 1 | |
HHFI | |||||
Food secured | 63 (40.9) | 33 (12) | 5.08 (3.13, 8.25) | 5.01 (2.92, 8.59)** | 0.001 |
Food insecured | 91 (59.1) | 242 (88) | 1 | 1 | |
ANC | Ante Natal Care |
AOR | Adjusted Odds Ratio |
BMR | Basal Metabolic Rate |
COR | Crude Odds Ration CSA: |
CI | Confidence Interval |
CVD | Cardiovascular Disease |
DD | Dietary Diversity |
DDS | Dietary Diversity Score |
EDHS | Ethiopian Demographic and Health Survey |
EPI INFO | Epidemiological Information |
FAO | Food and Agriculture Organization |
HFIAS | Household Food Insecurity Access Scale |
HHFI | Household Food Insecurity |
IUGR | Intrauterine Growth Retardation |
KM | Kilo Meter |
MDD-W | Minimum Diet Diversity Score for Women |
MUAC | Mid Upper Arm Circumference |
NGO | Non-Governmental Organization |
SD | Standard Deviation |
SNNPR | South Nation Nationalities’ and Peoples Region |
USAID | United States Agency for International Development |
WHO | World Health Organization |
WRA | Women Reproductive Age |
| [1] | Ghosh, S. (2014). Nutrition in pregnancy: Role of macro and micronutrients. Journal of Obstetrics and Gynecology. |
| [2] | Keefe, C. L., Couch, S., & Philipson, E. (2007). Nutrition and health: Handbook of nutrition and pregnancy. |
| [3] | Philipson, E. et al. (2007). Maternal energy requirements during pregnancy. |
| [4] | Lee, S. E., et al. (2013). Dietary intakes of women during pregnancy in low- and middle-income countries. Public Health Nutrition, 16(8), 1340–1353. |
| [5] | Blencowe, H., et al. (2013). Nutrition-related pregnancy outcomes and maternal mortality. |
| [6] | Global Nutrition Report. (2020). Global Nutrition Report 2020. |
| [7] | Food and Agriculture Organization (FAO). (2016). Minimum Dietary Diversity for Women (MDD-W). |
| [8] | Haidar, J. A., & Pobocik, R. S. (2009). Iron deficiency anemia among women of reproductive age in Ethiopia. BMC Blood Disorders, 9, 7. |
| [9] | Zerfu, T. A., Umeta, M., & Baye, K. (2016). Dietary habits, food taboos, and perceptions during pregnancy in rural Ethiopia. Journal of Health, Population and Nutrition, 35(1), 22. |
| [10] | Series, et al. (2020). Maternal mortality and nutrition in developing countries. |
| [11] | Federal Democratic Republic of Ethiopia. (2016). National Nutrition Program (2016–2020). |
| [12] | Yalewdeg, M., Birhane, M., & Adissu, Y. (2020). Dietary practices among pregnant women in Gedeo Zone, Ethiopia. Nutrition and Dietary Supplements, 12, 267–275. |
| [13] | Kobiro, D. H. (2018). Determinants of dietary diversity among pregnant women in Hossana town, Ethiopia. |
| [14] | G/selassie, et al. (2020). Nutrition information and dietary diversity among pregnant women. |
| [15] | Demilew, Y. M., Alene, G. D., & Belachew, T. (2020). Effect of guided counseling on dietary practices of pregnant women. PLoS ONE, 15(5), e0233429. |
| [16] | Desta, M., et al. (2019). Dietary diversity among pregnant women in Shashemane, Ethiopia. |
| [17] | Diddana, T. Z. (2019). Dietary practice and nutritional status of pregnant women in Dessie town. BMC Pregnancy and Childbirth, 19(1). |
| [18] | Nguyen, P. H., et al. (2018). Dietary diversity and micronutrient adequacy in pregnant women. Journal of Nutrition. |
| [19] | Oluleke, M., et al. (2018). Dietary practices of pregnant women in Nigeria. Journal of Advances in Medicine and Medical Research, 25(9). |
| [20] | Mideksa, S., & Dida, N. (2018). Dietary practices among pregnant women in Ambo district, Ethiopia. |
| [21] | Daba, G., et al. (2013). Nutritional practices of pregnant mothers in Guto Gida Woreda, Ethiopia. STAR Journal, 2(3), 105. |
| [22] | Shemsu, S. E. (2020). Dietary practice and nutritional status among pregnant women in Mettu, Ethiopia. Open Public Health Journal, 13(1), 538–546. |
| [23] | Tsegaye, D., et al. (2020). Undernutrition among pregnant women in Illu Aba Bor Zone, Ethiopia. |
| [24] | Abute, L., et al. (2020). Dietary practice among pregnant women in Misha Woreda, Ethiopia. |
| [25] | Jemal, K., & Awol, M. (2019). Minimum dietary diversity among pregnant women in Alamata Hospital, Ethiopia. Journal of Nutrition and Metabolism, 2019. |
| [26] | Yeromnesh. (2020). Dietary diversity among pregnant women attending ANC at Injibara General Hospital, Ethiopia. |
| [27] | Kiboi, W., Kimiywe, J., & Chege, P. (2017). Determinants of dietary diversity among pregnant women in Kenya. BMC Nutrition, 3(1). |
| [28] | Nunnery, D. L., Labban, J. D., & Dharod, J. M. (2018). Food security and dietary intake among low-income pregnant women. Public Health Nutrition, 21(4), 807–815. |
| [29] |
Na, M., et al. (2016). Maternal dietary diversity and food insecurity in rural Bangladesh. Journal of Nutrition, 146(10), 2109–2116. HYPERLINK "
https://doi.org/10.3945/jn.116.234229" https://doi.org/10.3945/jn.116.234229 |
APA Style
Tesfaye, T., Abdo, S. S., Abdo, R. A. (2026). Dietary Diversity and Associated Factors Among Pregnant Women in Lemo Woreda, Hadiya Zone, Central Ethiopia: Comparative Cross-Sectional Study. International Journal of Food Science and Biotechnology, 11(1), 8-21. https://doi.org/10.11648/j.ijfsb.20261101.12
ACS Style
Tesfaye, T.; Abdo, S. S.; Abdo, R. A. Dietary Diversity and Associated Factors Among Pregnant Women in Lemo Woreda, Hadiya Zone, Central Ethiopia: Comparative Cross-Sectional Study. Int. J. Food Sci. Biotechnol. 2026, 11(1), 8-21. doi: 10.11648/j.ijfsb.20261101.12
@article{10.11648/j.ijfsb.20261101.12,
author = {Tsegaab Tesfaye and Shambel Selman Abdo and Ritbano Ahmed Abdo},
title = {Dietary Diversity and Associated Factors Among Pregnant Women in Lemo Woreda, Hadiya Zone, Central Ethiopia: Comparative Cross-Sectional Study},
journal = {International Journal of Food Science and Biotechnology},
volume = {11},
number = {1},
pages = {8-21},
doi = {10.11648/j.ijfsb.20261101.12},
url = {https://doi.org/10.11648/j.ijfsb.20261101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijfsb.20261101.12},
abstract = {During pregnancy, a woman needs good nutrition for a healthy birth outcome. Besides, the need for nutrients dramatically increases more during pregnancy than at any other stage in the woman’s life. However, nutrient deficiencies and imbalanced dietary intake occur during the reproductive period in urban and rural women in both developing and developed nations. Nevertheless, there is a lack of information on dietary diversity among urban and rural pregnant women in Ethiopia. Therefore, this study was designed with the objectives of comparing the dietary diversity among pregnant women between urban and rural areas, and to identify associated factors in Lemo Woreda, Hadiya Zone, Central Ethiopia. A community-based comparative cross-sectional study was conducted on 429 pregnant women in urban and rural areas of Lemo Woreda, Hadiya Zone in July 2021. The collected data was entered in Epi data version 3.1, and exported to SPSS version 20 for analysis. Binary and multivariable logistic regression analyses were conducted to identify factors associated with the dietary diversity practice of pregnant mothers. P-value ≤0.05 was considered as statically significant. The proportion of pregnant women who had adequate dietary diversity practice was 35.9%. There was no statistical difference between urban and rural pregnant women in dietary diversity practice. Age (AOR=0.44, 95% CI: 0.20-0.98), family size (AOR=1.886, 95%CI: 1.094-3.250), occupation (AOR=3.30, 95%CI: 1.002-10.873) and household food security (AOR=5.0, 95%CI: 2.919-8.594) independently predicted dietary diversity practice. The prevalence of adequate dietary diversity among pregnant women was low. Therefore, interventions on household food security, women's occupations, and promoting family planning may improve the dietary diversity among pregnant women in the study areas.},
year = {2026}
}
TY - JOUR T1 - Dietary Diversity and Associated Factors Among Pregnant Women in Lemo Woreda, Hadiya Zone, Central Ethiopia: Comparative Cross-Sectional Study AU - Tsegaab Tesfaye AU - Shambel Selman Abdo AU - Ritbano Ahmed Abdo Y1 - 2026/01/20 PY - 2026 N1 - https://doi.org/10.11648/j.ijfsb.20261101.12 DO - 10.11648/j.ijfsb.20261101.12 T2 - International Journal of Food Science and Biotechnology JF - International Journal of Food Science and Biotechnology JO - International Journal of Food Science and Biotechnology SP - 8 EP - 21 PB - Science Publishing Group SN - 2578-9643 UR - https://doi.org/10.11648/j.ijfsb.20261101.12 AB - During pregnancy, a woman needs good nutrition for a healthy birth outcome. Besides, the need for nutrients dramatically increases more during pregnancy than at any other stage in the woman’s life. However, nutrient deficiencies and imbalanced dietary intake occur during the reproductive period in urban and rural women in both developing and developed nations. Nevertheless, there is a lack of information on dietary diversity among urban and rural pregnant women in Ethiopia. Therefore, this study was designed with the objectives of comparing the dietary diversity among pregnant women between urban and rural areas, and to identify associated factors in Lemo Woreda, Hadiya Zone, Central Ethiopia. A community-based comparative cross-sectional study was conducted on 429 pregnant women in urban and rural areas of Lemo Woreda, Hadiya Zone in July 2021. The collected data was entered in Epi data version 3.1, and exported to SPSS version 20 for analysis. Binary and multivariable logistic regression analyses were conducted to identify factors associated with the dietary diversity practice of pregnant mothers. P-value ≤0.05 was considered as statically significant. The proportion of pregnant women who had adequate dietary diversity practice was 35.9%. There was no statistical difference between urban and rural pregnant women in dietary diversity practice. Age (AOR=0.44, 95% CI: 0.20-0.98), family size (AOR=1.886, 95%CI: 1.094-3.250), occupation (AOR=3.30, 95%CI: 1.002-10.873) and household food security (AOR=5.0, 95%CI: 2.919-8.594) independently predicted dietary diversity practice. The prevalence of adequate dietary diversity among pregnant women was low. Therefore, interventions on household food security, women's occupations, and promoting family planning may improve the dietary diversity among pregnant women in the study areas. VL - 11 IS - 1 ER -
Department of Statistics, Wachemo University, Hossana, Ethiopia
Department of Midwifery, Wachemo Univeristy, Hossana, Ethiopia
Information