The global burden of non-communicable diseases remains unacceptably high and Kenya is among the countries experiencing an epidemiological transition from the communicable to non-communicable diseases. In Kenya, cancer is the second leading cause of non-communicable disease related mortalities after the cardiovascular diseases and Nyeri County is among the counties that are leading in this burden of non-communicable diseases. This study sought to assess the dietary practices of the cancer patients on chemotherapy at Nyeri County and Referral Hospital in comparison with the recommended dietary practices. Analytical cross-sectional study design was employed and the data on the dietary practices was collected using a 24-hour recall and a Food Frequency Questionnaire (FFQ). Sixty one percent of the respondents were female while 39% were male. Sixty one percent had acquired primary school education and half of the respondents survive on a monthly income of between 0-10,000. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. The mean energy intake of the respondents was 1068+- 520 Kcals which was not meeting the requirements as per the ESPEN clinical guidelines on cancer. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) and less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings recommended by the World Health Organization (WHO). Nutrition education and counselling is key in improving the dietary practices among the cancer patients. However, 44.19% had not received nutrition education and counselling regarding the appropriate diet to consume in the course of their treatment. This study found out that the dietary practices of the cancer patients do not meet the recommended clinical guidelines on cancer nutrition and almost half of the population had not received nutrition education and counselling services. Social and behavior change is one of the possible strategies that could be adopted to deliver nutrition information to the population, to improve the knowledge, attitude and dietary practices of cancer patients in Kenya, which in turn will improve their nutrition outcomes.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Dietary Practices, Nutrition Status, Food Frequency Questionnaire, 24-hour Recall, Body Mass Index, Malnutrition Risk
1. Introduction
Cancer is the second leading cause of non-communicable related mortalities after the cardiovascular diseases in Kenya
[1]
MoH-Kenya. Kenya STEPwise Survey for Non Communicable Diseases Risk Factors 2015 Report. Public Health 2015; 5: 8–210.
[1]
and approximately 10-20% of these mortalities are due to cancer- related malnutrition and not as a result of the tumor
[2]
Muscaritoli M, Lucia S, Farcomeni A, Lorusso V, Saracino V, Barone C, et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017; 8: 79884–96.
. The cancer burden in Kenya has been increasing with a reported incidence of 42,116 and a mortality of 27,092 cases in 2020
[3]
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71: 209–49.
. Besides the normal cancer pathogenesis, a huge percent (90%) of cancers cases develop as a result of lifestyle factors such as consumption of tobacco and alcohol, high levels of physical inactivity and sub-optimal diet, with the latter contributing to 5-10% of the total cases
[4]
Morze J, Danielewicz A, Przybyłowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr 2021; 60: 1561–86.
. This therefore indicates that consuming a healthy diet and in adequate amounts helps in prevention of both the tumor itself and also malnutrition among the cancer patients
[5]
Ministry of Health Kenya. National Guidelines for Healthy Diets. Natl Guidel Healthy Diets Phys Act 2017.
[6]
American Cancer Society. Nutrition for People With Cancer Benefits of good nutrition during cancer treatment 2018: 1–27.
[7]
Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr 2021; 40: 2898–913.
A healthy diet has a role both in cancer prevention and management. Natural polyphenols have been well studied to examine their possible health effects especially defense against oxidative stress because they contain anticancer properties
[8]
Bhosale PB, Ha SE, Vetrivel P, Kim HH, Kim SM, Kim GS. Functions of polyphenols and its anticancer properties in biomedical research: A narrative review. Transl Cancer Res 2020; 9: 7619–31.
. Dietary fish and marine omega-3 PUFAs have also been associated with survival of cancer patients because of their anti-inflammatory activity
[9]
Wang Y, Liu K, Long T, Long J, Li Y, Li J, et al. Dietary fish and omega-3 polyunsaturated fatty acids intake and cancer survival: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2023; 63: 6235–51.
A Mediterranean diet (MedDiet- a recommended cancer diet) is rich in complex carbohydrates, adequate amounts of fruits, vegetables and nuts. It also entails limited processed foods, red meats, poultry and dairy and it has been used in cancer management widely, although its uptake is still low in most countries
[4]
Morze J, Danielewicz A, Przybyłowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr 2021; 60: 1561–86.
. Other nutrients that have been associated to cancer management because of their various functions in the body is Vitamin D and selenium
[10]
Radomska D, Czarnomysy R, Radomski D, Bielawska A, Bielawski K. Selenium as a bioactive micronutrient in the human diet and its cancer chemopreventive activity. Nutrients 2021; 13: 1–25.
The ESPEN guidelines states the Total Energy Expenditure (TEE) of a cancer patient is similar to that of a healthy individual which ranges from 25-30kcal/kg/day. The amount of protein considered adequate for the cancer patients is 1g/kg/day, and if possible, a cancer patient should consume 1.5g/kg/day of proteins. Vitamins and minerals are key in management of cancer patients. There requirements are as per the RDA and there is need to supply them in adequate amounts to avoid instances of micronutrients deficiencies
[7]
Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr 2021; 40: 2898–913.
. The Kenya cancer policy 2019-2030 outlines that 27% of Kenyans are overweight and obese while 94% of people do not consume fruits and vegetables
[11]
Ministry of Health. Kenya Cancer Policy 2019-2030, 2019.
[11]
.
A 2023 meta-analysis showed that dietary fish and marine omega-3 PUFAs were associated cancer patient’s survival as a result of their anti-inflammatory activity. A consumption of about 300mg of the omega 3 PUFAs has a potential to reduce the mortalities of cancer patients by 13%
[9]
Wang Y, Liu K, Long T, Long J, Li Y, Li J, et al. Dietary fish and omega-3 polyunsaturated fatty acids intake and cancer survival: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2023; 63: 6235–51.
. This is similar to World Health recommendations of a healthy diet. The WHO outlines that a healthy diet should contain a minimum of 400g (5 servings) of fruits and vegetables in a day, adequate legumes such as beans, adequate nuts and complex carbohydrates, with less than 10% of total intake coming from free sugars
[5]
Ministry of Health Kenya. National Guidelines for Healthy Diets. Natl Guidel Healthy Diets Phys Act 2017.
[5]
. A high protein intake especially plant-based origin lowers the risks of mortalities from cancer and other non-communicable diseases. Increasing the plant protein and also replacing the animal protein with plant protein would result in a healthier population
[12]
Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. The BMJ 2020; 370.
The National cancer taskforce report released in 2022 on the cancer status in Kenya revealed that there is limited cancer research both in capacity and availability to inform policy
[13]
July 2022 NATIONAL CANCER TASKFORCE REPORT 2022.
[13]
. On this basis, this study aimed at assessing the dietary practices of cancer patients on chemotherapy attending Nyeri County Referral Hospital.
2. Materials and Methods
2.1. Research Design
This study employed analytical cross-sectional study design to collect data on the sociodemographic and economic characteristics of the cancer patients and collect data on their dietary practices. A similar study in Korea on iodine status of among the thyroid cancer patients utilized a 24-hour recall and an FFQ to collect the dietary data, employing a cross sectional study design
[14]
Choi JY, Lee JH, Song YJ. Evaluation of Iodine Status among Korean Patients with Papillary Thyroid Cancer Using Dietary and Urinary Iodine. Endocrinol Metab 2021; 36: 607–18.
This study was done in Nyeri County Referral Hospital in Nyeri County, Kenya. The county is experiencing a rise in the non- communicable diseases
[15]
Wambalaba FW, Son B, Wambalaba AE, Nyong’o D, Nyong’o A. Prevalence and Capacity of Cancer Diagnostics and Treatment: A Demand and Supply Survey of Health-Care Facilities in Kenya. Cancer Control 2019; 26: 1–12.
was used to estimate a sample size of 185 respondents at 95% Confidence Interval, 0.05 margins of error with an assumed malnutrition prevalence in Nyeri at 0.5 and an estimated non-response rate of 10%. The list of participants attending the clinic was used to select the sample using systematic random sampling. The first respondent was randomly selected using the table of random numbers generated from www.stattrek.com to determine the starting point. Every second respondent was systematically drawn until 185 respondents were achieved. The research team interviewed the respondents during the two days of clinic visits for a period of three weeks.
2.4. Validity and Reliability
Pre-testing of the research instruments enhanced the validity and reliability of the research instruments and the methodology. 10% of the total sample (18 respondents) was used in pre-testing the data collection tools at Meru County and Referral Hospital. Pre-testing aimed at evaluating the efficacy of the research instruments, sampling strategies and the method that the researcher had chosen for data analysis. It also aimed at enhancing the validity and reliability. Internal consistency (split half) method was used to indicate the degree of homogeneity of the items in the research instrument. The items on the instrument were divided into two. Reliability analysis was conducted on both sets of data and a reliability coefficient of 0.725 was generated, which is considered adequate for group studies
[18]
Danner D. Reliability – The Precision of a Measurement. GESIS Surv Guidel 2016.
There are a number of dietary assessment methods that can be used to collect dietary data. A prospective study in UK that aimed at assessing the dietary intake and colorectal cancer utilized a 24-hr recall and a food frequency questionnaire which are applicable in a cross-sectional study
[19]
Bradbury KE, Murphy N, Key TJ. Diet and colorectal cancer in UK Biobank: A prospective study. Int J Epidemiol 2020; 49: 246–58.
. The estimates acquired from the FFQ were used to identify dietary patterns, while the 24-hour recall was used to estimate the macro-and the micro- nutrient intakes of the cancer patients at NCRH. The food frequency questionnaire was designed guided by the National Guidelines for healthy diets and physical activity (2017)
[5]
Ministry of Health Kenya. National Guidelines for Healthy Diets. Natl Guidel Healthy Diets Phys Act 2017.
[5]
and the Nutrition assessment and counselling (NACs) user guide, (2016). Nine food groups were included, with the consumption estimated as daily or weekly, and an average number of servings indicated. The 24-hour recall was adopted from the Nutrition assessment and counselling (NACs) user guide, (2016).
2.6. Data Analysis
SPSS software version 27 was used to analyze the data. Nutri-survey 2007 was used to analyze the 24-hr recall data that collected individual nutrient intake. Parametric statistical tests were performed on the data, putting into consideration the assumptions of parametric tests. Measures of association (correlations) was performed to establish the strength of relationship between variables. Pearson moment correlation statistical tool was used to determine the correlation. Relationship between two categorical variables was investigated using Chi square tests. The statistical significance threshold was set at α=0.05(two tailed).
3. Results
3.1. Socio-Economic and Demographic Characteristics of the Study Population
The study had a 93% response rate which is within the acceptable range
[21]
Fincham JE. Response rates and responsiveness for surveys, standards, and the Journal. Am J Pharm Educ 2008; 72: 43.
. Sixty one percent were female while 39% of them were male. The mean (SD) age of the respondents was 65.9 for male and 55.8 for female. The youngest respondent in the population was 23 years old, with the oldest being 93 years old. Half of the respondents survive on a monthly income of between 0-10,000 Kenyan shillings and only 2.6% of the respondents earning more than Ksh. 50,000.
Table 1. Socio-economic and demographic characteristics of the study population.
Respondent’s Characteristics
Frequency
Percent (%)
Respondents gender
N=172
Male
67
39.0
Female
105
61.0
Religion
Christianity
165
95.9
Muslim
7
4.1
Respondent’s education level
Primary
105
61.0
Secondary
50
29.1
College
16
9.3
University
1
.60
Marital Status of the respondents
Married
125
72.7
Single
31
18.0
Widowed/Deceased
16
9.3
Monthly Income
0-10,000
86
50.0
10,000-20,000
49
28.5
20,000-50,000
32
18.6
50,000-100,000
5
2.9
There was a statistically significant association between education level and the monthly income of the respondents at p<0.05 rejecting a null hypothesis that there is no association between education level and the monthly income of the respondents.
3.2. Clinical Diagnosis of Cancer
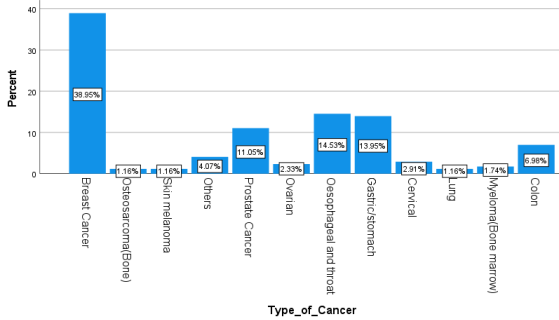
Various cancer types were reported by the respondents, with the largest percentage of respondents having breast cancer (39%), followed by esophageal and throat cancer at (14.5%) and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. Other cancer cases reported included colon cancer (7%), ovarian cancer (2.3%), cervical cancer (2.9%) and bone marrow (1.2%).
Figure 1. Distribution of the respondents by cancer types.
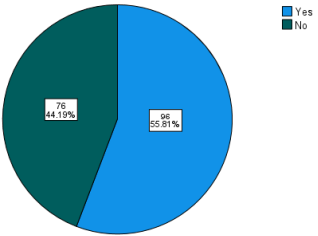
3.3. Nutritional Education and Counselling
A professional advice on nutrition is very key in cancer patients on chemotherapy. In this study, 55.81% of the respondents had received a professional advice on dietary intake during chemotherapy compared to 44.19% who had not received any nutritional counselling.
The aim of the dietary assessment (24 hr. recall and FFQ) was to characterize the dietary patterns of the respondents. The quantified 24hr-recall allowed for the calculation of individual energy and nutrients intakes. The conversion of the household measures to meaningful weights was done using a food composition database (Nutrisurvey 2007).
The mean energy intake of the 172 respondents was 1068+- 520 Kcals, 112+- 83g of carbohydrates, 46.8+-42g of protein and 27.1+-27 g of fats. Micronutrients are key in cancer care. 30-90% of cancer patients supplement their diets with micronutrients that support antioxidative process and immune-stabilizing roles. The commonly required micronutrients for cancer care are Vitamin C, Vitamin D and selenium for the antioxidative role.
Table 2. Mean dietary intakes.
Minimum
Maximum
Mean
S. D
Energy
169.30
3283.30
1068.61
520.62639
Water
240.80
3288.00
959.365
361.86533
Protein
5.50
443.40
46.8308
42.66351
Fat
.00
154.80
27.1380
27.57125
Carbohydrate
2.20
434.50
112.922
83.49550
Dietary Fiber
3.10
68.40
20.6814
12.21267
Alcohol
.00
272.10
46.1819
77.37332
PFA
.00
102.00
9.8035
14.78217
Cholesterol
.00
1102.70
92.2727
210.72963
Vitamin A
.00
23858.30
1137.71
2846.01160
Carotene
.00
7595.60
595.959
1310.93351
Vitamin E
.00
643.50
32.0442
101.53486
Vitamin B1
.10
2942.00
278.205
646.14196
Vitamin B2
.00
5892.70
107.107
618.01408
Vitamin B6
.00
3.00
.5390
.64513
Folic Acid
.00
1213.80
187.581
239.61854
Vitamin C
.10
436.30
78.6814
79.17806
Sodium
.70
5551.00
911.995
1087.75025
Potassium
165.30
8290.50
2105.25
1083.95038
Calcium
28.00
1704.50
416.126
269.89709
Magnesium
32.00
623.70
224.268
95.84983
Phosphorus
98.00
3276.00
849.868
423.89742
Iron
1.20
41.50
10.6581
6.20451
Zinc
.90
28.30
6.2738
4.58614
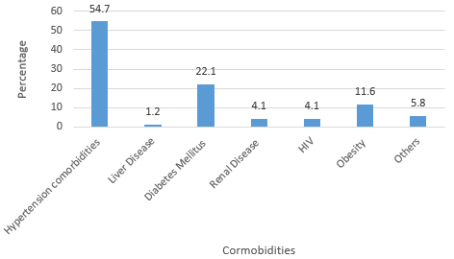
3.5. Comorbidities
Based on the Charlson comorbidity index, most cancer patients at NCRH had hypertension (54.7%), followed by Diabetes Mellitus (22.1%) and obese cases were 11.6%. The figure 3 below is a representation of the distribution of the respondents by the comorbidities present.
Figure 3. Distribution of respondents by the comorbidities.
3.6. Frequency Consumption of Various Foods by the Respondents (FFQ)
The starchy foods and the fats and oils category were the most consumed foods (65.1% respondents reporting to be taking them on a daily basis). Less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings, with 2.3 % rarely consuming fruits at all. A very small percent of people (8.7%) incorporated nuts and seeds in their diets with the largest percentage consuming the minimum serving. Similarly, a small percentage (37.8%) of respondents consumed milk and milk products key in bone strengthening.
Table 3. Frequency consumption of various foods by the respondents.
% FREQUENCY (N=172)
Food Group
Daily
Weekly
Rarely
Average Serving
Starchy foods
65.1
34.9
0
Large (65.1%)
Vegetables
57.6
42.4
0
Large (48.8%)
Fruits
41.9
55.8
2.3
Small (40.7%)
Legumes and pulses
60.5
37.8
1.7
Large (55.2%)
Nuts and seeds
8.7
44.2
47.1
Small (73.3%)
Meat, fish, animal protein
15.1
74.4
10.5
Small (61.1%)
Milk and milk products
37.8
43.0
19.2
Small (47.1%)
Fats and oils
65.1
27.9
7.0
Large (55.8%)
Sugar and sweets
33.1
33.7
33.1
Small (47.1%)
Condiments, spices and beverages
8.1
19.2
72.7
Small (83.7%)
Alcohol
2.3
2.9
94.8
Small (95.3%)
4. Discussion
4.1. Socio-Economic and Demographic Characteristics of the Respondents
Both men and women are affected by cancer non-selectively. More female (61%) had different types of cancer compared to male (39%), with the leading type of cancer among female being breast cancer (39%) and prostate cancer being the leading cancer type in men (11%). These findings agree with the 2020 global cancer statistics, where breast cancer surpassed the lung cancer incidence and was top of the commonly diagnosed cancers at 11.7% globally, and prostate was top leading male cancer at 7.3%
[3]
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71: 209–49.
. However, this study reveals higher statistics compared to the global estimates, indicating that there may be gaps in the cancer reporting or that it is because this study focused on the cancer patients on chemotherapy only. The average age of the respondents was 65.9 for male and 55.8 for female. A previous study on the diagnostic assessments in various cancer centers in Kenya, found that the most frequent age for the males is 65 and females 55
[17]
Sun Y, Phillips PCB. Understanding the Fisher equation. J Appl Econom 2004; 19: 869–86.
Income inequality has been increasing worldwide, education is one of the markers of financial stability and there is clear evidence that the higher the education level, the greater the chances of securing a formal employment and a higher income in response
[22]
Hinata A, Kabasawa K, Watanabe Y, Kitamura K, Ito Y, Takachi R, et al. Education, household income, and depressive symptoms in middle-aged and older Japanese adults. BMC Public Health 2021; 21: 1–10.
. Cancer care has been reportedly expensive and a big percent of the population requires to pay for some of the services since the National Health Insurance Fund does not comprehensively cover cancer treatment. In addition, the educated cancer patients have access to private care, improving their treatment outcomes. The significant association between education level and the monthly income of the respondents (p<0.05) was confirmed by this study. This explains why most of the respondents (61%) who had the basic primary education level had limited ability to comprehensive health care.
Most of the respondents (72.7%) were married, 18% were single while 9.3% were either divorced or widowed. A study shows that cancer survival is poorer among the unmarried compared to its counterparts who are married
[23]
Krajc K, Miroševič Š, Sajovic J, Klemenc Ketiš Z, Spiegel D, Drevenšek G, et al. Marital status and survival in cancer patients: A systematic review and meta‐analysis. Cancer Med 2023; 12: 1685–708.
. Prognosis associated with cancer diagnosis is influenced by marital status. The explanation is unclear, but researchers have tried to associate this with married individuals having the ability to follow up course of therapy compared to their unmarried counterparts. Another attempt to explain this association is that the married partners seem to present with early tumors, unlike the unmarried, yet this explanation remains unclear
[24]
Kravdal H, Syse A. Changes over time in the effect of marital status on cancer survival. BMC Public Health 2011; 11.
Nutrition education and counseling is very key in cancer care. This is because the non-communicable diseases such as cancer, hypertension, and diabetes co-exist due to the fact that they have shared risk factors
[25]
Peters R, Ee N, Peters J, Beckett N, Booth A, Rockwood K, et al. Common risk factors for major noncommunicable disease, a systematic overview of reviews and commentary: the implied potential for targeted risk reduction. Ther Adv Chronic Dis 2019; 10: 204062231988039.
. Co-morbidities that were present among the cancer patients at NCRH were hypertension, followed by Diabetes Mellitus and obesity. If a reduction in these chronic diseases has to be realized, the entire population requires nutrition education and counselling on how to prevent the non-communicable diseases through healthy lifestyle.
Despite the significant role played by nutrition education in improved nutrition outcomes, 44.19% of the respondents had not received any nutritional education in the course of their treatment. Almost thirty five percent of the respondents who had not received nutritional education reported that there are certain foods that they do not consume at all during treatment. Most of the reasons that they gave were not based on any scientific proof but was based on counsel from either relatives or village mates. One of the reported misconceptions that was reported is that, ’sugary foods acts as food for the tumor,’ that is why most of them (9.3%) would avoid carbohydrates from their diets. This justifies the need for comprehensive nutrition education among the cancer patients.
4.3. Dietary Practices of Cancer Patients
Dietary patterns of the cancer patients are very pertinent and they need to be closely monitored to prevent cancer related malnutrition
[26]
Rock CL, Thomson C, Gansler T, Gapstur SM, Mccullough ML, Patel AV, et al. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention 2020; 70: 245–71.
If cancer care has to attain the required standards, there is need to ensure nutrition and specifically dietary practices are monitored and the patients are guided accordingly. The American Cancer Society guidelines for a healthy diet recommends consumption of nutrient dense foods to maintain a healthy body weight for the cancer patients, consume adequate fruits and vegetables whole grains, limited use of red and processed meats, sugars and processed foods
[26]
Rock CL, Thomson C, Gansler T, Gapstur SM, Mccullough ML, Patel AV, et al. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention 2020; 70: 245–71.
The mean energy intake of the 172 respondents was 1068+- 520 Kcals, 112+- 83g of carbohydrates, 46.8+-42g of protein and 27.1+-27 g of fats. The ESPEN practical guideline recommends that the total energy expenditure of the cancer patients should be between 25-30kg/kg/day and the mean weight of the respondents was 60.4kgs+-13.9. From the ESPEN guidelines, the minimum energy consumption of the respondents should be 25kcals*60.4 which gives 1510kcals. The mean energy consumption of this population is lower than the minimum recommended energy intake of the cancer patients according to the ESPEN clinical guidelines. This can be linked to the nutrition impact symptoms such as nausea, vomiting and diarrhea, which cancer patients experience while undergoing treatment
[27]
de Pinho NB, Martucci RB, Rodrigues VD, D’Almeida CA, Thuler LCS, Saunders C, et al. Malnutrition associated with nutrition impact symptoms and localization of the disease: Results of a multicentric research on oncological nutrition. Clin Nutr 2019; 38: 1274–9.
in addition, micronutrients are key in cancer care. 30-90% of cancer patients supplement their diets with micronutrients that support antioxidative process and immune-stabilizing roles. The commonly required micronutrients for cancer care are Vitamin C, Vitamin D and selenium for the antioxidative role
[10]
Radomska D, Czarnomysy R, Radomski D, Bielawska A, Bielawski K. Selenium as a bioactive micronutrient in the human diet and its cancer chemopreventive activity. Nutrients 2021; 13: 1–25.
Using the Food frequency questionnaire, starchy foods and the fatty foods categories were the most consumed with majority of the respondents reporting to be taking them on a daily basis. This may be because the highest percentage of the respondents (40.1%) are farmers and mostly the starchy foods are readily available. However, this poses nutritional risks to them. The non-communicable diseases risk factors are similar, the main one being obesity and diets rich in fats and starches. Obesity pathophysiology is also linked to fat deposition associated with excessive intake of fats and carbohydrates
[28]
Lega IC, Lipscombe LL. Review: Diabetes, Obesity, and Cancer-Pathophysiology and Clinical Implications. Endocr Rev 2020; 41: 33–52.
. Whole grains for cancer care increase the bulkiness of stool. Bulky stools have an increased transit time which reduces the interaction between carcinogenic substances with normal cells
[21]
Fincham JE. Response rates and responsiveness for surveys, standards, and the Journal. Am J Pharm Educ 2008; 72: 43.
. It also limits the bacterial endotoxins which damages the cells from being absorbed. The whole grains are rich in fiber. During the digestion process, fiber breaks down into short chain fatty acids which are a source of energy that the cancer cells have the inability to utilize. This lowers the growth and development of the cancer cells
[29]
Nagy S, Petrosky SN, Beckler MD, Kesselman MM. The Impact of Modern Dietary Practices on Cancer Risk and Progression: A Systematic Review. Cureus 2023.
Less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings, with 2.3 % rarely consuming fruits at all. The WHO recommends of 3-5 servings of fruits and vegetables per week which was not being met by 41.9% of the respondents. Fruits and vegetables are associated with antioxidants that are so important in management of cancer. The anti-oxidant properties of flavonoids, Vitamin C and E and carotenoids are mostly found in fruits and the dark green vegetables. A very small percent of people (8.7%) incorporated nuts and seeds in their diets with the largest percentage consuming the minimum serving. Nuts and seeds are important sources of poly-unsaturated fatty acids, and specifically omega 3 and omega 6 fatty acids. Omega 3 fatty acids have been associated with reduction in inflammation, reduced angiogenesis, and metastasis and reduced proliferation of cells
[30]
Hanson S, Thorpe G, Winstanley L, Abdelhamid AS, Hooper L, Abdelhamid A, et al. Omega-3, omega-6 and total dietary polyunsaturated fat on cancer incidence: systematic review and meta-analysis of randomised trials. Br J Cancer 2020; 122: 1260–70.
A small percentage (37.8%) of respondents consumed milk and milk products, which are very high sources of calcium, key in bone strengthening. One of the common problems associated with chemotherapy treatment in cancer care is bone loss. Chemotherapy drugs such as doxorubicin and cisplatin reduce calcium levels in the body, leading to body loss, (MD Anderson, 2020). This must be supplied in adequate amounts together with Vitamin D rich foods because optimal levels of Vitamin D are necessary to enhance calcium absorption. This study reveals that a small percentage of the respondents consumed foods from the fish and meats categories, which is the main dietary source of Vitamin D.
5. Conclusions
Dietary assessment of cancer patients is key for revealing the dietary practices which have impact on their nutrition status. The findings from this study reveal inappropriate dietary practices among the cancer patients at Nyeri County and Referral Hospital. A 24-hour recall and a Food Frequency Questionnaire are key dietary assessment tools which can be easily adopted for use in a hospital setting to determine the dietary adequacy and patterns of these patients which informs the specific nutrition interventions for the patients. In addition, Nutrition education on the appropriate diet during treatment is a potential strategy for improved dietary practices of the cancer patients. Social and behavior change approaches can be adopted to deliver the key nutrition messages for improved dietary practices of cancer patients in Kenya.
Abbreviations
ESPEN
European Society for Clinical Nutrition and Metabolism
BMI
Body Mass Index
NCRH
Nyeri County Referral Hospital
FFQ
Food Frequency Questionnaire
Acknowledgments
I would like to appreciate the support from the Department of Health at Nyeri County during this research. In addition, special appreciation goes to the staff at the oncology department in Nyeri County Referral Hospital for the support in data collection.
Peter Chege: Conceptualization, Supervision, Writing – review & editing
Regina Kamuhu: Supervision, Writing – review & editing
Funding
This work is not supported by any external funding
Data Availability Statement
The data supporting the outcome of this research work has been reported in this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
MoH-Kenya. Kenya STEPwise Survey for Non Communicable Diseases Risk Factors 2015 Report. Public Health 2015; 5: 8–210.
[2]
Muscaritoli M, Lucia S, Farcomeni A, Lorusso V, Saracino V, Barone C, et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017; 8: 79884–96.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71: 209–49.
Morze J, Danielewicz A, Przybyłowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr 2021; 60: 1561–86.
Bhosale PB, Ha SE, Vetrivel P, Kim HH, Kim SM, Kim GS. Functions of polyphenols and its anticancer properties in biomedical research: A narrative review. Transl Cancer Res 2020; 9: 7619–31.
Wang Y, Liu K, Long T, Long J, Li Y, Li J, et al. Dietary fish and omega-3 polyunsaturated fatty acids intake and cancer survival: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2023; 63: 6235–51.
Radomska D, Czarnomysy R, Radomski D, Bielawska A, Bielawski K. Selenium as a bioactive micronutrient in the human diet and its cancer chemopreventive activity. Nutrients 2021; 13: 1–25.
Ministry of Health. Kenya Cancer Policy 2019-2030, 2019.
[12]
Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. The BMJ 2020; 370.
Choi JY, Lee JH, Song YJ. Evaluation of Iodine Status among Korean Patients with Papillary Thyroid Cancer Using Dietary and Urinary Iodine. Endocrinol Metab 2021; 36: 607–18.
Wambalaba FW, Son B, Wambalaba AE, Nyong’o D, Nyong’o A. Prevalence and Capacity of Cancer Diagnostics and Treatment: A Demand and Supply Survey of Health-Care Facilities in Kenya. Cancer Control 2019; 26: 1–12.
Hinata A, Kabasawa K, Watanabe Y, Kitamura K, Ito Y, Takachi R, et al. Education, household income, and depressive symptoms in middle-aged and older Japanese adults. BMC Public Health 2021; 21: 1–10.
Krajc K, Miroševič Š, Sajovic J, Klemenc Ketiš Z, Spiegel D, Drevenšek G, et al. Marital status and survival in cancer patients: A systematic review and meta‐analysis. Cancer Med 2023; 12: 1685–708.
Peters R, Ee N, Peters J, Beckett N, Booth A, Rockwood K, et al. Common risk factors for major noncommunicable disease, a systematic overview of reviews and commentary: the implied potential for targeted risk reduction. Ther Adv Chronic Dis 2019; 10: 204062231988039.
Rock CL, Thomson C, Gansler T, Gapstur SM, Mccullough ML, Patel AV, et al. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention 2020; 70: 245–71.
de Pinho NB, Martucci RB, Rodrigues VD, D’Almeida CA, Thuler LCS, Saunders C, et al. Malnutrition associated with nutrition impact symptoms and localization of the disease: Results of a multicentric research on oncological nutrition. Clin Nutr 2019; 38: 1274–9.
Nagy S, Petrosky SN, Beckler MD, Kesselman MM. The Impact of Modern Dietary Practices on Cancer Risk and Progression: A Systematic Review. Cureus 2023.
Hanson S, Thorpe G, Winstanley L, Abdelhamid AS, Hooper L, Abdelhamid A, et al. Omega-3, omega-6 and total dietary polyunsaturated fat on cancer incidence: systematic review and meta-analysis of randomised trials. Br J Cancer 2020; 122: 1260–70.
Bundi, D., Chege, P., Kamuhu, R. (2024). Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. International Journal of Nutrition and Food Sciences, 13(5), 209-218. https://doi.org/10.11648/j.ijnfs.20241305.16
Bundi, D.; Chege, P.; Kamuhu, R. Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. Int. J. Nutr. Food Sci.2024, 13(5), 209-218. doi: 10.11648/j.ijnfs.20241305.16
Bundi D, Chege P, Kamuhu R. Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. Int J Nutr Food Sci. 2024;13(5):209-218. doi: 10.11648/j.ijnfs.20241305.16
@article{10.11648/j.ijnfs.20241305.16,
author = {Dorothy Bundi and Peter Chege and Regina Kamuhu},
title = {Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey
},
journal = {International Journal of Nutrition and Food Sciences},
volume = {13},
number = {5},
pages = {209-218},
doi = {10.11648/j.ijnfs.20241305.16},
url = {https://doi.org/10.11648/j.ijnfs.20241305.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijnfs.20241305.16},
abstract = {The global burden of non-communicable diseases remains unacceptably high and Kenya is among the countries experiencing an epidemiological transition from the communicable to non-communicable diseases. In Kenya, cancer is the second leading cause of non-communicable disease related mortalities after the cardiovascular diseases and Nyeri County is among the counties that are leading in this burden of non-communicable diseases. This study sought to assess the dietary practices of the cancer patients on chemotherapy at Nyeri County and Referral Hospital in comparison with the recommended dietary practices. Analytical cross-sectional study design was employed and the data on the dietary practices was collected using a 24-hour recall and a Food Frequency Questionnaire (FFQ). Sixty one percent of the respondents were female while 39% were male. Sixty one percent had acquired primary school education and half of the respondents survive on a monthly income of between 0-10,000. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. The mean energy intake of the respondents was 1068+- 520 Kcals which was not meeting the requirements as per the ESPEN clinical guidelines on cancer. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) and less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings recommended by the World Health Organization (WHO). Nutrition education and counselling is key in improving the dietary practices among the cancer patients. However, 44.19% had not received nutrition education and counselling regarding the appropriate diet to consume in the course of their treatment. This study found out that the dietary practices of the cancer patients do not meet the recommended clinical guidelines on cancer nutrition and almost half of the population had not received nutrition education and counselling services. Social and behavior change is one of the possible strategies that could be adopted to deliver nutrition information to the population, to improve the knowledge, attitude and dietary practices of cancer patients in Kenya, which in turn will improve their nutrition outcomes.
},
year = {2024}
}
TY - JOUR
T1 - Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey
AU - Dorothy Bundi
AU - Peter Chege
AU - Regina Kamuhu
Y1 - 2024/09/29
PY - 2024
N1 - https://doi.org/10.11648/j.ijnfs.20241305.16
DO - 10.11648/j.ijnfs.20241305.16
T2 - International Journal of Nutrition and Food Sciences
JF - International Journal of Nutrition and Food Sciences
JO - International Journal of Nutrition and Food Sciences
SP - 209
EP - 218
PB - Science Publishing Group
SN - 2327-2716
UR - https://doi.org/10.11648/j.ijnfs.20241305.16
AB - The global burden of non-communicable diseases remains unacceptably high and Kenya is among the countries experiencing an epidemiological transition from the communicable to non-communicable diseases. In Kenya, cancer is the second leading cause of non-communicable disease related mortalities after the cardiovascular diseases and Nyeri County is among the counties that are leading in this burden of non-communicable diseases. This study sought to assess the dietary practices of the cancer patients on chemotherapy at Nyeri County and Referral Hospital in comparison with the recommended dietary practices. Analytical cross-sectional study design was employed and the data on the dietary practices was collected using a 24-hour recall and a Food Frequency Questionnaire (FFQ). Sixty one percent of the respondents were female while 39% were male. Sixty one percent had acquired primary school education and half of the respondents survive on a monthly income of between 0-10,000. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. The mean energy intake of the respondents was 1068+- 520 Kcals which was not meeting the requirements as per the ESPEN clinical guidelines on cancer. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) and less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings recommended by the World Health Organization (WHO). Nutrition education and counselling is key in improving the dietary practices among the cancer patients. However, 44.19% had not received nutrition education and counselling regarding the appropriate diet to consume in the course of their treatment. This study found out that the dietary practices of the cancer patients do not meet the recommended clinical guidelines on cancer nutrition and almost half of the population had not received nutrition education and counselling services. Social and behavior change is one of the possible strategies that could be adopted to deliver nutrition information to the population, to improve the knowledge, attitude and dietary practices of cancer patients in Kenya, which in turn will improve their nutrition outcomes.
VL - 13
IS - 5
ER -
Institute of Food Bioresources Technology, Dedan Kimathi University of Technology, Nyeri, Kenya
Biography:
Dorothy Kareainto Bundi is a Nutrition technologist at Dedan Kimathi University of Technology. She is a master’s student at Kenyatta University and holds a Bachelor’s degree from Egerton University, (2015).
Research Fields:
Non-communicable diseases and nutrition, Child and maternal nutrition
School of Health Sciences, Kenyatta University, Nairobi, Kenya
Biography:
Regina Kamuhu is a lecturer at Kenyatta University Department of Foods, Nutrition and Dietetics. She holds a PhD in Foods, Nutrition and Dietetics from Kenyatta University- 2016 and a Master’s degree from University of Panjab, India.
Research Fields:
HIV dyslipidaemia, Utilization of groundnuts/ peanut in treatment of lipid disorders in HIV and diabetes
Bundi, D., Chege, P., Kamuhu, R. (2024). Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. International Journal of Nutrition and Food Sciences, 13(5), 209-218. https://doi.org/10.11648/j.ijnfs.20241305.16
Bundi, D.; Chege, P.; Kamuhu, R. Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. Int. J. Nutr. Food Sci.2024, 13(5), 209-218. doi: 10.11648/j.ijnfs.20241305.16
Bundi D, Chege P, Kamuhu R. Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey. Int J Nutr Food Sci. 2024;13(5):209-218. doi: 10.11648/j.ijnfs.20241305.16
@article{10.11648/j.ijnfs.20241305.16,
author = {Dorothy Bundi and Peter Chege and Regina Kamuhu},
title = {Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey
},
journal = {International Journal of Nutrition and Food Sciences},
volume = {13},
number = {5},
pages = {209-218},
doi = {10.11648/j.ijnfs.20241305.16},
url = {https://doi.org/10.11648/j.ijnfs.20241305.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijnfs.20241305.16},
abstract = {The global burden of non-communicable diseases remains unacceptably high and Kenya is among the countries experiencing an epidemiological transition from the communicable to non-communicable diseases. In Kenya, cancer is the second leading cause of non-communicable disease related mortalities after the cardiovascular diseases and Nyeri County is among the counties that are leading in this burden of non-communicable diseases. This study sought to assess the dietary practices of the cancer patients on chemotherapy at Nyeri County and Referral Hospital in comparison with the recommended dietary practices. Analytical cross-sectional study design was employed and the data on the dietary practices was collected using a 24-hour recall and a Food Frequency Questionnaire (FFQ). Sixty one percent of the respondents were female while 39% were male. Sixty one percent had acquired primary school education and half of the respondents survive on a monthly income of between 0-10,000. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. The mean energy intake of the respondents was 1068+- 520 Kcals which was not meeting the requirements as per the ESPEN clinical guidelines on cancer. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) and less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings recommended by the World Health Organization (WHO). Nutrition education and counselling is key in improving the dietary practices among the cancer patients. However, 44.19% had not received nutrition education and counselling regarding the appropriate diet to consume in the course of their treatment. This study found out that the dietary practices of the cancer patients do not meet the recommended clinical guidelines on cancer nutrition and almost half of the population had not received nutrition education and counselling services. Social and behavior change is one of the possible strategies that could be adopted to deliver nutrition information to the population, to improve the knowledge, attitude and dietary practices of cancer patients in Kenya, which in turn will improve their nutrition outcomes.
},
year = {2024}
}
TY - JOUR
T1 - Dietary Practices of Cancer Outpatients at Nyeri County Referral Hospital, Kenya; A Cross Sectional Survey
AU - Dorothy Bundi
AU - Peter Chege
AU - Regina Kamuhu
Y1 - 2024/09/29
PY - 2024
N1 - https://doi.org/10.11648/j.ijnfs.20241305.16
DO - 10.11648/j.ijnfs.20241305.16
T2 - International Journal of Nutrition and Food Sciences
JF - International Journal of Nutrition and Food Sciences
JO - International Journal of Nutrition and Food Sciences
SP - 209
EP - 218
PB - Science Publishing Group
SN - 2327-2716
UR - https://doi.org/10.11648/j.ijnfs.20241305.16
AB - The global burden of non-communicable diseases remains unacceptably high and Kenya is among the countries experiencing an epidemiological transition from the communicable to non-communicable diseases. In Kenya, cancer is the second leading cause of non-communicable disease related mortalities after the cardiovascular diseases and Nyeri County is among the counties that are leading in this burden of non-communicable diseases. This study sought to assess the dietary practices of the cancer patients on chemotherapy at Nyeri County and Referral Hospital in comparison with the recommended dietary practices. Analytical cross-sectional study design was employed and the data on the dietary practices was collected using a 24-hour recall and a Food Frequency Questionnaire (FFQ). Sixty one percent of the respondents were female while 39% were male. Sixty one percent had acquired primary school education and half of the respondents survive on a monthly income of between 0-10,000. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. The mean energy intake of the respondents was 1068+- 520 Kcals which was not meeting the requirements as per the ESPEN clinical guidelines on cancer. The dietary patterns identified from the research were, excessive consumption of foods from the starchy foods and the fats category (65.1%) and less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings recommended by the World Health Organization (WHO). Nutrition education and counselling is key in improving the dietary practices among the cancer patients. However, 44.19% had not received nutrition education and counselling regarding the appropriate diet to consume in the course of their treatment. This study found out that the dietary practices of the cancer patients do not meet the recommended clinical guidelines on cancer nutrition and almost half of the population had not received nutrition education and counselling services. Social and behavior change is one of the possible strategies that could be adopted to deliver nutrition information to the population, to improve the knowledge, attitude and dietary practices of cancer patients in Kenya, which in turn will improve their nutrition outcomes.
VL - 13
IS - 5
ER -