3. Results
In attempting to try to understand the essence of depression, depression and self-destructiveness, the threshold for seeking treatment for depression and staying in treatment, and the contents of depression therapy and the individual monitoring of depression, it is essential that we form different heading lists. The accompanying chapters contain examples of their definitions with the help of the 7x4 field. They also describe other results that can be achieved through this method. Stars in parenthesis (*) always refer to parts and definitions of the 7x4 field.
3.1. Dealing with the Essence of Depression
An important thesis, the depression process can begin already from childhood experiences, claims Aaron Beck. He defined depression through the following key points
| [4] | Beck, A. (1971) Cognition, affect and psychopathology. Archives of General Psychiatry 24, 495- 500. |
[4]
: Loneliness in the form of absent parents, for example, surely has an effect. Disappointments as well as other punitive experiences in human relations are part of the depression process. There is much empirical evidence about the effects of experiencing guilt in depression. Losses in human relations are almost self-evident events that cause depression. These are represented in the squares marked with stars in the attached 7x4 field (
Table 1):
Table 1. Cornerstones of Mental Health.
Effectors: | A Human relations | B Bodily functions | C Rational functions | D View of Life |
1) Lonelinesses | * | | | |
2) Models | | | | |
3) Stresses | | | | |
4) Punishments, etc | * | | | * |
5) Losses | * | | | |
6) Avoidances | | | | |
7) Changes | | | | |
Beck's classification can be developed more broadly with the 7x4 field. Beck himself extended the bases of depression toward stresses
| [7] | Beck, A. (1982) Cognitive therapy of depression, new perspectives. In the work, Clayton, P. &. Barret, J.(edit.) Treatment of depression: Old controversies and new approaches. 265-290. New York: Raven. |
| [3] | Barret, J. (edit) (1982) Treatment of depression: Old controversies and new approaches. New York: Raven. |
[7, 3]
. For instance, light therapy in treating depression is also related to bodily functions, their stresses and changes, or the improvement of a poor economic situation is related to rational stress. In addition, models related to human relationships have provided the following confirmation of the thesis that “partner anxiety is somehow contagious in a similar way to exposure to the bacillus”: Male-female couples (N= 1708, Finns aged 18-75) were followed. Episodes of major depression that occurred over a 12-month period were examined. The University of Michigan Composite International Diagnostic Interview (UM-CIDI Short Form) was used. The following was then observed, among other things: Regardless of other risk factors, spouses had a statistically significant risk of receiving a depression diagnosis
| [40] | Lindeman, S., Kaprio, J., Isometsä, E., Poikolainen, K., Heikkinen, M., Hämäläinen, J., Haarasilta, L., Laukkala, T. & Aro, H. (2002) Spousal resemblance for history of major depressive episode in the previous year. Psychological Medicine. 32(2): 363-7. |
[40]
.
In addition: Many artists have illustrated experiential aspects of life that can be found in the 7x4 field, which are also causes. For example, a depressed young person sighing in Finnish "juokse sinä humma, kun tuo taivas on niin tumma" ("Run on, my horse, the sky is getting dark") in this well-known Finnish song expresses a sense of negative loneliness related to restlessness (*) or the description of a serious conflict of emotions, "On lainaa ilon sekunnitkin" (Even seconds of joy are just on loan), presented in a well-known musical speaks about irrational stress (* problems of self-value) The poet Kahil Gibran in his poem "Seven times have I despised my soul" addresses the factors in his own way about the factors in the 7x4 field. Furthermore: Works of many visual artists can be understood to be examples of squares on the 7x4 field
| [33] | Heiska, J. (2018) Ennakoiva mielenterveystyö, käsikirja meille kaikille. Tampere: Mediapinta. |
[33]
. For instance, the works of the famous Finnish painter Albert Edelfelt and famous Swedish painter Carl Larsson contain examples of each square. Therefore, we can establish a link to art therapy used in the treatment of depression.
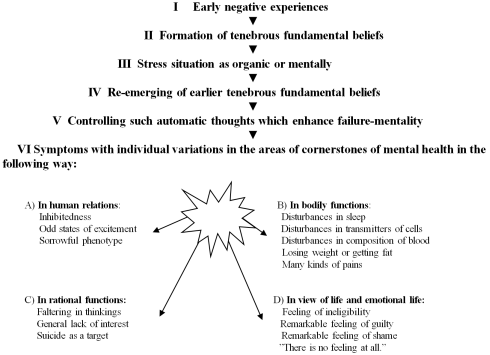
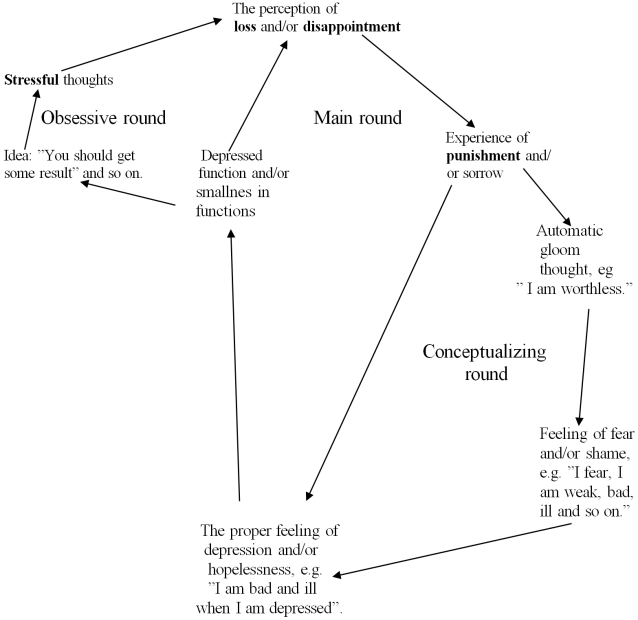
The stages of the depression process are connected to learning from examples (*human relations models) or other models for action (* worldview models) and through stress situations (*) can be placed in the 7x4 field in the following way:
Figure 1. The stages of the depression process.
For instance, early negative experiences in school create a negative model (*), "I am no good". This bleak basic belief will then surface and gain strength through difficulties in finding employment. In this way, automatic thoughts are formed in stressful situations in working life, and before long, the symptoms tell us we are reaching the cornerstone areas (* the four areas in question). The catalogue of symptoms in the picture is a summary of many studies on symptoms.
A follow-up study of female twins conducted in the state of Virginia also tells us about the stages. In it, the process of depression was organized under conclusions reached through correlation multipliers into tables
| [36] | Kendler, K., Gardner, C. & Prescott, C. (2002) Toward a Comprehensive Developmental Model for Major Depression in Women. American Journal of Psychiatry 159(7), 1133-1145. |
[36]
using an 18-square field. Its 13 frames can be included in the following squares of the 7x4 field relatively well (
table 2):
Table 2. Cornerstones of Mental Health.
Effectors: | A Human relations | B Bodily functions | C Rational functions | D View of Life |
1) Lonelinesses | * | | * | |
2) Models | * | | * | * |
3) Stresses | * | * | * | * |
4) Punishments etc. | * | | | |
5) Losses | * | | | |
6) Avoidances | | | | |
7) Changes | * | | * | |
The last five are neuroticism, low self-esteem, proneness to anxiety, disturbing behaviour, and the abuse of controlled substances.
Here we find the area of observation of the causal factors behind depression, other disturbances or illnesses, which will of course have their own fields of causes. For example, the development of low self-esteem can be identified under relevant stages in the 7x4 field. Or alternatively: Under possibilities of avoidance, the grid has no stars, but the abuse of controlled substances is known to be an illness and/or avoidance reaction (*). A group of Finnish researchers confirms this
| [55] | Torikka, A., Kaltiala-Heino, R-K., Rimpelä, A., Rimpelä, M. & Rantanen, P. (2001) Depression, drinking, and substance use among 14 to 16 year-old Finnish adolescents. Nordic Journal of Psychiatry 55(5), 351-357. |
[55]
through material from 14-16-year-olds, which supports the claim that the use of alcohol increases depression, but that depression does not increase the use of alcohol. For instance, diabetes as a loss of bodily functions (*) is closely connected to depression
| [15] | Eriksson, J. (2001) Altistaako masennus tyypin 2 diabetekselle. Diabetes ja lääkäri, September. |
[15]
.
When we ask whether or not depression is generally an illness, a subdivision of bipolar mental illness, an inevitable stage in recovery from psychosis, deep exhaustion, laziness, a part of the opposite of happiness, a part of the vicious circle of anxiety and depression, or, for example, a significant post-childbirth condition, the 7x4 field allows us to define the essence of depression in the following manner: A) K. Fulford's view is important both socially (*) and sociologically: When is grief following the loss of a loved one defined as an illness
| [16] | Fulford, K. (1989) Moral Theory and Medical Practice. Cambridge University Press. Cambridge. |
[16]
. B) The somatic (*) view is important in the clinical definition of depression as an illness and also, for instance, in examining the interaction between smoking and depression. C) Health care funding (*) and single-visit billing greatly depend on the clinical definition of depression. D) In ethical conclusions (*) related to depression
| [39] | Lewinsohn, P., Mischel, W., Chaplin, W. & Barton, R. (1980). Social competence and depression: The role of illusory self-perception’s. Journal of Abnormal Psychology 89, 2103-2112. |
[39]
, we encounter the following research result: When test subjects themselves and external observers both assess social competency, those experiencing depression and those living in that realm of perception self-asses, on average, more accurately than non-depressives . Thus, we have to face worldview-related and irrational stress (*). It is difficult to work with an accurate ethical sense of reality, which turns out to be bad or poor.
Self-healing (*), placebo treatments (*), and the side effects of treatments (*) are also part of the processing of the essence of depression. For example, already in the 1980s, research on depression produced the following results: antidepressants always have some stressful side effects (* negative impact on blood consistency, general fitness etc.), and studies even showed equally good treatment results with the use of side effects producing placebos as with actual antidepressants
| [53] | Thomson, R. (1982) Side effects and placebo amplification. British journal of psychiatry 140. |
[53]
.
However, it should be mentioned at this point that the side effects of the latest antidepressants have been reduced to the point where significant relief has been achieved within an average of 72 hours
| [8] | Berman, R., Cappiello, A., Anand, A., Oren, D., Heninger, G., Charney, D. & Krystal, J. (2000) Antidepressant effects of ketamine in depressed patients. Biological Psychiatry Vol. 47, Issue 4, 15 February, 351-354. |
[8]
.
In addition to all the above, the essence of depression also includes an evolutionary point of view (changes) (*): depression as a phenomenon with which materials inadequate for development are filtered out. For example, the following experiments have been conducted in laboratories with rats: Rats are given a certain tone before a pleasant experience, i.e. a proper portion of food. Then, before a negative experience, i.e. going without food or being exposed to a disturbing noise, the rats hear a different tone. When hungry rats are then given a tone in the middle of those tone signals, some react in the direction of the positive experience (continue to press the lever), while others react in the direction of the negative experience (stop trying). This is very similar to human depression behavior, where the essential thing is the following: The patient is tired and uses his last strength to make his own situation worse.
3.2. Depression and Self-destructiveness
According to different estimates, 30-40% of self-destructive people are not depressed, and in treatment practices, suicide is often discovered when depression has partly receded. Suicidal thoughts can emerge during treatment, and defining suicide is tricky as a person can take their life in order to save someone else or have an accident that appears to be a suicide. Furthermore, suicide attacks are often the result of brainwashing, and therefore not actual suicides. Also, the claim that euthanasia is not suicide is denied by many. In this sense, the definitions should include the following thought structures
| [41] | Litman, R. (1961) When Patients Commit Suicide. Psychotherapy of America 19, 570-576. |
[41]
: 1) I wish to atone or sacrifice according to a certain worldview. 2) I wish to seek revenge or punishment even beyond the grave. 3) I wish to rejoin my lost beloved. 4) I wish to escape/sleep because I have no more strength. 5) I wish to be born again, begin a new life, or something related. These can be placed in the following squares (
table 3):
Table 3. Cornerstones of Mental Health.
Effectors: | A Human relations | B Bodily functions | C Rational functions | D View of Life |
1) Lonelinesses | | | | |
2) Models | | | | 1* |
3) Stresses | | | | |
4) Punishments etc. | | | | 2* |
5) Losses | | | | 3* |
6) Avoidances | | | | 4* |
7) Changes | | | | 5* |
The equivalents in the 7x4 field's verification list are thus 1) Models for handling feelings of guilt, 2) Situations of unforgiveness, 3) Loss of identity, 4) Opportunities to avoid thinking about life's so-called big questions and 5) Emergence of new ideologies in the life field. These thought structures naturally include individual specifications. For example, regarding worldview-related avoidances, we can make the following clarification: The sufferer emphasizes to those close to them their life-affirming faith in God but fundamentally thinks the following: "I am a terrible burden that I ought to remove by killing myself, which is a way to receive God's grace".
It is also significant that, for example, according to one official diagnostic manual (ICD-11), people with depression also commonly have problems with their outlook on life, which resemble the five points presented.
What follows are phrases from those who went through their suicide, spoken in significant situations and gathered from recollections of those close to them
| [45] | Mikkelin läänin työryhmä (1988) Toteutuneiden itsemurhien tapausselostuksia vuosilta 1987 - 1988. Julkaisematon raporttikokoelma Suomen itsemurhaprojektista. |
[45]
. The phrases give an even more accurate picture of the organization of the thought structures of self-destructive people:
1) Loneliness (*) related to the following: "Father, take me away". "I am a rock in the open sea". "I have no place in the business world, or in the city". "Because I feel that even God is not helping".
2) Distorted models of thought (*) are the following: "If the sauna (the steam bath that is a culturally and spiritually significant place for Finns), booze and women do not help, then the disease is fatal". "I have my own solutions" (in seeking treatment). "Until I do not see you again" (phrase repeated while leaving the rehabilitation clinic). "What if something happens to me" (after receiving prescriptions and assurances that there is nothing bad happening in the body). "I will no longer be torn apart in operations, I wish to die as a whole". He used obscure allusions, to which no clarifications or explanations were received.
3) Exclamations belonging to states of excessive stress (*) are "I can't take it anymore" and "I don't want to live, as I have so many faults".
4) Experiences of punishment/disappointment (*) involve the following: "I am so ugly and skinny" (viewing oneself in front of the mirror). "Shut your mouth. I will shoot".
5) The following relates to loss (*): "Now the ridge of our home's roof has cracked". "I had the strength to live for mom's sake". "Dad, why did you leave me!"
6) Defensiveness (* main class avoidances) is reflected in the following: "I have completed my tasks in this world". "I will not attend that court". "You can take from there" (referring to a bank statement). "It won't be needed much longer" (about a book purchased hymns).
7) Related to change (*) "I want to be with Dad" and "take good care of S".
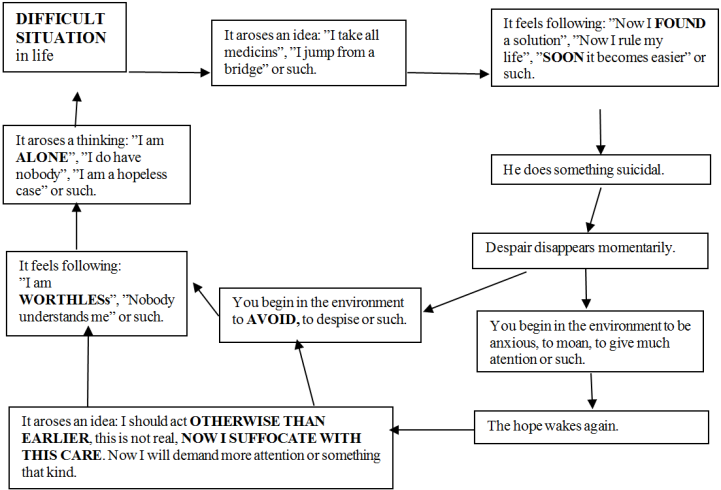
Also, this chart of the vicious circles of self-destruction
| [44] | Meretoja, P. & Laakso, J. (2002) Itsemurhaan altistavat kognitiiviset mallit. Suomen Lääkärilehti 49-50, 5045-5048. |
[44]
contains parts of the 7x4 field. They are indicated in capital letters in the following figure:
Figure 2. The chart of the vicious circles of self-destruction.
This vicious circle process begins at the point of a difficult situation (*), continues to the point "despair disappears momentarily", and then continues along three different paths.
3.3. Threshold for Seeking Help and Remaining in Treatment in the Treatment of Depression
B. Brenner, for one, has described the following conformity in depression processes: Of depressed people, a clear minority seeks professional help for their depression, but they do seek it for other problems
| [11] | Brenner, B. (1985) Continuity between the presence and absence of the depressive syndrome. Presentation at the APHA annual congress (113) in Washington, in November. |
[11]
. These avoidance functions (* mistakes, side effects or other factors in treatment that enable an avoidance reaction) can be clarified with the following examples from suicide cases
| [45] | Mikkelin läänin työryhmä (1988) Toteutuneiden itsemurhien tapausselostuksia vuosilta 1987 - 1988. Julkaisematon raporttikokoelma Suomen itsemurhaprojektista. |
[45]
:
Human relations (*) related:
-- In his last year, he visited the health center only once -- and then only during the Sunday reception hours with his partner. Only insomnia and tiredness issues were revealed. They did have serious problems with sex.
-- He cried out for help only among friends -- and the cries were masked. He told the General Practitioner only about his urination problems and shoulder and neck muscle pains. There were two visits to the school/university nurse, but without any problems related to depression.
Bodily functions, physical activity and exercise (*) related:
-- He had annual treatments for prostate problems that he did not reveal even to his wife.
Rational activity (*) related:
-- He had not visited any health care facilities in ten years. While drunk, he nonetheless often barged into his siblings' homes, asking for help when in a rage, and was naturally turned away.
-- There were 14 visits to the social welfare office during his final year and only due to financial matters.
-- He complained to his mother about a migraine, but no note of a migraine exists in the treatment centre records.
Worldview activities (*) related:
-- He visited a spiritual healer, unsuccessfully, to receive help for his headaches, which had been treated at the neurology clinic two months earlier.
-- He got in touch with a former classmate, a priest, who realized too late that these were calls for help.
When planning actions regarding seeking treatment for depressed people and remaining in treatment, the examples above and their organisation are central.
In addition, there is the organisation into the cornerstones of mental health. For example, the monitoring of medical treatment related to bodily functions (*) tells us that unmedicated depressed people (N= 484) and medicated depressed people suffering from medium depression (N= 3671) have states of health that allowed the following conclusion: That depression is not recognized in basic health care does not lead to serious negative consequences
| [17] | Goldberg, D. (1998) The effect of detection and treatment on the outcome of major depression in primary care. British Journal of General Practice 48. |
| [48] | Pigott, A., Leventhal, G., Alter, J. & Boren, J. (2010) Efficacy and Effectiveness of Antidepressants: Current Status of Research. Psychotherapy and Psychosomatics 79. |
[17, 48]
.
Furthermore, the organization of seeking out treatment should take into account psychoanalytic research results on transference
| [14] | Enckell, H. (2012) Terapiaprosessin teoriaa. A chapter in the article Psykoanalyysi ja psykoanalyyttiset terapiat (29-32) in book Huttunen, M. & Kalska, H. (edit.) Psykoterapiat. Porvoo: Bookwell oy. |
[14]
, which reveal the following irrationality (*): the care relationship starts to develop even before meeting the person treating the depression. All in all, several aspects need to be considered in the organization of seeking treatment and remaining in it, and the 7x4 field is also necessary.
3.4. The Contents of Depression Therapy
Already the Old Testament (Job 16: 2-5) tells us of the exclamations of a depressed Job, which corresponds to depression therapy's seven important starting positions in the following manner:
1) I have heard these words before! (the alone-together phenomenon) (*).
2) Well, that's some consolation! You just add to my pain! (wrong model of approach) (*).
3) Are you done or are you still talking nonsense! (the stress of beginning) (*).
4) Why do you always disagree with me! (experiences of disappointment in treatment or treatments) (*).
5) I could speak just like that too! (bad examination of losses) (*).
6) If you were in my position, just how wisely I would speak to you! With my condolences, I would commiserate to your accident. (bad examination of defenses) (*).
7) I would encourage you with kind words. I would console you with the speech from my lips! (little hope for the future) (*).
This description classifies in a significant way the old insight regarding the processing of the internal speech of the depressed. It may be important that nowadays such internal speech is also linked to neuropsychology.
Current treatments of depression certainly fall under many labels. The rational-emotive learning therapy, gestalt therapy, reality therapy, logotherapy, medical treatment, or even psychoanalysis and spiritual healing tell us surprisingly little about the caretaker's "official" school of thought. The analyses of videotaped therapy sessions strongly point to this
| [1] | Ablon, J., Levy, R., Katzenstein, T. (2006) Beyond brand names of psychotherapy: Identifying empirically supported change processes. Psychotherapy: Theory, Research, Practice, Training 43(2), 216-231. |
[1]
. However, depression therapy's four sections and the seven active elements of a psychotherapist's actions can be specified in a 7x4 form in the following way:
A) The language used:
a) Shared concepts or form of expression through which the sufferer and the therapist understand each other.
b) Shared concepts or form of expression through which the therapist can communicate with other experts about the progress and results of the therapy.
B) Discovery
a) New insights, reshapings and procedures
b) Mental activity, from which insight, reshaping or other such discoveries come.
C) Structure:
a) The therapist and patient's meeting places, meeting situations, and meeting times.
b) The theoretical basis, classification method or the like of a therapist's actions.
D) Mood:
a) Opportunities to progress in the internal actions between the therapist and the client.
b) Operational and confronted values, limits of actions and the like.
- - -
1) Unconditional and respectful attitude: For instance, taking respect into account in the realization of the initial interview.
2) Empathy: For example, dealing with transference, i.e. the transfer of feelings felt toward a person.
3) Acknowledgement of realities and limits: For instance, the so-called dynamic and cognitive handling of problems and their limitations.
4) Striving for sincerity: For example, utilizing speech from different levels of the ego.
5) Setting for confrontation: For example, utilizing desensitisation or the so-called thought-stop practise.
6) Avoidance of games: During sessions, clients easily play, for example, the 'yes yes - but' game, in which excuses are made. For example, suggestions to increase exercise are often met with sentences such as 'yes, but there is this...' and a certain victory is gained from bewildering the person who suggested. This is one of the so-called Berne's games that was handled in therapy sessions as early as the 1950s.
7) Striving for concreteness: For example, utilizing symptom control programs. In addition, depression therapy's general principles once again manifest a functioning 7-part classification:
a) In the handling of individual beliefs (*) the attempt is to create an atmosphere of understanding.
b) A psychotherapist's main visible forms of action (*) are asking, nodding, explaining and commenting.
c) The more difficult (*) the depression or self-destructive effort, the more active the carers.
d) Judgmental/ stigmatizing (*) utterances are minimized.
e) Interpretative utterances are minimized, so that trust is not lost in the beginning (*).
f) Utterances intended as means of adjustment, such as 'cheer up' are terrible suggestions to a depressed person. They are not to be presented.
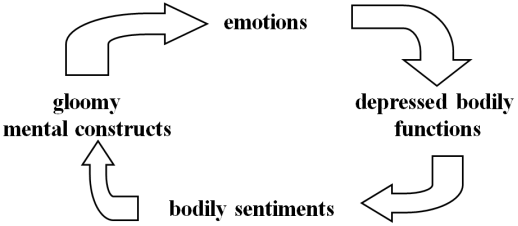
g) In the treatment combining physical well-being with psychotherapy, it is clarified that depression essentially includes bleak thought structures and the functions of a depressed body
| [49] | Radloff, L. (1977) The CES-D Scale: a self-report depression scale for research in the general population. Applied Psychological Measurement 1, 385-401. |
[49]
. Through the emotions and bodily sensations, they form a stressful situation (*), in which bleak thought structures affect depressed bodily functions and vice versa. The vicious circle in question is the following:
Figure 3. The vicious circle in depression.
In treating depression, the vicious circle is slowed down with medication regarding the bodily functions, and with psychological means regarding the depressed thought structures. It is also significant that the vicious circle in question operates in the case of rational stress (*) in the following way: assistance event -|> economic plan -> financial resources -> spent money -> assistance event. Therefore, a bleak assistance event, in which the one who assisted or the one paying for the assistance feels "pointlessness" in the beginning, and this may deprive financial resources from another assistance attempt, that nonetheless is acutely needed.
The psychotherapy of depression also manifests much of the content of the 7x4 field. The first example of classification is this list of problems compiled in co-operation with a sufferer (* situations relating to the handling of mutual issues) about problematic symptoms, life situations, thoughts and feelings of hopelessness.
Human relations (*): Difficulty in accepting the break-up of a romantic relationship, difficulty in surviving alone (*) from the break-up and difficulty in finding a satisfactory intimate relationship.
Bodily functions & exercise/movement (*): Stressfulness of required daily mobility (*), inability in almost any activity and diminished sensations of pleasure in the body.
Thinking and immediate survival (*Subcategory of loneliness: lack of practical support from immediate surroundings that could be given for treatments): 'The inability to express myself is horrible', difficulty in expressing one's wishes and the mulling over of the same thoughts.
Values and worldviews (*): Feelings of inferiority and worthlessness as a human being, 'I am a bad mother' and 'no one likes me'.
Depression therapy also encourages the assessment of the proposed therapy model through certain questions and proposes alternative models of operation to replace bleakness (*). Especially Gestalt therapists explain many shaping phenomena. Also, the directing of thoughts to a positive future (*) is crucial, because then extreme hopelessness, i.e. losses (*), are dealt with as soon as possible, thus enhancing authoritativeness.
The therapist's level of directiveness, weekly issues, homework and feedback queries are parts of a plan in which the cognitive therapist deals with the object mode as well as the metacognitive mode with the language of the client, and the transaction analyst handles the adult-child system. In any case, the sufferer's independence (*), unambiguous rationality (*) and experiences of success (*) are central issues to be taken into consideration.
The cognition and consistent monitoring of distorted and bleak thoughts is connected to possibilities of avoidance on the part of the depressed (*). At this time, one seeks reasons for depression and ignores the thoughts immediately related to the depression. Thus, we encounter the following metaphor: "When the fire brigade arrives, what takes priority - putting out the flames or finding out who started the fire?". Furthermore, several therapy sessions are spent teaching that it is possible to think about thinking. It may be significant that this is also the special area of NLP therapy. The most significant automatic but adjustable thought distortions are models of rational and worldview activity (*), which therapy researchers deal with. For example, Beck has found a model
All or Nothing | [6] | Beck, A., Rush, A., Shaw, B. & Emery, G. (1979) Cognitive therapy of depression. New York: Guilford. |
[6]
, manifested in the exclamation 'Because I did not fully succeed, it makes no sense to try anymore.' His other findings include
overgeneralization | [5] | Beck, A. (1976) Cognitive therapy and emotional disorders. New York: International Universities Press. |
[5]
: 'Because I had a setback, I am a wholly failed human being and certainly not someone who has committed only one mistake.'
Self-blame | [6] | Beck, A., Rush, A., Shaw, B. & Emery, G. (1979) Cognitive therapy of depression. New York: Guilford. |
[6]
: 'Everything that goes wrong here is probably my fault.'
Hasty, crippling conclusions | [6] | Beck, A., Rush, A., Shaw, B. & Emery, G. (1979) Cognitive therapy of depression. New York: Guilford. |
[6]
are the following: "I can tell by the tones of their voices that they will abandon me.", and
Catastrophe thinking | [6] | Beck, A., Rush, A., Shaw, B. & Emery, G. (1979) Cognitive therapy of depression. New York: Guilford. |
[6]
means 'No point in trying because even worse things are coming.'
Other researchers have found the following:
I must-thinking | [13] | Ellis, A. & Grieger, R. (1972) Handbook of rational emotive therapy. New York: Springer. |
[13]
: 'I must do this so that at least someone could love me.'
Overstating and minimization | [10] | Burns, D. (1980) Feeling good. New York: Morrow. |
[10]
: 'My own failures are greater than those of others, and my successes smaller than those of others.'
The invalidation of positive aspects | [43] | Meichenbaum, D. (1977) Cognitive behavior modification. New York: Plenum. |
[43]
: 'As a whole, the successful experience is examined only in light of the one negative aspect, somehow staring at it.'
Automatic reduction of worth | [35] | Katajainen, A., Lipponen, K., & Litovaara, A. (2003) Voimavarat käyttöön. Helsinki: Duodecim. |
[35]
: 'She is just trying to be polite; it is part of her job.'
Emotion-focused reasoning | [18] | Goldman, R. & Greenberg, L. (1997) Caseformulation in process-experiental therapy. In book Eels, T. edit. Handbook of psychotherapy case formulation. New York: Guilford Press, 403. |
[18]
: 'I feel guilt - I must have done something wrong.'
These harmful models discovered by researchers are found through the sufferer's own examples.
Also, an action model (*), combining issues, is important in every therapy. For example, the sufferer is asked to describe unpleasant feelings and situations connected to them, and these are written on a large piece of paper. Then dark thoughts are observed and connected to feelings by drawing arrows between sentences.
Once the sufferer can identify and correct immediate and automatic negative thoughts related to situations of depression, we can move on to the so-called
dysfunctional basic assumptions | [6] | Beck, A., Rush, A., Shaw, B. & Emery, G. (1979) Cognitive therapy of depression. New York: Guilford. |
[6]
. They characteristically include the forming of obstacles, development of unnecessary anxiety and inadequate observations of reality - all of which are shared challenges among different approaches to therapy. For example, the belief "one must be strong and capable" displaces the essential aspect of vulnerability belonging to man. Also, changes in circumstances (*) are disregarded along with unnecessary extreme feelings. Therefore, depression and despair are more likely outcomes than sadness and grief. In addition, dysfunctionality manifests often without words and it does not diminish in solitude (*) or through one's own means. The following contain specifications of dysfunctionality:
1) There is hope for acceptance, respect, love and the like, but the feeling is that the needs for security or care cannot be dealt with when lonely (*), and they cannot even be expressed.
2) Overambitious norms of achievement (*) confuse one's goals. For example, the following thought structure: "I must always carry out my work so well that everyone respects me, or otherwise I am insignificant or worthless", would be the following in the non-dysfunctional form: 'No matter how well I perform my duties, everyone's appreciation is not guaranteed. "I can accept that one can only slightly influence the judgment of others".
3) While attending to the needs of others, one strives to cope (*) alone infinitely. For example, when reminded of childhood, that "one had to always please parents," the transference situation of pleasing is a stress (*) where the transfer of emotions brings continuous strain.
4) Holistic self-assessments such as stupid, childish or some diagnostic term one has heard reflect irrational thoughts of punishment (*), of which we have the following examples: "When I feel poorly, I get more rights and power to punish (*)", or "all those who try to love stupid me shall be punished" or "The Hell I know is better than the heaven I don't".
5) Human relations games that take the form of a vicious circle become apparent
| [9] | Berne, E. (1967) Kanssakäymisen kuviot. Jyväskylä: Gummerus. |
[9]
. For example, being lonely (*) relates to the square avoidances / human relations, (*) i.e. a certain human relations game where attention, empathy and the like that the depressed receives strengthens depression. This also illustrates depression treatment's special point of view. Empathy is often considered a natural part of treatment, but communality is more complicated here than is assumed.
These sections can be placed in the following areas marked with numbered stars (
table 4):
Table 4. Cornerstones of Mental Health.
Effectors: | A Human relations | B Bodily functions | C Rational functions | D View of Life |
1) Lonelinesses | | | | 1* |
2) Models | | | | 2* |
3) Stresses | | | | 3* |
4) Punishments etc. | | | | 4* |
5) Losses | | | | |
6) Avoidances | | | | 5* |
7) Changes | | | | |
Here, as well as in the previous placings in the field, we find a problem that can be described with a comment from part one: "When a person feels that their needs for safety or care are not met and cannot really be expressed, it is not a question of loneliness in the sense of worldview, but a misunderstanding or the like". The situation is similar to the scoring of projected test answers. There, the consensus among classifiers improves when scoring, i.e, placing answers into certain boxes, is studied. Equally, there are instructions for specifying the 7x4 field, which consider Carnap's principle from philosophy - "each can make their language their own" - and that different mental health workers have many concepts that can be understood in the same way. That is, those handling depression have their own premises and criteria of action, which they wish to maintain. We then encounter a situation known in the history of science as "only insiders are allowed to speak". What is then present is the square avoidances / rational activity, which clarifies the section 'the abuse possibilities of power'.
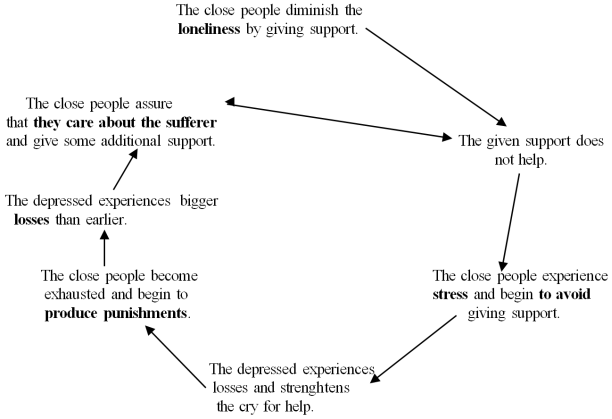
Different labels are used for the specifications for circular models (*), but an essential point of origin is the supporting role of close relatives (*)
| [42] | McDaniel, S. & Campbell, T. (1990) Family-oriented primary care. Springer, New York, 265. |
[42]
. The operation of this vicious circle contains elements that share the following with the 7x4 field (
figure 4):
The mind's internal circular model (*)
| [19] | Greenberg, L. & Paivio, S. (1997) Working with emotions in Psychotherapy. New York: Guilford Press. |
[19]
is also significant, as it contains an unconscious main vicious circle and a conscious attempt to conceptualize (What am I now?) or an adjustment method (*). In addition, it is related to an enforcement circle sidetrack (I have to, I have to!) in the following way:
Figure 5. The enforcement circle sidetrack (I have to, I have to!).
The acknowledgement of the dysfunctionality in these vicious circles through one's own examples is often a necessary prerequisite in the slowing down of other vicious circles. This is because the depressed person often deals with a large chunk all at once that deepens depression when left unstructured.
What is significant in these charts describing vicious circles is that although they are necessary from the perspective of treatment, they appear as complexities to the depressed and thus as new stress situations (*) that easily evoke a bleak thought like this: 'I fail even at this because I don't understand such figures'. This vicious circularity in the essence of depression and in the social surroundings of the depressed person brings out the following thesis: The core of the problem field of the depressed person cannot be understood by anyone else, though one can get close to it. It is still possible to help. Somehow there needs to be a slowing down of the vicious circle called general - specific - simple - general
| [54] | Thorngate, W. (1976) Possible limits on a science of social behavior. Kirjassa Strickland, I., Aboud, F. & Gerzen, K. (edit.) Social psychology in transition. New York: Plenum Press. |
[54]
: Person A makes a claim about the general principle regarding realising treatment. Then person B refutes this principle, calling for specifications. When A then presents specifications, the presentation becomes too complicated, and we must return to the general level.
The above points to the following theory: When every square of the 7x4 grid is taken into practice in the treatment of depression, we reach a new stage in the treatment of this big problem.
3.5. Monitoring Depression
In tests and interviews measuring depression, the contents of questions often reflect the seven classes of factors. For example, the short (lyhyt) mapping (kartoittava) depression (D) scale (asteikko) (LKDA) used in Finland has seven questions and, at the same time, parts of the 7x4 classification. Also, 20 segments of the more recent CES-D scale (Center for Epidemiologic Studies Depression Scale)
| [49] | Radloff, L. (1977) The CES-D Scale: a self-report depression scale for research in the general population. Applied Psychological Measurement 1, 385-401. |
[49]
can be easily similarly classified. An important example is provided by a study
| [58] | Williams, A., Hagerty, B. & Yousha, S. (2002) Factors Associated with Depression in Navy Recruits. Journal of Clinical Psychology 58(4), 323-337. |
[58]
, in which the depression of navy freshmen was monitored with tests that measured loneliness (*) (Loneliness Scale, RULS), models (*) (Sense of Belonging Inventory, SOB), stresses (*) (Perceived Stress Scale, PSS), losses (*) (List of Threatening Experiences, LTE), coping mechanisms (*) (Coping Inventory, CISS) and changes (*) (Global Assesment of Functioning, GAF). Results with good validity were gained precisely by these tests.
Measuring depression with the 7x4 as its basis also clarifies the following obscurity: The positive views of the patient about the received treatment correlate very little with the success of the treatment
| [57] | Viinamäki, H., Antikainen, R., Koivumaa-Honkanen, H., Honkalampi, K., Tanskanen, A., Kontkanen, J. & Hintikka, J. (2002) Masennuspotilaiden hoitotyytyväisyyskyselyt. Suomen Lääkärilehti 46(57) 4687-4691. |
[57]
. It could be that the mere feeling of loneliness (*), "no one knows what I feel", is the central aspect in the patient's mind when assessing the treatment, and so the question of whether the symptoms of depression have receded is left hidden in the questionnaires about treatment satisfaction
| [51] | Scott, J. (1993) Who does well with cognitive therapy? A four-year outcome of chronic major depressives treated with cognitive therapy and pharmacotherapy. Presentation at the European learning therapy conference in London, in September. |
[51]
.