Abstract
Early initiation of antenatal care (ANC) during the first trimester is a critical determinant of maternal and neonatal health outcomes. However, despite national and World Health Organization recommendations, first-trimester antenatal care (ANC1) attendance remains suboptimal in many rural settings in Uganda. At Nsiika Health Centre IV in Buhweju District, only 62% of pregnant women initiated ANC within the first trimester in 2025, indicating persistent gaps in timely maternal health service utilization. This paper presents a context-specific Theory of Change (ToC) developed to improve first-trimester ANC attendance at Nsiika Health Centre IV by addressing locally relevant socio-cultural, geographical, and health system barriers influencing maternal health-seeking behavior. This study aimed to design a practical, evidence-informed framework to guide district-level interventions for increasing early ANC uptake and improving maternal and neonatal outcomes. The ToC was developed using routine District Health Information Software (DHIS2) data, facility performance reviews, maternal health indicators, and district health priorities. Key barriers identified included delayed pregnancy confirmation, limited community awareness of early ANC benefits, long distances to health facilities, and inadequate community-level follow-up. The proposed framework integrates community-based strategies such as Village Health Team (VHT) engagement, home-based pregnancy screening using human chorionic gonadotropin (HCG) tests, targeted health education, and integrated community outreaches with facility-level interventions focused on improving service readiness, client experience, and continuity of care. The Theory of Change assumes that early identification of pregnancy, strengthened community facility linkages, and improved service responsiveness will lead to timely ANC initiation, increased institutional deliveries, and improved maternal and neonatal outcomes. By tailoring interventions to the Nsiika context, this ToC provides a scalable model for improving early ANC uptake in rural, resource-constrained settings and supports district efforts to increase ANC1 attendance to 95% by 2027.
|
Published in
|
Innovation (Volume 7, Issue 2)
|
|
DOI
|
10.11648/j.innov.20260702.11
|
|
Page(s)
|
21-29 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
First-Trimester Antenatal Care, Theory of Change, Community Based Health Innovation, Maternal and Child Health, Health Systems Strengthening, Rural Healthcare Delivery, Uganda
1. Introduction
Antenatal care (ANC) plays a pivotal role in safeguarding the health and well-being of expectant mothers and their unborn children. The early initiation of ANC, particularly during the first trimester, is associated with improved pregnancy outcomes, reduced maternal and neonatal mortality, and better management of pregnancy-related complications. Despite the known benefits of early ANC, many women particularly in underserved communities such as Nsiika face barriers that hinder timely access to essential healthcare services.
Nsiika Health Center IV (HC IV) serves as a critical healthcare facility in the region, offering maternal and child health services to the surrounding population. However, like many healthcare institutions in resource-constrained settings, Nsiika HC IV encounters challenges in ensuring early ANC attendance among pregnant women. Factors such as geographical barriers, socio-cultural beliefs, financial constraints, and inadequate healthcare infrastructure contribute to low ANC1 attendance rates at Nsiika HC IV.
Recognizing the urgency of addressing this issue and the potential to significantly improve maternal and neonatal health outcomes, a theory of change is proposed to increase ANC1 attendances during the first trimester at Nsiika HC IV. This theory aims to comprehensively address the multifaceted barriers and facilitators influencing maternal healthcare-seeking behaviors in the local context. Through stakeholder engagement, community resource mobilization, healthcare system strengthening, and targeted interventions, the theory seeks to create an enabling environment that supports pregnant women in seeking ANC early in their pregnancies.
This paper outlines the key components of the theory of change and its strategic approach to enhancing ANC1 attendance rates at Nsiika HC IV. Through collaborative efforts and evidence-based interventions, the theory endeavors to promote a culture of proactive maternal healthcare seeking behavior, ultimately contributing to improve maternal and child health outcomes in the community.
2. Background
Maternal mortality remains a significant public health problem globally
| [7] | World Health Organization. (2023). WHO recommendations on antenatal care for a positive pregnancy experience: Updated guidance 2023. Geneva: WHO. |
[7]
. Although substantial progress has been made in reducing maternal mortality over the last two decades, the number of maternal deaths worldwide remains unacceptably high. In 2017, an estimated 295,000 women died from complications related to pregnancy and childbirth. Worldwide, about 830 women die from pregnancy and childbirth-related complications every day. It has been reported that in 2015, about 303,000 women died during and following pregnancy and childbirth, and most of these deaths could have been prevented. The high number of maternal deaths in some parts of the world reflects inequities in access to health services and highlights the gap between the rich and the poor. Almost all maternal deaths (99%) occur in low- and middle-income countries (LMICs). More than half of these deaths occur in Sub-Saharan Africa (SSA) and about a third in South Asia. These are usually fragile, humanitarian, and post conflict areas
| [1] | Bright Opoku Ahinkorah, E. K.-A. (2021, January 28). Examining barriers to healthcare access and utilization of antenatal care services: evidence from demographic health surveys in sub-Saharan Africa. Springer Nature Link.
https://doi.org/10.1186/s12913-021-06129-5 |
[1]
. Despite the decline in the global trend of maternal mortality ratio (MMR), estimated at 5.4% between 1990 and 2015, this is not the case for SSA where the decline is still very low and has remained stagnant in some areas.
In Uganda, the maternal mortality ratio is estimated at 336 maternal deaths per 100,000 live births
| [6] | Uganda Bureau of Statistics & Ministry of Health Uganda. (2022). Uganda Demographic and Health Survey 2021–2022. Kampala, Uganda: UBOS and MOH. |
[6]
. It is recommended by the Ministry of Health (MoH) that all maternal deaths are reviewed, following the development of maternal death review (MDR) guidelines in 2004, based on WHO guidance “Beyond the numbers.
In the Ankole region
| [9] | Mbarara Regional Referral Hospital (MRRH). (2020). Maternal and perinatal death surveillance and response (MPDSR) audit report, 2015–2019. Department of Obstetrics and Gynaecology, Mbarara, Uganda. |
[9]
there were 44,592 livebirths and 164 maternal deaths between 2015 and 2019, with a ∼ 8918 births/year and MMR 375 per 100,000 live births. MMR ranged from 247 in 2016 to 606 in 2018. Audit forms were completed for 124/164 (76%) of cases. Causes of death are presented. Most women were <30 years (62%), multiparous (76%) and were referred from another health facility (71%). Most (35%) of the women experienced delay one. The majority (83%) were unstable or critical on arrival: 52% had an abnormal vital sign, 25% were unconscious and 7% were dead on arrival. Most deaths (41%) occurred within 24 hours of admission
| [5] | Ministry of Health Uganda. (2023). Uganda Health Sector Annual Performance Report 2022/2023. Kampala, Uganda: Ministry of Health. |
[5]
.
Most maternal deaths result from haemorrhages, sepsis, pre-eclampsia, unsafe abortion, and congenital disabilities. These complications can be prevented with appropriate maternal health services, including antenatal care (ANC).
Early initiation and adequate utilization of antenatal care (ANC) play a critical role in lowering maternal and perinatal mortality. In this study, early ANC attendance is defined as the first ANC contact occurring before 12 weeks of gestation, while optimal ANC refers to completion of at least four visits, in line with earlier World Health Organization (WHO) guidance. Timely and adequate ANC enables the early identification, prevention, and management of pregnancy-related risks and complications. It also provides an important platform for delivering proven interventions that improve maternal and neonatal outcomes, including health education, counselling on physiological changes and danger signs, immunization, nutritional support, prevention of anaemia and malaria, and interventions to prevent mother-to-child transmission of sexually transmitted infections.
Previously, WHO recommended a minimum of four ANC visits, with the first occurring in the first trimester. In 2016, this guidance was updated to a minimum of eight ANC contacts, as evidence showed that eight or more visits can reduce perinatal mortality by approximately eight deaths per 1,000 live births compared with four visits. Meeting this recommendation remains challenging, particularly in low- and middle-income countries (LMICs). Available evidence indicates that only about half of women in sub-Saharan Africa complete at least four ANC visits during pregnancy. Barriers to optimal ANC use include long distances to health facilities, limited access to information, poor service availability and quality, and socio-cultural norms and practices.
In response to these challenges, community-based approaches have been proposed as effective strategies to improve access to and uptake of maternal health services
| [2] | Million Phiri, J. M. (2025, March 25). Delay in timing of first antenatal care utilisation among women of reproductive age in sub-Saharan Africa: a multilevel mixed effect analysis. Journal of Health, Population and Nutrition.
https://doi.org/10.1186/s41043-025-00857-8 |
[2].
Such interventions include community mobilization, women’s support groups, community dialogues, household visits, and training of community health workers (CHWs). Existing studies demonstrate that these strategies can enhance breastfeeding practices and increase timely referrals for pregnancy-related complications and other maternal health services
| [4] | Olive Tengera, P. M.-M. (2025, May 21). Barriers hindering attendance and adherence to antenatal care visits among women in rural areas in Rwanda: An exploratory qualitative study. plosone. https://doi.org/10.1371/journal.pone.0323762 |
[4]
. For example, in northern Uganda, a CHW-led intervention involving Village Health Team training, household follow-up of women who missed ANC appointments, and structured community dialogues resulted in significant improvements in both ANC attendance and skilled birth attendance.
Early initiation of ANC in the first trimester is essential for the timely detection, prevention, and management of pregnancy-related conditions
| [7] | World Health Organization. (2023). WHO recommendations on antenatal care for a positive pregnancy experience: Updated guidance 2023. Geneva: WHO. |
| [10] | Ninsiima, M., Tumwine, J., & Lubogo, D. (2021). Early antenatal care attendance and its determinants among women in rural southwestern Uganda. International Journal of Women's Health, 13, 1065–1077.
https://doi.org/10.2147/IJWH.S312345 |
[7, 10]
. Nevertheless, wide regional and national variations persist across Africa in the proportion of women who begin ANC within the first trimester contact and the factors contributing to it. To create a suitable intervention plan, it is crucial to overcome these differences through single standard and uniform guidelines. This can be achieved through meta-analysis and systematic reviews. Thus, this systematic review aimed to assess the pooled prevalence of first-trimester ANC contact and the contributing factors at Nsiika HC IV.
Table 1. Statistical evidence.
Nsiika Health Centre IV |
Period | ANC 1st Visit for women | ANC 1st Visit for women (1st Trimester) |
2022 | 926 | 589 | 64% |
2023 | 845 | 317 | 38% |
2024 | 970 | 666 | 69% |
2025 | 850 | 640 | 75% |
Total | 3591 | 2212 | 62% |
| we are at 62% early attendance at Nsiika |
So our strategy is improve from 62% to 95% by the end of 2027
| [8] | Ministry of Health Uganda. (2025). District Health information Software (DHIS). |
[8]
.
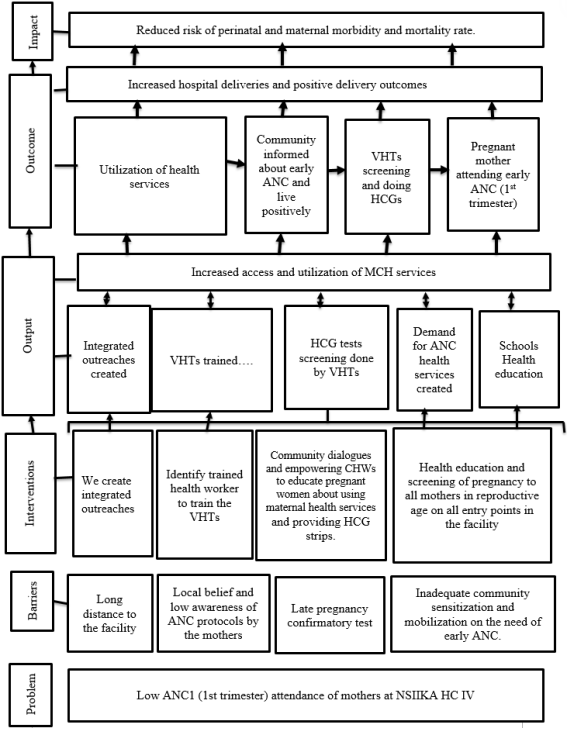
3. Problem
Nsiika HC IV is currently experiencing low attendance at ANC1 (first trimester) and several problems could have contributed to the problem.
Lack of Awareness and Education: Some pregnant women may not fully understand the importance of early ANC visits for their own health and that of their baby. This could be due to inadequate dissemination of information about the benefits and necessity of early antenatal care.
Geographical Barriers: The healthcare center might be inaccessible or distant for some pregnant women, especially in rural areas with limited transportation options. Poor roads or long travel distances can deter women from seeking early care.
Socioeconomic Factors: Financial constraints might prevent some women from seeking healthcare services, including ANC1. Costs associated with transport, consultations, or tests could pose significant barriers.
Cultural Beliefs and Practices: Cultural beliefs and traditional practices might influence women’s decisions about seeking healthcare early in pregnancy. Misconceptions or fear surrounding healthcare services, especially in the first trimester, could deter attendance.
Healthcare System Challenges: Long waiting times, inadequate facilities, or shortages of healthcare staff at the healthcare center can discourage women from attending ANC1. Poor quality of services might reduce trust in the healthcare system.
Lack of Support and Encouragement: Women might lack family or community support to attend ANC1 early in their pregnancy. Social norms or family obligations might prioritize other responsibilities over seeking healthcare.
Fear or Stigma: Fear or Stigma: Concerns about negative diagnoses or stigma may prevent women from seeking early care, particularly if they perceive healthcare settings as lacking confidentiality or privacy.
Addressing these problems requires a multifaceted approach, including community engagement, educational campaigns, improved accessibility, financial support or subsidies, culturally sensitive interventions, improvements in healthcare infrastructure, and enhanced support systems for pregnant women. Tailoring interventions to address these specific barriers can significantly increase ANC1 attendance at Nsiika HC IV.
4. Goal of Nsiika MCH Department
To improve maternal and neonatal health outcomes in Buhweju District by increasing timely first trimester antenatal care attendance through community based pregnancy identification and strengthened community facility linkages.
5. Theory of Change Narrative
The project is based on the theory that if there is increase in ANC1 (1st trimester) attendances at Nsiika HC IV will Increase hospital deliveries and positive delivery outcomes and in long run reduce risk of perinatal and maternal morbidity and mortality rate.
By creating integrated outreaches, Identify trained health worker to train the VHTs, Identify and train VHT in pregnancy screening by use of HCG strips and providing health education and screening of pregnancy to all mothers in reproductive age on all entry points in the facility that will lead to early identification of high risk mother.
Theory of change frame work
Complex interventions, including community health worker (CHW) programmes, must be guided by a clearly articulated theory of change that explains how intervention components are expected to produce desired outcomes
. Such a framework should explicitly outline the assumed causal pathways linking activities to results. The theory of change informing this study has been presented elsewhere; however, its core assumptions are summarized here. The intervention was designed on the premise that CHW-led home visits and structured community dialogues would strengthen women’s engagement with antenatal care (ANC), with particular emphasis on initiating care early in pregnancy and completing at least four facility-based ANC visits.
This effect was expected to occur through multiple, reinforcing mechanisms. First, CHWs provided targeted counselling to improve knowledge of ANC and enhance motivation to seek care. Second, women were informed about the availability and location of nearby health facilities offering ANC services, reducing informational barriers to access. Third, repeated household contacts acted as timely prompts for women who had already intended to attend ANC or deliver at a health facility. Finally, CHWs were anticipated to influence social norms by reinforcing the importance of ANC and other maternal health services within the community.
Collectively, these mechanisms were hypothesized to result in more timely initiation of ANC and increased frequency of visits compared with standard care.
Assumptions informing the Nsiika MCH Department TOC
The intended impact of the Nsiika MCH Department is to reduce risk of perinatal and maternal morbidity and mortality rate.
The following assumptions must be met for Nsiika MCH Department impact to be achieved:
Mothers are empowered and are capable of assuming responsibility for own health needs. The following are preconditions for the empowerment of Mothers:
1) Accessibility: Women in the community can easily reach the healthcare center.
2) Awareness: The target population is aware of the importance of early ANC.
3) Perception: The community perceives early ANC1 at Nsiika HC IV as beneficial and trustworthy.
4) Community workers have strong ties and influence within the community.
5) Community workers understand the cultural context and barriers to accessing healthcare.
6) Community workers are trained and motivated to promote maternal health care.
7) Based on the positive health-seeking attitudes, Pregnant mothers will adhere to health facility appointments and benefit from scheduled various tests and other necessary treatment (HIV testing, HCG, HepB test).
8) As a result of regular clinic visits, pregnant mothers will benefit from routine monitoring of their health status.
9) The above assumption clarify why the Nsiika MCH Department program support mothers to receive on-going and support services and remain within the system and be monitored up to delivery.
For the Outcome: “Increased hospital deliveries and positive delivery outcomes” the following assumptions must be met for this outcome to be achievable:
1) Access to Healthcare Facilities: Assumption that pregnant individuals have reasonable access to healthcare facilities offering obstetric care services. This includes the availability of transportation, proximity of healthcare facilities, and infrastructure that supports safe and timely travel to hospitals.
2) Quality of Healthcare Services: Assuming that healthcare facilities provide quality obstetric care, including skilled birth attendants, necessary medical equipment, medications, and facilities to handle complications during delivery.
3) Community Awareness and Education: Assuming that the community is educated about the benefits of hospital deliveries and is aware of potential risks associated with home births or unassisted deliveries. This includes understanding the importance of skilled attendance during childbirth for maternal and neonatal health.
4) Cultural Acceptance and Practices: Assuming that cultural norms and practices do not significantly hinder hospital deliveries. Addressing any cultural barriers or traditional beliefs that discourage hospital deliveries is crucial.
5) Financial Accessibility: Assuming that the cost of hospital deliveries, including associated services and transportation, is not a significant barrier for pregnant individuals and their families.
6) Availability of Skilled Birth Attendants: Assuming that hospitals have a sufficient number of trained and qualified healthcare professionals, including midwives and obstetricians, to attend deliveries promptly and competently.
7) Referral and Emergency Services: Assuming that there is an established and efficient referral system in place to transfer high-risk pregnancies or emergency cases to higher-level facilities equipped to manage complications.
8) Post-Delivery Care and Support: Assuming that postnatal care and support services are available for both mothers and newborns after hospital deliveries to ensure a smooth transition back home and early detection of any health issues.
9) Community Trust in Healthcare Facilities: Assuming that the community trusts and has confidence in the healthcare facilities and personnel, encouraging them to seek institutional deliveries.
10) Governmental and Policy Support: Assuming that supportive policies and initiatives are in place, encouraging and incentivizing hospital deliveries, and ensuring the quality of maternal healthcare services.
6. Barriers
The following barriers result in this:
1) Long distance to the facility
2) Local belief and low awareness of ANC protocols by the mothers
3) Late pregnancy confirmatory test
4) Inadequate community sensitization and mobilization on the need of early ANC.
7. Discussion
Increasing ANC1 (first trimester) attendances at Nsiika HC IV requires a multifaceted approach that addresses the various barriers preventing pregnant women from seeking early antenatal care. Identifying these barriers is crucial, and they include geographical distance, lack of awareness about the importance of early ANC, cultural beliefs and practices, financial constraints, and perceived quality of healthcare services
| [1] | Bright Opoku Ahinkorah, E. K.-A. (2021, January 28). Examining barriers to healthcare access and utilization of antenatal care services: evidence from demographic health surveys in sub-Saharan Africa. Springer Nature Link.
https://doi.org/10.1186/s12913-021-06129-5 |
[1]
.
Community Engagement:
Involving the local community is essential for raising awareness and shaping positive attitudes toward early ANC. Community leaders, traditional birth attendants, women's groups, and religious institutions play pivotal roles in disseminating information, addressing misconceptions, and encouraging ANC1 attendance
| [2] | Million Phiri, J. M. (2025, March 25). Delay in timing of first antenatal care utilisation among women of reproductive age in sub-Saharan Africa: a multilevel mixed effect analysis. Journal of Health, Population and Nutrition.
https://doi.org/10.1186/s41043-025-00857-8 |
[2]
.
Healthcare System Strengthening:
Strengthening the healthcare system at Nsiika HC IV involves improving infrastructure, staffing, and service delivery to accommodate increased ANC1 attendance. This may include training healthcare providers in early pregnancy detection, providing adequate ANC resources, and ensuring the availability of essential medications and equipment.
Targeted Interventions:
Implementing interventions tailored to the community’s specific needs helps overcome barriers to ANC1 attendance. These may include mobile outreach clinics, community-based education programs, incentive schemes for early ANC seekers, and integration of ANC services with other healthcare programs.
Empowering Women:
Empowering women to take charge of their reproductive health is essential. Education on the importance of early ANC, family planning, and maternal nutrition enables women to make informed decisions about their healthcare needs.
Monitoring and Evaluatio:
Continuous monitoring and evaluation are crucial for assessing intervention effectiveness and making necessary adjustments. Tracking ANC1 attendance rates, conducting client satisfaction surveys, and collecting qualitative feedback from pregnant women provide valuable insights into progress.
Expected Outcomes:
Implementing the Theory of Change successfully is expected to significantly increase ANC1 attendance at Nsiika HC IV, resulting in improved pregnancy outcomes, reduced maternal and neonatal mortality, and overall better health for women and children in the community. Additionally, fostering a culture of early ANC-seeking behavior will contribute to long-term improvements in maternal healthcare utilization and overall community health.
In conclusion, increasing ANC1 attendance at Nsiika HC IV requires a collaborative effort involving the community, healthcare providers, and policymakers. By addressing barriers, implementing targeted interventions, and empowering women, the Theory of Change aims to create a supportive environment that promotes early antenatal care and ultimately enhances maternal and child health.
Figure 1. Theory of Change Frame work.
8. Interventions
Community Engagement and Education:
Strategy: Conduct community outreach programs, workshops, and health education sessions.
Activities: Organize health talks, distribute informational pamphlets, involve community leaders, and use media for awareness campaigns on the significance of early ANC.
Strategy: Provide comprehensive training and engage community workers as advocates for maternal health.
Activities: Conduct workshops/training on the importance of ANC1, communication skills, and cultural sensitivity. Empower them to disseminate accurate health information and address community concerns.
Community Mobilization and Awareness:
Strategy: Utilize community workers to mobilize and raise awareness.
Activities: Task community workers with organizing community meetings, home visits, and discussions about the benefits of early ANC1. Encourage them to use their networks to spread information effectively.
Improved Service Provision:
Strategy: Enhance the quality and convenience of ANC services.
Activities: Ensure sufficient staff, reduce waiting times, provide incentives (if possible), maintain cleanliness, and improve facilities at the healthcare center.
Follow-up and Reminders:
Strategy: Implement a system for follow-up and reminders.
Activities: Develop a reminder system (via SMS, phone calls, or community health workers) for upcoming ANC appointments to encourage attendance.
Home Visits and Personalized Support:
Strategy: Leverage community workers for personalized support.
Activities: Assign community workers to conduct home visits for pregnant women, offering guidance, addressing concerns, and emphasizing the importance of ANC1. Provide them with resources like informational materials or tools to aid discussions.
Addressing Barriers:
Strategy: Identify and mitigate barriers preventing ANC1 attendance.
Activities: Conduct surveys or interviews to understand reasons for non-attendance (e.g., cultural beliefs, transportation issues, cost barriers), then address these barriers (e.g., provide transportation support, address misconceptions through targeted education).
Feedback Loop and Collaboration:
Strategy: Establish a feedback mechanism and collaboration between healthcare providers and community workers.
Activities: Organize regular meetings between community workers and healthcare staff to discuss challenges, successes, and areas of improvement. Encourage community workers to share feedback from the community regarding ANC1 attendance barriers.
9. Monitoring and Evaluation
Study Design
This study adopts a mixed-methods implementation and evaluation design to assess the effectiveness of a context-specific Theory of Change aimed at increasing first-trimester antenatal care (ANC1) attendance at Nsiika Health Centre IV. The evaluation combines routine health service data analysis, process monitoring, and qualitative assessments to examine both outcomes and implementation fidelity.
Study Setting
The evaluation will be conducted at Nsiika Health Centre IV and its catchment communities in Buhweju District, southwestern Uganda. The facility serves a predominantly rural population with known geographical, socio-cultural, and health system barriers to early antenatal care utilization.
Data Sources
Quantitative data will be obtained from:
1) DHIS2 (ANC1 attendance, first-trimester ANC coverage, institutional deliveries)
2) HMIS registers (ANC, maternity, referral records)
3) VHT activity reports (pregnancy screening, HCG testing, home visits)
4) Client satisfaction survey tools
Qualitative data will be collected through:
1) Key informant interviews with health workers, VHTs, and facility in-charges.
2) Community feedback obtained during dialogues and barazas.
3) Support supervision and mentorship reports.
Outcome and Process Indicators
Primary outcome indicators include:
1) Proportion of pregnant women attending ANC1 in the first trimester.
2) Facility-based delivery rate.
Secondary process indicators include:
1) Number of women screened for pregnancy by VHTs.
2) Number of VHT home visits conducted.
3) Timeliness of ANC reporting.
4) Client satisfaction scores related to ANC services.
Data Collection and Analysis
Quantitative data will be analyzed using descriptive statistics to compare baseline and follow-up trends in ANC1 attendance and related indicators. Time-series comparisons will be made using routine monthly and quarterly DHIS2 reports.
Qualitative data will be analyzed using thematic content analysis to identify facilitators, barriers, and contextual factors influencing implementation and uptake of ANC1 services. Findings from qualitative and quantitative analyses will be triangulated to assess the coherence of the Theory of Change pathways.
Monitoring and Evaluation Framework
Monitoring will be conducted quarterly through DHT review meetings, support supervision visits, and routine performance reviews. The Theory of Change framework will be used as an analytical lens to assess whether proposed assumptions, outputs, and outcomes are achieved as intended.
Ethical Considerations
The evaluation will utilize routine program and health service data with no collection of personal identifiers. Community engagements will follow Ministry of Health guidelines, and informed verbal consent will be obtained for interviews and feedback sessions.
10. Indicators
Impact: Reduced risk of perinatal and maternal morbidity and mortality rate.
% of perinatal and maternal death registered in the reporting period
Outcome 1: Increased hospital deliveries and positive delivery outcomes
% of live birth in facility reported the reporting period
Numerator: Number of normal live birth at delivered in the facility
Denominator: Number of deliveries in the reporting period
Outcome 2: Utilization of health services.
% of mothers attending early ANC1 (1st trimester) services at the facility
Numerator: Number of mothers receiving preconception care services at the facility the reporting period.
Denominator: Number of mothers attending the facility for preconception care services in the reporting period.
Outcome 3: Community informed about early ANC1 and live positively
% mothers/ communities informed about the importance of attending early ANC1 and live positively
Numerator: Number of mothers in the reproductive age health educated about the importance of attending early ANC1.
Denominator: number of mothers in the reproductive age in Buhweju District
Outcome 4: VHTs screening and doing HCGs
Indicator 1: Percentage of pregnant women within the community screened by VHTs.
Indicator 2: Total number of screenings performed by VHTs within a specific period
Indicator 3: Accuracy rates of HCG tests conducted by VHTs compared to confirmatory tests at healthcare facilities.
Outcome 5: Pregnant mothers attending early ANCI
% of mothers attending early ANC1 (1st trimester) services at the facility
Numerator: Number of mothers attending early ANC1 (1st trimester) services at the facility the reporting period.
Denominator: Number of mothers attending the facility for ANC1 services in the reporting period.
Output:
1) Number of integrated outreaches created
2) Number of VHTs trained
3) Number of mothers screened for HCG eligibility
4) Number of mother eligible for HCG testing
5) Number of HCG test done
6) Number of school health education session conducted
7) Number of mothers attending early ANC1 in the facility
Community efforts towards change
Reduced reasons for non-attendance as identified through community feedback.
Increased ANC1 attendance rates attributable to community worker involvement.
Positive feedback from pregnant women regarding the support and information received.
Improved collaboration between community workers and healthcare providers.
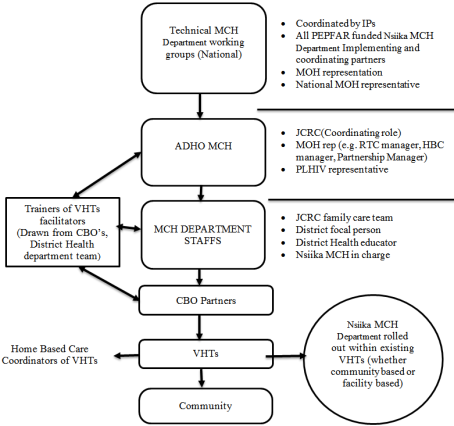
Figure 2. Implementation Model.
11. Conclusion
Early initiation and optimal use of antenatal care are essential for reducing maternal and perinatal morbidity and mortality, yet timely first-trimester attendance remains low in many low- and middle-income settings. These persistent barriers highlight the limitations of relying solely on facility-based approaches. Evidence indicates that community-based interventions particularly those involving community health workers, household follow-up, and community engagement can substantially improve early ANC uptake and continuity of care. Strengthening community–facility linkages through context-specific, scalable strategies, supported by routine monitoring, is critical for advancing WHO ANC recommendations and achieving sustainable improvements in maternal and newborn health.
Abbreviations
ANC | Antenatal Care |
TOC | Theory of Change |
DHIS | District Health Information System |
VHT | Village Health Team |
HCG | Health Center/Health Centre Grade |
LMICs | Low- and Middle-Income Countries |
SSA | Sub-Saharan Africa |
MMR | Maternal Mortality Ratio |
MOH | Ministry of Health |
MDR | Multi-Drug Resistant |
WHO | World Health Organization |
CHWs | Community Health Workers |
MCH | Maternal and Child Health |
HIV | Human Immunodeficiency Virus |
SMS | Short Message Service |
HMIS | Health Management Information System |
DHIS2 | District Health Information System 2 |
DHT | District Health Team |
CBO | Community-Based Organization |
JCRC | Joint Clinical Research Centre |
RTC | Regional Training Centre |
HBC | Home-Based Care |
PEPFAR | President’s Emergency Plan for AIDS Relief |
IPs | Implementing Partners |
Conflicts of Interest
The author declares no conflicts of interest.
References
| [1] |
Bright Opoku Ahinkorah, E. K.-A. (2021, January 28). Examining barriers to healthcare access and utilization of antenatal care services: evidence from demographic health surveys in sub-Saharan Africa. Springer Nature Link.
https://doi.org/10.1186/s12913-021-06129-5
|
| [2] |
Million Phiri, J. M. (2025, March 25). Delay in timing of first antenatal care utilisation among women of reproductive age in sub-Saharan Africa: a multilevel mixed effect analysis. Journal of Health, Population and Nutrition.
https://doi.org/10.1186/s41043-025-00857-8
|
| [3] |
Nishimwe C, M. G. (2021, Sep 30). Community- based maternal and newborn interventions in Africa2514-2539. Epub 2021 Mar 24. 17-18.
https://doi.org/10.1111/jocn.15737
|
| [4] |
Olive Tengera, P. M.-M. (2025, May 21). Barriers hindering attendance and adherence to antenatal care visits among women in rural areas in Rwanda: An exploratory qualitative study. plosone.
https://doi.org/10.1371/journal.pone.0323762
|
| [5] |
Ministry of Health Uganda. (2023). Uganda Health Sector Annual Performance Report 2022/2023. Kampala, Uganda: Ministry of Health.
|
| [6] |
Uganda Bureau of Statistics & Ministry of Health Uganda. (2022). Uganda Demographic and Health Survey 2021–2022. Kampala, Uganda: UBOS and MOH.
|
| [7] |
World Health Organization. (2023). WHO recommendations on antenatal care for a positive pregnancy experience: Updated guidance 2023. Geneva: WHO.
|
| [8] |
Ministry of Health Uganda. (2025). District Health information Software (DHIS).
|
| [9] |
Mbarara Regional Referral Hospital (MRRH). (2020). Maternal and perinatal death surveillance and response (MPDSR) audit report, 2015–2019. Department of Obstetrics and Gynaecology, Mbarara, Uganda.
|
| [10] |
Ninsiima, M., Tumwine, J., & Lubogo, D. (2021). Early antenatal care attendance and its determinants among women in rural southwestern Uganda. International Journal of Women's Health, 13, 1065–1077.
https://doi.org/10.2147/IJWH.S312345
|
Cite This Article
-
APA Style
Ssejjengo, K., Edyedu, I., Muhamya, P., Tukamushaba, C. (2026). A Theory of Change to Increase First Trimester Antenatal Care (Anc1) Attendance at Nsiika Health Centre IV, Buhweju District, Uganda. Innovation, 7(2), 21-29. https://doi.org/10.11648/j.innov.20260702.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Ssejjengo, K.; Edyedu, I.; Muhamya, P.; Tukamushaba, C. A Theory of Change to Increase First Trimester Antenatal Care (Anc1) Attendance at Nsiika Health Centre IV, Buhweju District, Uganda. Innovation. 2026, 7(2), 21-29. doi: 10.11648/j.innov.20260702.11
Copy
|
Download
AMA Style
Ssejjengo K, Edyedu I, Muhamya P, Tukamushaba C. A Theory of Change to Increase First Trimester Antenatal Care (Anc1) Attendance at Nsiika Health Centre IV, Buhweju District, Uganda. Innovation. 2026;7(2):21-29. doi: 10.11648/j.innov.20260702.11
Copy
|
Download
-
@article{10.11648/j.innov.20260702.11,
author = {Kennedy Ssejjengo and Isaac Edyedu and Philip Muhamya and Caroline Tukamushaba},
title = {A Theory of Change to Increase First Trimester Antenatal Care (Anc1) Attendance at Nsiika Health Centre IV, Buhweju District, Uganda},
journal = {Innovation},
volume = {7},
number = {2},
pages = {21-29},
doi = {10.11648/j.innov.20260702.11},
url = {https://doi.org/10.11648/j.innov.20260702.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.innov.20260702.11},
abstract = {Early initiation of antenatal care (ANC) during the first trimester is a critical determinant of maternal and neonatal health outcomes. However, despite national and World Health Organization recommendations, first-trimester antenatal care (ANC1) attendance remains suboptimal in many rural settings in Uganda. At Nsiika Health Centre IV in Buhweju District, only 62% of pregnant women initiated ANC within the first trimester in 2025, indicating persistent gaps in timely maternal health service utilization. This paper presents a context-specific Theory of Change (ToC) developed to improve first-trimester ANC attendance at Nsiika Health Centre IV by addressing locally relevant socio-cultural, geographical, and health system barriers influencing maternal health-seeking behavior. This study aimed to design a practical, evidence-informed framework to guide district-level interventions for increasing early ANC uptake and improving maternal and neonatal outcomes. The ToC was developed using routine District Health Information Software (DHIS2) data, facility performance reviews, maternal health indicators, and district health priorities. Key barriers identified included delayed pregnancy confirmation, limited community awareness of early ANC benefits, long distances to health facilities, and inadequate community-level follow-up. The proposed framework integrates community-based strategies such as Village Health Team (VHT) engagement, home-based pregnancy screening using human chorionic gonadotropin (HCG) tests, targeted health education, and integrated community outreaches with facility-level interventions focused on improving service readiness, client experience, and continuity of care. The Theory of Change assumes that early identification of pregnancy, strengthened community facility linkages, and improved service responsiveness will lead to timely ANC initiation, increased institutional deliveries, and improved maternal and neonatal outcomes. By tailoring interventions to the Nsiika context, this ToC provides a scalable model for improving early ANC uptake in rural, resource-constrained settings and supports district efforts to increase ANC1 attendance to 95% by 2027.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - A Theory of Change to Increase First Trimester Antenatal Care (Anc1) Attendance at Nsiika Health Centre IV, Buhweju District, Uganda
AU - Kennedy Ssejjengo
AU - Isaac Edyedu
AU - Philip Muhamya
AU - Caroline Tukamushaba
Y1 - 2026/05/28
PY - 2026
N1 - https://doi.org/10.11648/j.innov.20260702.11
DO - 10.11648/j.innov.20260702.11
T2 - Innovation
JF - Innovation
JO - Innovation
SP - 21
EP - 29
PB - Science Publishing Group
SN - 2994-7138
UR - https://doi.org/10.11648/j.innov.20260702.11
AB - Early initiation of antenatal care (ANC) during the first trimester is a critical determinant of maternal and neonatal health outcomes. However, despite national and World Health Organization recommendations, first-trimester antenatal care (ANC1) attendance remains suboptimal in many rural settings in Uganda. At Nsiika Health Centre IV in Buhweju District, only 62% of pregnant women initiated ANC within the first trimester in 2025, indicating persistent gaps in timely maternal health service utilization. This paper presents a context-specific Theory of Change (ToC) developed to improve first-trimester ANC attendance at Nsiika Health Centre IV by addressing locally relevant socio-cultural, geographical, and health system barriers influencing maternal health-seeking behavior. This study aimed to design a practical, evidence-informed framework to guide district-level interventions for increasing early ANC uptake and improving maternal and neonatal outcomes. The ToC was developed using routine District Health Information Software (DHIS2) data, facility performance reviews, maternal health indicators, and district health priorities. Key barriers identified included delayed pregnancy confirmation, limited community awareness of early ANC benefits, long distances to health facilities, and inadequate community-level follow-up. The proposed framework integrates community-based strategies such as Village Health Team (VHT) engagement, home-based pregnancy screening using human chorionic gonadotropin (HCG) tests, targeted health education, and integrated community outreaches with facility-level interventions focused on improving service readiness, client experience, and continuity of care. The Theory of Change assumes that early identification of pregnancy, strengthened community facility linkages, and improved service responsiveness will lead to timely ANC initiation, increased institutional deliveries, and improved maternal and neonatal outcomes. By tailoring interventions to the Nsiika context, this ToC provides a scalable model for improving early ANC uptake in rural, resource-constrained settings and supports district efforts to increase ANC1 attendance to 95% by 2027.
VL - 7
IS - 2
ER -
Copy
|
Download