Abstract
Introduction: Healthcare-associated bloodstream infections (HA-BSIs) represent a major cause of morbidity and mortality in neonatal intensive care units, particularly in low- and middle-income countries (LMICs). In Senegal, few data exist regarding the incidence, bacterial spectrum, and antimicrobial resistance patterns of HA-BSIs in neonates. This study aimed to describe the epidemiological and microbiological profile of healthcare-associated bloodstream infections in the neonatal unit of Dalal Jamm National Hospital in Senegal. Methods: We conducted a retrospective longitudinal study from October 2022 to July 2023 in the neonatal unit of Dalal Jamm National Hospital. All neonates with at least one positive blood culture obtained ≥48 hours after admission were included. Data were extracted from medical records and bacteriology registers and analyzed using R software v4.1.3. Categorical variables were expressed as frequencies, and the time to infection onset was described by the median and interquartile range. Results: Among 288 admitted neonates, 36 cases of HA-BSIs were recorded, yielding a cumulative incidence of 12.5% and an incidence density of 15.5 cases per 1 000 patient-days. The median time to infection was 6 days [IQR 2–13]. Prematurity and low birth weight (< 2 500 g) were observed in 53% of cases. A total of 38 pathogens were isolated, predominantly Gram-negative bacilli (65.8%), mainly Enterobacter cloacae (18.4%), Klebsiella pneumoniae (15.8%), and Escherichia coli (13.1%). Gram-positive cocci accounted for 31.6% of isolates, primarily coagulase-negative staphylococci (21%). Among 28 strains tested for resistance, 57% were multidrug-resistant, including 61% ESBL- or carbapenemase-producing Enterobacterales. The case-fatality rate was 36%. Conclusion: The incidence of healthcare-associated bloodstream infections in the neonatal unit of Dalal Jamm Hospital is high, with a predominance of multidrug-resistant Gram-negative bacteria. Strengthening infection prevention and control programs, rational antibiotic use, and continuous surveillance are urgently needed to reduce neonatal morbidity and mortality in resource-limited settings.
|
Published in
|
American Journal of Pediatrics (Volume 12, Issue 1)
|
|
DOI
|
10.11648/j.ajp.20261201.11
|
|
Page(s)
|
1-8 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Neonatal Sepsis, Healthcare-associated Infections, Bloodstream Infection, Antimicrobial Resistance,
Low-resource Countries, Senegal
1. Introduction
Bacteremia remains one of the leading causes of severe infection in neonates and constitutes a major public health concern worldwide. The incidence of neonatal bacteremia varies considerably across settings, ranging from 2 to 20 per 1,000 live births in high-income countries, but reaching 40 to 50 per 1,000 in low- and middle-income countries (LMICs)
| [1] | Thaver D, Zaidi AKM. Burden of neonatal infections in developing countries: a review of evidence from community-based studies. Pediatr Infect Dis J. 2009; 28(1 Suppl): S3–S9. https://doi.org/10.1097/inf.0b013e3181958755 |
| [2] | Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, et al. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Glob Health. 2018; 6(3): e300–e310. https://doi.org/10.1016/s2213-2600(18)30063-8 |
[1, 2]
. Mortality associated with neonatal bacteremia remains high, estimated between 20% and 50% in LMICs, with the highest rates observed among preterm and very low birth weight infants
| [3] | Okomo U, Akpalu ENK, le Doare K, et al. Aetiology of invasive bacterial infection and antimicrobial resistance in neonates in sub-Saharan Africa: a systematic review and meta-analysis. Lancet Infect Dis. 2019; 19(11): 1219–1234.
https://doi.org/10.1016/S1473-3099(19)30414-1 |
| [4] | Klingenberg C, Kornelisse RF, Buonocore G, et al. Culture-negative early-onset neonatal sepsis—At the crossroad between efficient sepsis care and antimicrobial stewardship. Pediatr Infect Dis J. 2018; 37(9): 950–955.
https://doi.org/10.3389/fped.2018.00285 |
[3, 4]
. The main identified risk factors include prematurity, low birth weight, mechanical ventilation, parenteral nutrition, prolonged use of intravenous catheters, and hospitalization in neonatal intensive care units
| [5] | Vergnano S, Sharland M, Kazembe P, et al. Neonatal sepsis: an international perspective. Arch Dis Child Fetal Neonatal Ed. 2011; 96(2): F115–F120.
https://doi.org/10.1136/adc.2002.022863 |
| [6] | Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011; 377(9761): 228–41.
https://doi.org/10.1016/s0140-6736(10)61458-4 |
[5, 6]
. Healthcare-associated infections (HAIs) represent a major public health challenge, particularly in developing countries where resources for infection prevention and control remain limited or absent
.
In neonates—a population particularly vulnerable due to immune immaturity—HAIs are responsible for substantial morbidity and mortality. They are defined as any infection occurring during or following medical management (diagnostic, therapeutic, palliative, preventive, or educational) of a newborn (0–28 days), which was neither present nor incubating at the time of admission. A delay of at least 48 hours after hospitalization is generally used as the diagnostic threshold.
The incidence of HAIs in neonatal units varies according to the level of care (routine care, special care nursery, neonatal intensive care unit) and the types of interventions provided. In Senegal, limited data are available regarding HAIs in neonatal settings. Therefore, this study was undertaken to determine the incidence and to describe the epidemiological and microbiological profiles of healthcare-associated bloodstream infections (HA-BSIs) within the neonatal unit of Dalal Jamm National Hospital in Dakar, Senegal.
2. Materials and Methods
2.1. Study Setting
This study was conducted in the neonatology unit of the pediatric department at the Dalal Jamm National Hospital Center in Guediawaye, Senegal. This facility is a tertiary-level public healthcare institution located in the suburbs of Dakar.
The neonatal unit functions as an intensive care unit, although endotracheal intubation is not performed. Most admitted newborns are inborn, originating from the hospital’s own maternity ward, which is adjacent to the neonatal unit. However, a proportion of patients are outborn, referred from other healthcare facilities in the region.
2.1.1. Study Design and Period
This was a retrospective observational cohort study conducted over a 10-month period, from October 2022 to July 2023.
2.1.2. Study Population
All newborns with at least one positive blood culture obtained more than 48 hours after admission to the neonatal unit were included in the study.
Newborns with bacteremia due to Staphylococcus epidermidis and those with documented maternal–fetal infectionswere excluded from the analysis.
2.2. Bacteriological Methods
Blood culture was collected in pediatric service where patients were admitted. Venous blood (3 mL for pediatric bottles) was collected into one specific culture media PEDS Plus) per children strictly adhering aseptic technique recommendations, as the volume collected is the main determinant of diagnostic performance. The automated BD Bactec system (BACTEC FX40) was used for incubation and monitoring at 37°C for up to 5 days. The instrument monitors CO₂ production to detect microbial growth. a negative result was reported if no growth was detected within 5 days. For positive blood cultures, a fresh wet mount was first examined under a microscope (40x objective). Subsequently, the sample was sub cultured onto blood agar plate and incubated at 37°C for 24-48 hours. Identification and antibiotic susceptibility were determined using the Vitek®2 automated system, in accordance with the recommendations of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) in force at the time of the study.
2.3. Data Collection and Analysis
Data were collected from medical records, hospital admission registers, and the bacteriology laboratory logbook. The following information was retrieved: source of admission, age at admission, gestational age, birth weight, sex, bacteriological findings, invasive procedures, and clinical outcome. Data were analyzed using R software, version 4.1.3.
Categorical variables were summarized as frequencies and percentages. The time to onset of healthcare-associated infection was described using the median and interquartile range (IQR: 25th–75th percentiles), as the distribution did not follow a normal pattern according to normality tests.
3. Results
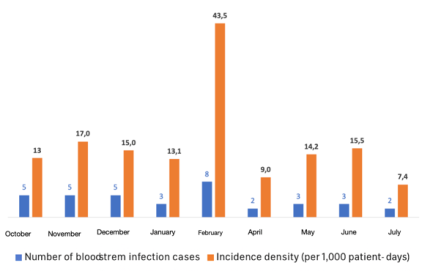
A total of 36 cases of HA-BSI were recorded among 288 neonates admitted, corresponding to a cumulative incidence of 12.5%. For a total of 2,315 hospitalization days, the incidence density was 15.5 cases per 1,000 patient-days. The incidence density varied by month (
Figure 1). It tripled in February, with a peak of eight recorded cases, corresponding to an incidence density of 43.5 cases per 1,000 patient-days. The absence of data for March 2023 was due to the temporary closure of the neonatal unit during that month.
Figure 1. Trend in the incidence density of healthcare-associated bloodstream infections from October 2022 to February 2023, Neonatology Unit, Dalal Jamm National Hospital (Senegal).
Nearly two-thirds (61%) of neonates were admitted on day 0 of life, and the majority were inborn (69%). More than half (53%) had a low birth weight (<2,500 g) and were preterm (
Table 1). The median time to onset of HA-BSI was 6 days (IQR: 2–13 days). Congenital malformations were observed in 39% (n=14) of cases (including omphalocele, volvulus, congenital heart disease, and intestinal atresia), among which five neonates underwent surgical intervention. Seven (19%) had a central venous catheter (CVC) in place.
Table 1. Epidemiological, clinical, and outcome characteristics of healthcare-associated bloodstream infection cases; Neonatology Unit, Dalal Jamm National Hospital (Senegal) (n = 36).
Variable | Number | Percentage (%) |
Age at admission |
Day 0 (birth day) | 22 | 61 |
Day 1–7 | 11 | 31 |
7 days | 3 | 8 |
Origin of admission |
Hospital maternity (inborn) | 25 | 69 |
Referred from other facilities (outborn) | 11 | 31 |
Sex | | |
Female | 20 | 56 |
Male | 16 | 44 |
Birth weight (grams) |
2500 | 19 | 53 |
≥ 2500 | 17 | 47 |
Prematurity (< 37 weeks of gestation) |
Yes | 19 | 53 |
No | 17 | 47 |
Outcome | | |
Death | 13 | 36 |
Favorable outcome | 23 | 64 |
A total of 38 bacterial isolates were recovered. Gram-negative bacilli accounted for 65.8% of isolates, predominantly Enterobacterales (47.3%), mainly
Enterobacter, Klebsiella, and
Escherichia species (
Table 2). Among Gram-positive cocci (31.6%),
Staphylococcus species were predominant.
Staphylococcus haemolyticus and other coagulase-negative staphylococci were identified in 21% of cases.
Table 2. Distribution of cases according to bacteriological findings; Neonatology Unit, Dalal Jamm National Hospital (Senegal) (n = 38).
Gram/Genus | Species | Number | Percentage (%) |
Gram-positive (n = 13) | | | 34.2 |
Staphylococcus (n = 12) | | | |
| Coagulase-negative staphylococci | 5 | 13.1 |
| Staphylococcus aureus | 4 | 10.5 |
| Staphylococcus haemolyticus | 3 | 7.9 |
Enterococcus (n = 1) | Enterococcus faecalis | 1 | 2.6 |
Gram-negative (n = 25) | | | 65, 8 |
Enterobacterales | | | |
Enterobacter | Enterobacter cloacae | 7 | 18.4 |
Klebsiella | Klebsiella pneumoniae | 6 | 15.8 |
Escherichia | Escherichia coli | 5 | 13.1 |
Non-fermenting Gram-negative bacilli | | | |
Acinetobacter | Acinetobacter baumannii | 3 | 7.9 |
| Acinetobacter spp. | 2 | 5.3 |
Pseudomonas | Pseudomonas aeruginosa | 1 | 2.6 |
| Pseudomonas fluorescens | 1 | 2.6 |
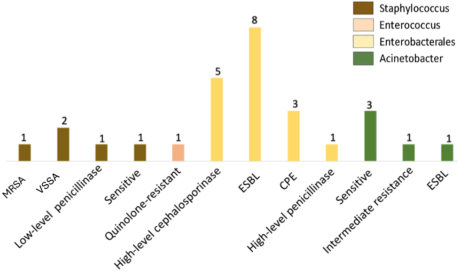
Antimicrobial resistance profiles were available for 28 isolates. The prevalence of multidrug-resistant (MDR) bacteria was 57% (
Figure 2). Among the 18 Enterobacterales isolates, 61% were extended-spectrum β-lactamase (ESBL) or carbapenemase-producing Enterobacterales (CPE), comprising 8 ESBL-producing and 3 CPE strains. Additionally, One methicillin-resistant
Staphylococcus aureus (MRSA) isolate was identified and two Vancomycin-non-susceptible S. aureus. The in-hospital case fatality rate was 36% (13/36).
Figure 2. Antimicrobial resistance phenotypes of bacterial isolates. Study on healthcare-associated bloodstream infections in the Neonatology Unit, Dalal Jamm National Hospital (Senegal).
4. Discussion
This study provided a situational analysis of HA-BSIs within the neonatal unit of Dalal Jamm Hospital in Senegal. In our series, the cumulative incidence was 12.5%, with an incidence density of 15.5 cases per 1,000 patient-days. These findings are consistent with those reported in other resource-limited settings, where HA-BSIs remain a major concern in neonatal care.
Indeed, in Cameroon, a longitudinal study conducted at the Yaounde University Hospital Center reported an incidence density of healthcare-associated infections of 17.44 cases per 1,000 hospitalization-days in the neonatal unit
| [9] | Nouetchognou JS, Ateudjieu J, Jemea B, et al. Surveillance of nosocomial infections in the Yaounde University Teaching Hospital, Cameroon. BMC Res Notes. 2016; 9(1): 505.
https://doi.org/10.1186/s13104-016-2310-1 |
[9]
. In Brazil, a study published by the National Healthcare Safety Network (NHSN) reported a sepsis incidence rate of 17.9 cases per 1,000 patient-days, of which 60% were bloodstream infections, accounting for 65.8% of all healthcare-associated infections recorded
| [10] | Porto JP, Mantese OC, Arantes A, Freitas C, Gontijo Filho PP, Ribas RM. Nosocomial infections in a pediatric intensive care unit of a developing country: NHSN surveillance. Rev Soc Bras Med Trop. 2012; 45(4): 475-9.
https://doi.org/10.1590/s0037-86822012005000003 |
[10]
.
At the Diamniadio Children’s Hospital in Senegal, the overall incidence of healthcare-associated infections in the neonatal unit was 18.9%, slightly higher than that observed in our study. However, infection was microbiologically confirmed in 68% of cases. Bacteremia and fungemia were the most common types of infection, accounting for 44% of all cases
| [11] | Sarr R. Epidemiological, clinical, paraclinical and evolutionary aspects of healthcare-associated infections in the neonatology department of Diamniadio Children's Hospital: A two-year retrospective study (2020-2021) [Medical Thesis]. Thies (Senegal): Iba Der Thiam University; 2022. |
[11]
.
Among preterm infants, the incidence of healthcare-associated infections was higher, reaching 41.8%
| [12] | Sy A. Morbidity and mortality of healthcare-associated infections in premature infants at the neonatology department of Diamniadio Children's Hospital: A one-year retrospective study (2018) [Specialized Studies Diploma in Pediatrics dissertation]. Dakar (Senegal): Cheikh Anta Diop University; 2019. [cited 2023 Mar 1]. Available from:
https://bibnum.ucad.sn/viewer.php?c=mmoires&d=memm_2019_0666 |
[12]
. In high-income countries, however, a lower incidence is generally reported. In the United States, Prochaska et al. Found an incidence density of 1.1 cases per 1,000 patient-days
.
In Germany, the series reported by Geffers et al. found an incidence density of 6.5 cases per 1,000 patient-days, with 8.5 per 1,000 among very low birth weight infants and 4.0 per 1,000 among those weighing more than 1,500 g
| [14] | Geffers C, Baerwolff S, Schwab F, et al. Incidence of healthcare-associated infections in high-risk neonates: results from the German surveillance system for very-low-birthweight infants. J Hosp Infect. 2008; 68(3): 214-21.
https://doi.org/10.1016/j.jhin.2008.01.016 |
[14]
.
These disparities may be explained by the limited infrastructure and resources in LMICs. Neonatal units often face bed overcrowding, a low nurse-to-infant ratio, and a lack of essential protective measures such as access to running water, alcohol-based hand rubs, and personal protective equipment. In addition, infection prevention and control (IPC) programs are frequently absent or only partially implemented.
In high-income countries, the incidence rates of bloodstream infections are most often expressed in relation to the number of central venous catheter (CVC) days, since catheterization increases the risk of sepsis three- to fourfold, and this risk rises with the duration of catheter use
.
In our study, 19% of neonates had a CVC inserted. In France, in 2019, the incidence of umbilical venous catheter (UVC)-related bloodstream infections was 2.3 cases per 100 UVCs, with an incidence density of 5 cases per 1,000 UVC-days
.
In the Netherlands, a surveillance study conducted in a neonatal unit from 2012 to 2020 recorded 310 episodes of HA-BSIs among preterm infants. One-third of these infections were associated with CVCs. The incidence of catheter-related bloodstream infections (CRBSIs) ranged from 8.83 to 25.3 cases per 1,000 CVC-days, with no significant variation over the study period
| [18] | Jansen SJ, van der Hoeven A, van den Akker T, et al. A longitudinal analysis of nosocomial bloodstream infections among preterm neonates. Eur J Clin Microbiol Infect Dis. 2022; 41(11): 1327-1336.
https://doi.org/10.1007/s10096-022-04502-8 |
[18]
. In Turkey, Kulali et al. reported an incidence of 12.4 UVC-related bloodstream infections per 1,000 UVC-days, which was markedly reduced to 3.9 per 1,000 UVC-days following the implementation of bundles
| [19] | Kulali F, Çalkavur Ş, Oruç Y, et al. Impact of central line bundle for prevention of umbilical catheter-related bloodstream infections in a neonatal intensive care unit: A pre-post intervention study. Am J Infect Control. 2019; 47(4): 387-390. https://doi.org/10.1016/j.ajic.2018.10.002 |
[19]
. In our setting, as in most LMICs, the use of CVCs and other invasive devices often occurs without single-use materials and in the absence of standardized insertion and maintenance protocols. Moreover, the removal of such devices is frequently delayed. All these factors contribute to an increased risk of infection.
Apart from CVCs, bacterial translocation from the gastrointestinal tract and systemic dissemination from an initial localized infectious focus are other key mechanisms explaining the occurrence of HA-BSIs in neonatal units
.
It has been demonstrated that gestational age and low birth weight are significant risk factors for the occurrence of HAIs
.
In our series, preterm infants and low birth weight newborns represented the majority of cases (53%). The clinical condition of these infants often necessitates the use of invasive procedures (such as intubation or central venous catheterization), prolonged hospitalization, and broad-spectrum antibiotic therapy, all of which predispose to the development of HAIs.
According to the World Health Organization (WHO), there were an estimated 2.8 million neonatal deaths worldwide in 2015, of which 47.6% were attributable to neonatal infections
. HAIs in neonatal units are responsible for a high case fatality rate, ranging from 12% to 52%
| [22] | Shefali O, Joy E, Daniel R, et al. Neonatal causes of death estimates for the early an late neonatale periods for 194 countries. Bull World Health Organ. 2015; 93(1): 19–28.
https://doi.org/10.2471/blt.14.139790 |
[22]
. In our series, one-third (36%) of neonates died. A similar rate (37%) was reported at the Diamniadio Children’s Hospital in Senegal
| [11] | Sarr R. Epidemiological, clinical, paraclinical and evolutionary aspects of healthcare-associated infections in the neonatology department of Diamniadio Children's Hospital: A two-year retrospective study (2020-2021) [Medical Thesis]. Thies (Senegal): Iba Der Thiam University; 2022. |
[11]
.
From a microbiological perspective, five cases of infection due to Enterobacter cloacae were identified, strongly suggesting the occurrence of a localized outbreak during that period. In our study, Gram-negative bacilli were the most frequently isolated pathogens in blood cultures (65.8%), predominantly Enterobacter cloacae (18.4%), Klebsiella pneumoniae (15.8%), and Escherichia coli (13.1%). Gram-positive cocci accounted for approximately one-third of cases (31.6%).
Gram-positive cocci accounted for one-third of the cases (31.6%). Coagulase-negative staphylococci (CoNS) were isolated in 21% of cases, followed by
Staphylococcus aureus in 10.5%. These findings are consistent with those reported in Senegal and in other LMICs, showing a predominance of Gram-negative bacilli. In the neonatal unit of the Diamniadio Hospital Center in Senegal, the three most frequently isolated pathogens in blood cultures among neonates hospitalized for more than two days were Klebsiella pneumoniae (33%), Enterobacter spp. (24%), and Escherichia coli (8.6%)
| [23] | Makiese Khoto D. Bacteriological profile of neonatal infections in the neonatology department of the Diamniadio National Children's Hospital (from January 2015 to December 2016) [Specialized Studies Diploma in Pediatrics dissertation]. Dakar (Senegal): Cheikh Anta Diop University; 2018. [cited 2023 Mar 1]. Available from:
http://bibnum.ucad.sn/viewer.php?c=mmoires&d=memm%5f2019%5f0119 |
[23]
.
In the multicenter prospective “BIRDY” study, Klebsiella spp. (24.4%), Escherichia coli (22.2%), and Staphylococcusspp. (24.4%) were the main bacterial pathogens isolated in cases of severe neonatal infections
| [11] | Sarr R. Epidemiological, clinical, paraclinical and evolutionary aspects of healthcare-associated infections in the neonatology department of Diamniadio Children's Hospital: A two-year retrospective study (2020-2021) [Medical Thesis]. Thies (Senegal): Iba Der Thiam University; 2022. |
[11]
.
In the meta-analysis published by Zelellw DA et al., Klebsiella pneumoniae (26.36%) was identified as the most frequently isolated pathogen in cases of neonatal infections in developing countries
| [24] | Zelellw DA, Dessie G, Mengesha EW, et al. A Systemic Review and Meta-analysis of the Leading Pathogens Causing Neonatal Sepsis in Developing Countries. Biomed Res Int. 2021; 2021: 6626983. https://doi.org/10.1155/2021/6626983 |
[24]
. The bacterial ecology in high-income countries, however, is markedly different—particularly in catheter-related bloodstream infections, where CoNS are predominant (28–70%), followed by Staphylococcus aureus (7.5–19%)
.
The management of HAIs is particularly challenging because the isolated bacteria are most often MDR. In our series, analysis of resistance phenotypes showed that 57% of isolates were MDR. Among the 18 Enterobacterales strains, 61% were either ESBL or CPE. In a hospital-based study from South Africa, 80% of Klebsiella pneumoniae isolates were ESBL producers, and 66.7% of staphylococcal strains were methicillin-resistant
| [26] | Gezmu AM, Bulabula ANH, Dramowski A, et al. Laboratory-confirmed bloodstream infections in two large neonatal units in sub-Saharan Africa. Int J Infect Dis. 2021; 103: 201-207. https://doi.org/10.1016/j.ijid.2020.11.169 |
[26]
.
In LMICs, the emergence of MDR bacteria is linked to several factors, including inappropriate antibiotic prescribing, self-medication, illegal over-the-counter sales of antibiotics, and insufficient regulation of drug quality control, among others
. The therapeutic arsenal available for the management of MDR HAIs remains limited in Senegal. Indeed, several key antibiotics—such as ertapenem, ceftazidime, linezolid, piperacillin–tazobactam, and dalbavancin—are not readily available. This limitation results in high patient mortality and increases the risk of cross-transmission to other patients if appropriate IPC measures are not strictly observed.
5. Conclusions
The incidence of HA-BSIs in neonatal units remains relatively high, confirming the major public health challenge posed by this condition. In resource-limited countries, the prevention of infectious risk in neonatology represents the most effective strategy to reduce the morbidity and mortality associated with HA-BSIs. Prevention efforts should focus on the implementation of targeted interventions, including the adequate design and organization of neonatal care units, strengthening of healthcare staffing, regular assessment of clinical practices, training of healthcare workers in infection prevention and hygiene measures, continuous reinforcement of adherence to these practices, and the prospective surveillance of healthcare-associated infections in neonatal settings.
Abbreviations
LMICs | Low- and Middle-Income Countries |
HAIs | Healthcare-Associated Infections |
HA-BSIs | Healthcare-Associated Bloodstream Infections |
MDR | Multidrug-Resistant |
ESBL | Extended-Spectrum β-Lactamase |
CPE | Carbapenemase-Producing Enterobacterales |
VSSA | Vancomycin-Non Susceptible Staphylococcus Aureus |
MRSA | Methicillin-resistant Staphylococcus Aureus |
NHSN | National Healthcare Safety Network |
IPC | Infection Prevention and Control |
MICs | Minimum Inhibitory Concentrations |
CVC | Central Venous Catheter |
UVC | Umbilical Venous Catheter |
CRBSIs | Catheter-related Bloodstream Infections |
WHO | World Health Organization |
CoNS | Coagulase-Negative Staphylococci |
Acknowledgments
We deeply thank nurses in pediatric for blood collection and the bacteriology laboratory staff for performing tests related to blood culture during the study.
Author Contributions
Ndeye Fatou Sow: Writing – original draft.
Louise Fortes: Writing – review & editing.
Awa Ba: Investigation, Writing – review & editing.
Abou Ba: Supervision, Validation.
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Thaver D, Zaidi AKM. Burden of neonatal infections in developing countries: a review of evidence from community-based studies. Pediatr Infect Dis J. 2009; 28(1 Suppl): S3–S9.
https://doi.org/10.1097/inf.0b013e3181958755
|
| [2] |
Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, et al. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Glob Health. 2018; 6(3): e300–e310.
https://doi.org/10.1016/s2213-2600(18)30063-8
|
| [3] |
Okomo U, Akpalu ENK, le Doare K, et al. Aetiology of invasive bacterial infection and antimicrobial resistance in neonates in sub-Saharan Africa: a systematic review and meta-analysis. Lancet Infect Dis. 2019; 19(11): 1219–1234.
https://doi.org/10.1016/S1473-3099(19)30414-1
|
| [4] |
Klingenberg C, Kornelisse RF, Buonocore G, et al. Culture-negative early-onset neonatal sepsis—At the crossroad between efficient sepsis care and antimicrobial stewardship. Pediatr Infect Dis J. 2018; 37(9): 950–955.
https://doi.org/10.3389/fped.2018.00285
|
| [5] |
Vergnano S, Sharland M, Kazembe P, et al. Neonatal sepsis: an international perspective. Arch Dis Child Fetal Neonatal Ed. 2011; 96(2): F115–F120.
https://doi.org/10.1136/adc.2002.022863
|
| [6] |
Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011; 377(9761): 228–41.
https://doi.org/10.1016/s0140-6736(10)61458-4
|
| [7] |
Zaidi AK, Huskins WC, Thaver D, et al. Hospital-acquired neonatal infections in developing countries. Lancet. 2005; 365: 1175–88.
https://doi.org/10.1016/s0140-6736(05)71881-x
|
| [8] |
Hadfield BR, Cantey JB. Neonatal Bloostream infections. Curr Opin Infect Dis. 2021; 34(5): 533-537.
https://doi.org/10.1097/qco.0000000000000764
|
| [9] |
Nouetchognou JS, Ateudjieu J, Jemea B, et al. Surveillance of nosocomial infections in the Yaounde University Teaching Hospital, Cameroon. BMC Res Notes. 2016; 9(1): 505.
https://doi.org/10.1186/s13104-016-2310-1
|
| [10] |
Porto JP, Mantese OC, Arantes A, Freitas C, Gontijo Filho PP, Ribas RM. Nosocomial infections in a pediatric intensive care unit of a developing country: NHSN surveillance. Rev Soc Bras Med Trop. 2012; 45(4): 475-9.
https://doi.org/10.1590/s0037-86822012005000003
|
| [11] |
Sarr R. Epidemiological, clinical, paraclinical and evolutionary aspects of healthcare-associated infections in the neonatology department of Diamniadio Children's Hospital: A two-year retrospective study (2020-2021) [Medical Thesis]. Thies (Senegal): Iba Der Thiam University; 2022.
|
| [12] |
Sy A. Morbidity and mortality of healthcare-associated infections in premature infants at the neonatology department of Diamniadio Children's Hospital: A one-year retrospective study (2018) [Specialized Studies Diploma in Pediatrics dissertation]. Dakar (Senegal): Cheikh Anta Diop University; 2019. [cited 2023 Mar 1]. Available from:
https://bibnum.ucad.sn/viewer.php?c=mmoires&d=memm_2019_0666
|
| [13] |
Prochaska EC, Xiao S, Colantuoni E, et al. CDC Prevention Epicenters Program. Hospital-Onset Bacteremia Among Neonatal Intensive Care Unit Patients. JAMA Pediatr. 2024; 178(8): 792-799.
https://doi.org/10.1001/jamapediatrics.2024.1840
|
| [14] |
Geffers C, Baerwolff S, Schwab F, et al. Incidence of healthcare-associated infections in high-risk neonates: results from the German surveillance system for very-low-birthweight infants. J Hosp Infect. 2008; 68(3): 214-21.
https://doi.org/10.1016/j.jhin.2008.01.016
|
| [15] |
Lachassinne E, Letamendia-Richard E, et al. Épidémiologie des infections nosocomiales en néonatalogie. Arch Pediatr. 2004; 11(3): 229-33.
https://doi.org/10.1016/j.arcped.2003.10.016
|
| [16] |
Sanderson E, Yeo KT, Wang AY, et al. Dwell time and risk of central-line-associated bloodstream infection in neonates. Hosp Infect. 2017; 97(3): 267-274.
https://doi.org/10.1016/j.jhin.2017.06.023
|
| [17] |
Néocat Surveillance Network; CPias Ile-de-France. Surveillance of central venous catheters in neonatology - Néocat Network: 2019 Results [Internet]. Paris: CPias Ile-de-France; 2019 [cited 2023 Mar 24]. Available from:
https://www.cpias-ile-defrance.fr/surveillance/neocat/2019/Neocat2019_Rapport.pdf
|
| [18] |
Jansen SJ, van der Hoeven A, van den Akker T, et al. A longitudinal analysis of nosocomial bloodstream infections among preterm neonates. Eur J Clin Microbiol Infect Dis. 2022; 41(11): 1327-1336.
https://doi.org/10.1007/s10096-022-04502-8
|
| [19] |
Kulali F, Çalkavur Ş, Oruç Y, et al. Impact of central line bundle for prevention of umbilical catheter-related bloodstream infections in a neonatal intensive care unit: A pre-post intervention study. Am J Infect Control. 2019; 47(4): 387-390.
https://doi.org/10.1016/j.ajic.2018.10.002
|
| [20] |
Doit C, Biran V, Aujar Y. Infections nosocomiales en néonatologie. In: Infections néonatales. Paris: Elsevier Masson; 2015. p. 91–106.
https://doi.org/10.1016/B978-2-294-74135-7.00009-7
|
| [21] |
Lima CSSDC, Rocha HAL, Araújo DABS, et al. Determinants of late neonatal nosocomial infection: a case-control study in Ceará. Rev Saude Publica. 2022; 56: 40.
https://doi.org/10.11606/s1518-8787.2022056003291
|
| [22] |
Shefali O, Joy E, Daniel R, et al. Neonatal causes of death estimates for the early an late neonatale periods for 194 countries. Bull World Health Organ. 2015; 93(1): 19–28.
https://doi.org/10.2471/blt.14.139790
|
| [23] |
Makiese Khoto D. Bacteriological profile of neonatal infections in the neonatology department of the Diamniadio National Children's Hospital (from January 2015 to December 2016) [Specialized Studies Diploma in Pediatrics dissertation]. Dakar (Senegal): Cheikh Anta Diop University; 2018. [cited 2023 Mar 1]. Available from:
http://bibnum.ucad.sn/viewer.php?c=mmoires&d=memm%5f2019%5f0119
|
| [24] |
Zelellw DA, Dessie G, Mengesha EW, et al. A Systemic Review and Meta-analysis of the Leading Pathogens Causing Neonatal Sepsis in Developing Countries. Biomed Res Int. 2021; 2021: 6626983.
https://doi.org/10.1155/2021/6626983
|
| [25] |
Gowda H, Norton R, White A, et al. Late-onset Neonatal Sepsis-A 10-year Review from North Queensland, Australia. Pediatr Infect Dis J. 2017; 36(9): 883-888.
https://doi.org/10.1097/inf.0000000000001568
|
| [26] |
Gezmu AM, Bulabula ANH, Dramowski A, et al. Laboratory-confirmed bloodstream infections in two large neonatal units in sub-Saharan Africa. Int J Infect Dis. 2021; 103: 201-207.
https://doi.org/10.1016/j.ijid.2020.11.169
|
| [27] |
Da L, Somé D, Yehouenou C, et al. Overview of antibiotic resistance in sub-Saharan Africa. Med Mal Infect. 2023; 2(1): 3-12.
https://doi.org/10.1016/j.mmifmc.2023.01.003
|
| [28] |
WHO Regional office for Africa. Antimicrobial resistance in the African Region: Issues, challenges and actions proposed. Geneva: WHO; 2017.
https://www.afro.who.int/sites/default/files/2017-06/amr-paper-march-2013-jbn-and-all.pdf?
|
Cite This Article
-
APA Style
Sow, N. F., Fortes, L., Diallo, A. B., Ba, A. (2026). Healthcare-associated Bloodstream Infections in the Neonatal Unit of Dalal Jamm National Hospital, Senegal: Epidemiological and Microbiological Characteristics. American Journal of Pediatrics, 12(1), 1-8. https://doi.org/10.11648/j.ajp.20261201.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Sow, N. F.; Fortes, L.; Diallo, A. B.; Ba, A. Healthcare-associated Bloodstream Infections in the Neonatal Unit of Dalal Jamm National Hospital, Senegal: Epidemiological and Microbiological Characteristics. Am. J. Pediatr. 2026, 12(1), 1-8. doi: 10.11648/j.ajp.20261201.11
Copy
|
Download
AMA Style
Sow NF, Fortes L, Diallo AB, Ba A. Healthcare-associated Bloodstream Infections in the Neonatal Unit of Dalal Jamm National Hospital, Senegal: Epidemiological and Microbiological Characteristics. Am J Pediatr. 2026;12(1):1-8. doi: 10.11648/j.ajp.20261201.11
Copy
|
Download
-
@article{10.11648/j.ajp.20261201.11,
author = {Ndeye Fatou Sow and Louise Fortes and Awa Ba Diallo and Abou Ba},
title = {Healthcare-associated Bloodstream Infections in the Neonatal Unit of Dalal Jamm National Hospital, Senegal: Epidemiological and Microbiological Characteristics},
journal = {American Journal of Pediatrics},
volume = {12},
number = {1},
pages = {1-8},
doi = {10.11648/j.ajp.20261201.11},
url = {https://doi.org/10.11648/j.ajp.20261201.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261201.11},
abstract = {Introduction: Healthcare-associated bloodstream infections (HA-BSIs) represent a major cause of morbidity and mortality in neonatal intensive care units, particularly in low- and middle-income countries (LMICs). In Senegal, few data exist regarding the incidence, bacterial spectrum, and antimicrobial resistance patterns of HA-BSIs in neonates. This study aimed to describe the epidemiological and microbiological profile of healthcare-associated bloodstream infections in the neonatal unit of Dalal Jamm National Hospital in Senegal. Methods: We conducted a retrospective longitudinal study from October 2022 to July 2023 in the neonatal unit of Dalal Jamm National Hospital. All neonates with at least one positive blood culture obtained ≥48 hours after admission were included. Data were extracted from medical records and bacteriology registers and analyzed using R software v4.1.3. Categorical variables were expressed as frequencies, and the time to infection onset was described by the median and interquartile range. Results: Among 288 admitted neonates, 36 cases of HA-BSIs were recorded, yielding a cumulative incidence of 12.5% and an incidence density of 15.5 cases per 1 000 patient-days. The median time to infection was 6 days [IQR 2–13]. Prematurity and low birth weight (< 2 500 g) were observed in 53% of cases. A total of 38 pathogens were isolated, predominantly Gram-negative bacilli (65.8%), mainly Enterobacter cloacae (18.4%), Klebsiella pneumoniae (15.8%), and Escherichia coli (13.1%). Gram-positive cocci accounted for 31.6% of isolates, primarily coagulase-negative staphylococci (21%). Among 28 strains tested for resistance, 57% were multidrug-resistant, including 61% ESBL- or carbapenemase-producing Enterobacterales. The case-fatality rate was 36%. Conclusion: The incidence of healthcare-associated bloodstream infections in the neonatal unit of Dalal Jamm Hospital is high, with a predominance of multidrug-resistant Gram-negative bacteria. Strengthening infection prevention and control programs, rational antibiotic use, and continuous surveillance are urgently needed to reduce neonatal morbidity and mortality in resource-limited settings.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Healthcare-associated Bloodstream Infections in the Neonatal Unit of Dalal Jamm National Hospital, Senegal: Epidemiological and Microbiological Characteristics
AU - Ndeye Fatou Sow
AU - Louise Fortes
AU - Awa Ba Diallo
AU - Abou Ba
Y1 - 2026/01/23
PY - 2026
N1 - https://doi.org/10.11648/j.ajp.20261201.11
DO - 10.11648/j.ajp.20261201.11
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 1
EP - 8
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20261201.11
AB - Introduction: Healthcare-associated bloodstream infections (HA-BSIs) represent a major cause of morbidity and mortality in neonatal intensive care units, particularly in low- and middle-income countries (LMICs). In Senegal, few data exist regarding the incidence, bacterial spectrum, and antimicrobial resistance patterns of HA-BSIs in neonates. This study aimed to describe the epidemiological and microbiological profile of healthcare-associated bloodstream infections in the neonatal unit of Dalal Jamm National Hospital in Senegal. Methods: We conducted a retrospective longitudinal study from October 2022 to July 2023 in the neonatal unit of Dalal Jamm National Hospital. All neonates with at least one positive blood culture obtained ≥48 hours after admission were included. Data were extracted from medical records and bacteriology registers and analyzed using R software v4.1.3. Categorical variables were expressed as frequencies, and the time to infection onset was described by the median and interquartile range. Results: Among 288 admitted neonates, 36 cases of HA-BSIs were recorded, yielding a cumulative incidence of 12.5% and an incidence density of 15.5 cases per 1 000 patient-days. The median time to infection was 6 days [IQR 2–13]. Prematurity and low birth weight (< 2 500 g) were observed in 53% of cases. A total of 38 pathogens were isolated, predominantly Gram-negative bacilli (65.8%), mainly Enterobacter cloacae (18.4%), Klebsiella pneumoniae (15.8%), and Escherichia coli (13.1%). Gram-positive cocci accounted for 31.6% of isolates, primarily coagulase-negative staphylococci (21%). Among 28 strains tested for resistance, 57% were multidrug-resistant, including 61% ESBL- or carbapenemase-producing Enterobacterales. The case-fatality rate was 36%. Conclusion: The incidence of healthcare-associated bloodstream infections in the neonatal unit of Dalal Jamm Hospital is high, with a predominance of multidrug-resistant Gram-negative bacteria. Strengthening infection prevention and control programs, rational antibiotic use, and continuous surveillance are urgently needed to reduce neonatal morbidity and mortality in resource-limited settings.
VL - 12
IS - 1
ER -
Copy
|
Download