Abstract
Introduction: Type 1 diabetes mellitus (T1DM) is a chronic disease that predominantly affects children and adolescents. Its management requires strict adherence to medical recommendations in order to prevent severe acute and chronic complications. However, during adolescence, therapeutic adherence often becomes challenging due to physical, psychological, and social factors specific to this stage of life. The objective of this study was to determine the prevalence of poor therapeutic adherence among adolescents with T1DM followed in pediatric departments of the University Hospital Center of Dakar and to identify the factors associated with non-adherence. Methods: This was a prospective, descriptive, analytical, and multicenter study conducted over a three-month period (March–April–May 2023) in the pediatric departments of Abass Ndao Hospital Center and Albert Royer National Children’s Hospital in Dakar, Senegal. All patients aged 10 to 18 years with a diagnosis of T1DM for at least three months who attended outpatient consultations during the study period were included. Data were collected at the end of consultations using a pre-established questionnaire. Written informed consent was obtained from all participants and their caregivers. Therapeutic adherence to insulin was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8). Results: A total of 106 adolescents were included among 219 children who attended consultations during the study period. The sex ratio was 0.66, and the mean age was 14.61 years. According to the Morisky score, low adherence to insulin therapy was observed in 18.87% of patients, while good adherence was found in 27.36%. Overall, the prevalence of poor therapeutic adherence was 61.32%. Several factors were significantly associated with adherence. Full parental supervision was associated with better adherence compared to minimal parental involvement (p = 0.003). A perceived loss of freedom related to treatment and the presence of treatment-related side effects were significantly associated with poor adherence (p = 0.029 and p = 0.003, respectively). Poor adherence was also associated with diabetes diagnosis disclosure by a general practitioner rather than a pediatrician (p = 0.03). Furthermore, poor therapeutic adherence was significantly correlated with poor glycemic control (p = 0.03). Conclusion: This study highlights the importance of considering adolescent-specific factors in the management of type 1 diabetes. Improved understanding of these determinants may contribute to more effective care strategies and better prevention of complications among adolescents living with T1DM.
|
Published in
|
American Journal of Pediatrics (Volume 12, Issue 1)
|
|
DOI
|
10.11648/j.ajp.20261201.12
|
|
Page(s)
|
9-13 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Type 1 Diabetes Mellitus, Therapeutic Adherence, Adolescents
1. Introduction
Type 1 diabetes (T1D) is considered one of the most common chronic diseases among children and adolescents
. It results from an absolute insulin deficiency caused by autoimmune destruction of pancreatic β-cells within the islets of Langerhans
| [2] | National College of University Pediatricians; National College of Hospital and University Pediatric Surgery. Pediatrics. 8th ed. Issy-les-Moulineaux, France: Elsevier Masson; 2021. |
[2]
. In 2025, the International Diabetes Federation (IDF) estimated that 1.9 million children and adolescents under the age of 20 were living with T1DM worldwide, with a steadily increasing incidence, particularly in Africa
| [3] | Ward ZJ, Yeh JM, Reddy CL, et al. Global estimates of incidence of type 1 diabetes in children and adolescents aged 0-19 years: a simulation-based analysis. Lancet Diabetes Endocrinol. 2022; 10(12): 848-858. |
| [4] | International Diabetes Federation. IDF Diabetes Atlas. 11th ed. Brussels, Belgium: International Diabetes Federation; 2025. |
[3, 4]
. In Senegal, the prevalence of T1DM was estimated at 1.451‰ in 2021
| [5] | Magliano DJ, Boyko EJ. IDF Diabetes Atlas. 10th ed. Brussels, Belgium: International Diabetes Federation; 2021. |
[5]
. T1DM is associated with severe complications, including diabetic ketoacidosis as the main acute complication and a frequent cause of mortality, as well as chronic complications such as neuropathy, nephropathy, and retinopathy
| [2] | National College of University Pediatricians; National College of Hospital and University Pediatric Surgery. Pediatrics. 8th ed. Issy-les-Moulineaux, France: Elsevier Masson; 2021. |
[2]
. These complications are often related to poor glycemic control
| [6] | Brink SJ; International Society for Pediatric and Adolescent Diabetes. Diabetes in Childhood and Adolescence. 2nd ed. Bagsværd, Denmark: Novo Nordisk; 2013. |
[6]
. Therapeutic adherence, defined as “the extent to which a patient’s behavior corresponds with medical recommendations”
| [7] | Desbrus-Qochih A, Cathébras P. Adherence or compliance? Rethinking therapeutic adherence. Medecine & Longévité. 2012; 4(3-4): 111-122. |
[7]
, is therefore essential to reduce the risk of such complications. However, adherence tends to decline significantly during adolescence due to psychological and social factors specific to this developmental period
| [8] | Baron S, Caquard M, Caldagues E, et al. Therapeutic adherence in childhood and adolescent diabetes. Arch Pediatr. 2017; 24(2): 94-102. |
[8]
. In this context, we conducted the present study to determine the prevalence of poor therapeutic adherence among adolescents with T1DM followed at the University Hospital Center of Dakar, and to identify the factors associated with non-adherence, with the aim of improving the overall management of this population.
2. Materials and Methods
This was a prospective, descriptive, analytical, and multicenter study conducted over a three-month period (March–April–May 2023) in the pediatric departments of Abass Ndao Hospital Center and Albert Royer National Children’s Hospital in Dakar, Senegal.
2.1. Study Population
All patients aged 10 to 18 years with a diagnosis of type 1 diabetes for at least three months, followed in one of the participating centers, who attended outpatient consultations during the study period and who provided assent along with informed consent from their caregiver, were included in the study.
2.2. Data Collection
The variables studied included:
1) Sociodemographic data: sex, age, geographical origin, and socioeconomic status of parents or caregivers
2) Clinical data: family history of diabetes, circumstances of diagnosis, perception of the disease, and level of glycemic control
3) Therapeutic data: health care system-related factors and their perception, treatment-related factors and their perception, and therapeutic adherence
4) Data were collected at the end of outpatient consultations using a standardized pre-designed questionnaire.
5) Assessment of Therapeutic Adherence: Therapeutic adherence to insulin treatment was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8)
| [9] | Korb-Savoldelli V, Gillaizeau F, Pouchot J, et al. Validation of a French version of the 8-item Morisky Medication Adherence Scale in hypertensive patients. J Clin Hypertens. 2012; 14(7): 429-434. |
| [10] | Plakas S, Mastrogiannis D, Mantzorou M, et al. Validation of the Morisky Medication Adherence Scale (MMAS-8) in chronic ambulatory patients. Open J Nurs. 2016; 6(3): 158-169. |
[9, 10]
. In this study, poor adherence was defined by the presence of one or more of the following criteria:
a) A Morisky score indicating low adherence
b) Omission or skipping of insulin doses (affirmative response to the dichotomous question)
c) Poor attendance at follow-up visits (more than one missed consultation)
Any patient who failed to meet one or more of these criteria was considered non-adherent.
2.2. Statistical Analysis
Data entry and analysis were performed using Epi Info version 7.2.2.6 and Microsoft Excel 2019. Quantitative variables were expressed as means, standard deviations, medians, and ranges, while qualitative variables were presented as frequencies and percentages. Comparisons between qualitative variables were performed using the chi-square test. A p-value < 0.05 was considered statistically significant.
3. Results
During the study period, a total of 219 pediatric consultations were recorded in the participating centers. Among these, 106 adolescents met the inclusion criteria and were included in the analysis.
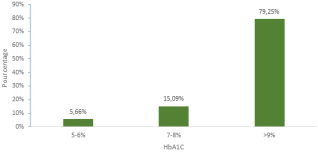
The mean age of the study population was 14.61 years, with a range from 10 to 18 years. The sample consisted of 64 females (60.38%) and 42 males (39.62%), resulting in a sex ratio of 0.66. Regarding socioeconomic status, most families had a middle socioeconomic level (58.95%), while 14.74% and 4.21%belonged to the low and very low socioeconomic categories, respectively. The mean glycated hemoglobin (HbA1c) level was 11.17%. Only 5.66% of patients achieved good glycemic control (HbA1c < 7%), indicating that the vast majority of adolescents had suboptimal metabolic control. With respect to insulin therapy, 66 adolescents were treated with human insulin, while 40 were receiving insulin analogues. A total of 61.22% of participants reported not administering insulin daily. The main reasons for missed insulin doses were simple forgetfulness (31.13%), intentional omission to test the necessity of treatment (25.47%), and expression of opposition toward parental authority (16.98%). According to the MMAS-8 score, 18.87% of patients exhibited low adherence to insulin therapy, while 27.36%demonstrated high adherence. Overall, 38.68% of adolescents were classified as adherent, whereas 61.32% were considered non-adherent. Adherence status was determined based on the combined criteria of Morisky score results, number of missed consultations, and insulin dose omissions.
Criteria for Poor Therapeutic Adherence: Poor therapeutic adherence was identified based on the following criteria:
1) Low adherence according to the Morisky score: 18.87%
2) More than one missed follow-up consultation: 6.60%
3) Skipping insulin doses: 61.22%
Several factors were found to be significantly associated with therapeutic adherence among adolescents with T1DM. Parental involvement played a key role in adherence. Adolescents whose parents provided only reminders had a significantly higher rate of poor adherence (67.19%) compared with those who benefited from full parental supervision (38.89%) (p = 0.003; 95% CI: [1.09–9.49]). Perceived loss of freedom related to treatment was also associated with poor adherence. Adolescents who felt that insulin therapy restricted their freedom exhibited poor adherence in 69.84% of cases, compared with 48.84% among those who did not share this perception (p = 0.029; 95% CI: [1.08–5.42]). The perception of treatment-related side effects was significantly associated with non-adherence. Poor adherence was observed in 74.55% of adolescents reporting side effects, compared with 47.06% among those who did not perceive side effects. Adolescents whose diabetes diagnosis was disclosed by a general practitioner had a 4.97-fold increased risk of poor adherence compared with those whose diagnosis was announced by a pediatrician (p = 0.03; 95% CI: [1.10–5.72]). Finally, a significant correlation was found between poor therapeutic adherence and poor glycemic control. Adolescents with an HbA1c level greater than 9% had a tenfold higher risk of non-adherence compared with those with an HbA1c level below 7% (p = 0.03; 95% CI: [1.11–89.75]).
Figure 1. Distribution of patients according to glycated hemoglobin levels.
4. Discussion
In the present study, 38.68% of adolescents demonstrated good therapeutic adherence, while 61.32% exhibited poor adherence. Weissberg-Benchell et al. reported a lower rate of poor adherence (25%) among adolescents with type 1 diabetes
| [11] | Weissberg-Benchell J, Glasgow AM, Tynan WD, et al. Adolescent diabetes management and nonmanagement. Diabetes Care. 1995; 18(1): 77-82. |
[11]
. However, the literature indicates that non-adherence rates in adolescents with chronic diseases are often comparable to those observed in adults, ranging from 30% to 50%
| [8] | Baron S, Caquard M, Caldagues E, et al. Therapeutic adherence in childhood and adolescent diabetes. Arch Pediatr. 2017; 24(2): 94-102. |
| [12] | Alvin P. Adolescents and treatment compliance. Enfances & Psy. 2004; 25(1): 46-54. |
[8, 12]
. The relatively high prevalence of poor adherence observed in our study may be explained by the exclusive inclusion of adolescents, a population known to be particularly vulnerable to treatment discontinuation. Regarding socioeconomic status, 18.95% of families belonged to low or very low socioeconomic categories, 58.95% to the middle category, and 22.1% to high or very high categories. Although our study population appeared to have a higher socioeconomic level compared with previous studies conducted in Dakar, such as that of Niang et al.
| [13] | Niang B, Faye P M, Ly I D, et al. Epidemiological and clinical profile of type 1 diabetes in children in Dakar. CAMES Santé. 2015; 3(2): 89-93. |
[13]
, no significant association was found between socioeconomic status and therapeutic adherence. This finding suggests that non-adherence in adolescents may be influenced more strongly by psychosocial and behavioral factors than by economic constraints alone.
Parental involvement emerged as a key determinant of adherence in our study. Adolescents under full parental supervision demonstrated significantly better adherence than those whose parents provided only reminders. Similar findings were reported by Pamela S. King et al. in the United States, who showed that declines in both maternal and paternal involvement over time were associated with reduced adherence in adolescents with T1DM
| [14] | King PS, Berg CA, Butner J, et al. Longitudinal trajectories of parental involvement in type 1 diabetes and adolescent adherence. Health Psychol. 2014; 33(5): 424-432. |
[14]
. Deborah J. Wiebe et al. also reported an inverse relationship between perceived low maternal involvement and adherence, while noting that overly intrusive or controlling parental behaviors could have negative effects, particularly in older adolescents
| [15] | Wiebe DJ, Helgeson VS, Berg CA, et al. Maternal involvement and adherence to diabetes treatment in adolescents. J Pediatr Psychol. 2005; 30(2): 167-176. |
[15]
.
Adolescence is characterized by a strong desire for autonomy and independence, which may conflict with parental monitoring and the constraints imposed by chronic disease management. Furthermore, adolescents tend to focus on the present, making it difficult for them to fully comprehend long-term complications and life-threatening risks associated with poor glycemic control
| [8] | Baron S, Caquard M, Caldagues E, et al. Therapeutic adherence in childhood and adolescent diabetes. Arch Pediatr. 2017; 24(2): 94-102. |
| [16] | Farthing P, Bally J, Rennie DC, et al. Sharing responsibilities for type 1 diabetes management between adolescents and parents: an integrative review. J Spec Pediatr Nurs. 2022; 27: e12395. https://doi.org/10.1111/jspn.12395 |
[8, 16]
. This complex dynamic may negatively affect parent–adolescent relationships and diabetes self-management.
In our study, 78.30% of adolescents perceived insulin treatment as a restriction of their freedom, and this perception was significantly associated with poor adherence. Although few studies have specifically explored this aspect, existing literature highlights that the daily constraints imposed by diabetes management—such as insulin injections, dietary rules, and regular monitoring—may conflict with adolescents’ desire for independence and negatively influence adherence
| [8] | Baron S, Caquard M, Caldagues E, et al. Therapeutic adherence in childhood and adolescent diabetes. Arch Pediatr. 2017; 24(2): 94-102. |
| [17] | Taddeo D, Egedy M, Frappier JY. Treatment adherence in adolescents. Paediatr Child Health. 2008; 13(1): 19-24. |
| [18] | Jacquin P, Levine M. Adherence difficulties in chronic diseases during adolescence: understanding to improve care. Arch Pediatr. 2008; 15(1): 89-94. |
[8, 17, 18]
. These findings underscore the importance of patient-centered therapeutic education that promotes dialogue and actively considers adolescents’ psychosocial needs.
We also identified a significant association between perceived treatment-related side effects and poor adherence, regardless of the type of insulin used. Adolescents reporting side effects—mainly pain and cramps—were significantly more likely to be non-adherent. These findings are consistent with those reported by Al-Ramahi et al.
| [19] | Al-Ramahi R. Medication adherence and associated factors among hypertensive patients in Palestine. J Epidemiol Glob Health. 2014; 5(2): 125-131. |
[19]
and with broader evidence indicating that perceived side effects constitute a major barrier to adherence in chronic diseases
| [20] | Morris AD, Boyle DI, McMahon AD, et al. Adherence to insulin therapy and glycaemic control in insulin-dependent diabetes mellitus. Lancet. 1997; 350(9090): 1505-1510. |
| [21] | Odegard PS, Capoccia K. Medication taking and diabetes. Diabetes Educ. 2007; 33(6): 1014-1029. |
[20, 21]
. Such adverse experiences may discourage patients from following treatment recommendations and compromise disease control.
Another notable finding was the association between the professional responsible for diagnostic disclosure and therapeutic adherence. Adolescents whose diabetes diagnosis was disclosed by a general practitioner had a nearly fivefold increased risk of poor adherence compared with those whose diagnosis was announced by a pediatric specialist. Although comparable studies are scarce, this result highlights the critical role of diagnostic disclosure in shaping patients’ understanding, acceptance, and long-term engagement in care
| [18] | Jacquin P, Levine M. Adherence difficulties in chronic diseases during adolescence: understanding to improve care. Arch Pediatr. 2008; 15(1): 89-94. |
| [22] | Haute Autorité de Santé. Disclosure and support following the diagnosis of chronic disease: care pathway guidelines. Saint-Denis La Plaine, France: HAS; 2014. |
[18, 22]
. Pediatric specialists may be better equipped to provide age-appropriate explanations, establish trust, and address the psychosocial dimensions of chronic illness, thereby fostering better adherence.
Finally, we observed a significant correlation between poor therapeutic adherence and poor glycemic control. The mean HbA1c level in our study population was 11.17%, with approximately four-fifths of adolescents exhibiting HbA1c values above 9%. Similar findings have been reported in other African settings, such as Niger and Tunisia
| [23] | Mahamane Aminou MS, Ousmane Bounou O, Daou M, et al. Clinical profile of childhood and adolescent diabetes in Niger. Health Sci Dis. 2022; 23(3). |
| [24] | Ben Ahmed I, Zouari B, Amri R, et al. Clinical and evolutionary profile of Tunisian adolescents with type 1 diabetes. Ann Endocrinol (Paris). 2016; 77(4): 472-473. |
[23, 24]
, whereas lower mean HbA1c levels have been observed in European cohorts
| [25] | Pelicand J, Maes M, Charlier D, et al. Adolescence and type 1 diabetes: self-care and glycemic control. Arch Pediatr. 2012; 19(6): 585-592. |
[25]
. These disparities may reflect differences in socioeconomic conditions, health system resources, and access to diabetes education and monitoring tools.
The strong association between non-adherence and elevated HbA1c levels reinforces the critical role of adherence in achieving optimal metabolic control. Similar associations have been documented in type 2 diabetes
| [26] | Currie CJ, Peyrot M, Morgan CL, et al. The impact of treatment non-adherence on mortality in type 2 diabetes. Diabetes Care. 2012; 35(6): 1279-1284. |
[26]
, emphasizing the need to identify and support adolescents at high risk of non-adherence to improve long-term outcomes.
5. Conclusion
The prevalence of type 1 diabetes among children and adolescents is steadily increasing. Therapeutic adherence, a cornerstone of complication prevention, is influenced by multiple factors that are particularly pronounced during adolescence. Our study demonstrates that adherence in adolescents with T1D is strongly affected by psychosocial and contextual determinants, including parental involvement, perceived loss of freedom, treatment-related side effects, and the professional responsible for diagnostic disclosure. Notably, the role of the healthcare professional delivering the diagnosis appears to be a critical factor influencing long-term adherence. These findings highlight the importance of tailored training for healthcare providers involved in diagnostic disclosure and adolescent diabetes management. Integrating these considerations into clinical practice may improve therapeutic adherence and contribute to better glycemic control and prevention of complications in adolescents living with type 1 diabetes.
Abbreviations
T1DM | Type 1 Diabetes Mellitus |
IDF | International Diabetes Federation |
MMAS | Morisky Medication Adherence Scale |
HbA1c | Glycated Hemoglobin |
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
World Health Organization. Global report on diabetes [Internet]. Geneva: World Health Organization; 2016 [cited 2023 May 18]. 86 p. Available from:
https://apps.who.int/iris/handle/10665/254648
|
| [2] |
National College of University Pediatricians; National College of Hospital and University Pediatric Surgery. Pediatrics. 8th ed. Issy-les-Moulineaux, France: Elsevier Masson; 2021.
|
| [3] |
Ward ZJ, Yeh JM, Reddy CL, et al. Global estimates of incidence of type 1 diabetes in children and adolescents aged 0-19 years: a simulation-based analysis. Lancet Diabetes Endocrinol. 2022; 10(12): 848-858.
|
| [4] |
International Diabetes Federation. IDF Diabetes Atlas. 11th ed. Brussels, Belgium: International Diabetes Federation; 2025.
|
| [5] |
Magliano DJ, Boyko EJ. IDF Diabetes Atlas. 10th ed. Brussels, Belgium: International Diabetes Federation; 2021.
|
| [6] |
Brink SJ; International Society for Pediatric and Adolescent Diabetes. Diabetes in Childhood and Adolescence. 2nd ed. Bagsværd, Denmark: Novo Nordisk; 2013.
|
| [7] |
Desbrus-Qochih A, Cathébras P. Adherence or compliance? Rethinking therapeutic adherence. Medecine & Longévité. 2012; 4(3-4): 111-122.
|
| [8] |
Baron S, Caquard M, Caldagues E, et al. Therapeutic adherence in childhood and adolescent diabetes. Arch Pediatr. 2017; 24(2): 94-102.
|
| [9] |
Korb-Savoldelli V, Gillaizeau F, Pouchot J, et al. Validation of a French version of the 8-item Morisky Medication Adherence Scale in hypertensive patients. J Clin Hypertens. 2012; 14(7): 429-434.
|
| [10] |
Plakas S, Mastrogiannis D, Mantzorou M, et al. Validation of the Morisky Medication Adherence Scale (MMAS-8) in chronic ambulatory patients. Open J Nurs. 2016; 6(3): 158-169.
|
| [11] |
Weissberg-Benchell J, Glasgow AM, Tynan WD, et al. Adolescent diabetes management and nonmanagement. Diabetes Care. 1995; 18(1): 77-82.
|
| [12] |
Alvin P. Adolescents and treatment compliance. Enfances & Psy. 2004; 25(1): 46-54.
|
| [13] |
Niang B, Faye P M, Ly I D, et al. Epidemiological and clinical profile of type 1 diabetes in children in Dakar. CAMES Santé. 2015; 3(2): 89-93.
|
| [14] |
King PS, Berg CA, Butner J, et al. Longitudinal trajectories of parental involvement in type 1 diabetes and adolescent adherence. Health Psychol. 2014; 33(5): 424-432.
|
| [15] |
Wiebe DJ, Helgeson VS, Berg CA, et al. Maternal involvement and adherence to diabetes treatment in adolescents. J Pediatr Psychol. 2005; 30(2): 167-176.
|
| [16] |
Farthing P, Bally J, Rennie DC, et al. Sharing responsibilities for type 1 diabetes management between adolescents and parents: an integrative review. J Spec Pediatr Nurs. 2022; 27: e12395.
https://doi.org/10.1111/jspn.12395
|
| [17] |
Taddeo D, Egedy M, Frappier JY. Treatment adherence in adolescents. Paediatr Child Health. 2008; 13(1): 19-24.
|
| [18] |
Jacquin P, Levine M. Adherence difficulties in chronic diseases during adolescence: understanding to improve care. Arch Pediatr. 2008; 15(1): 89-94.
|
| [19] |
Al-Ramahi R. Medication adherence and associated factors among hypertensive patients in Palestine. J Epidemiol Glob Health. 2014; 5(2): 125-131.
|
| [20] |
Morris AD, Boyle DI, McMahon AD, et al. Adherence to insulin therapy and glycaemic control in insulin-dependent diabetes mellitus. Lancet. 1997; 350(9090): 1505-1510.
|
| [21] |
Odegard PS, Capoccia K. Medication taking and diabetes. Diabetes Educ. 2007; 33(6): 1014-1029.
|
| [22] |
Haute Autorité de Santé. Disclosure and support following the diagnosis of chronic disease: care pathway guidelines. Saint-Denis La Plaine, France: HAS; 2014.
|
| [23] |
Mahamane Aminou MS, Ousmane Bounou O, Daou M, et al. Clinical profile of childhood and adolescent diabetes in Niger. Health Sci Dis. 2022; 23(3).
|
| [24] |
Ben Ahmed I, Zouari B, Amri R, et al. Clinical and evolutionary profile of Tunisian adolescents with type 1 diabetes. Ann Endocrinol (Paris). 2016; 77(4): 472-473.
|
| [25] |
Pelicand J, Maes M, Charlier D, et al. Adolescence and type 1 diabetes: self-care and glycemic control. Arch Pediatr. 2012; 19(6): 585-592.
|
| [26] |
Currie CJ, Peyrot M, Morgan CL, et al. The impact of treatment non-adherence on mortality in type 2 diabetes. Diabetes Care. 2012; 35(6): 1279-1284.
|
Cite This Article
-
APA Style
Mbaye, A., Sow, N. F., Jeribi, H., Diagne, G., Kane, A., et al. (2026). Assessment of Therapeutic Adherence Among Adolescents with Type 1 Diabetes at the University Hospital Center of Dakar. American Journal of Pediatrics, 12(1), 9-13. https://doi.org/10.11648/j.ajp.20261201.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Mbaye, A.; Sow, N. F.; Jeribi, H.; Diagne, G.; Kane, A., et al. Assessment of Therapeutic Adherence Among Adolescents with Type 1 Diabetes at the University Hospital Center of Dakar. Am. J. Pediatr. 2026, 12(1), 9-13. doi: 10.11648/j.ajp.20261201.12
Copy
|
Download
AMA Style
Mbaye A, Sow NF, Jeribi H, Diagne G, Kane A, et al. Assessment of Therapeutic Adherence Among Adolescents with Type 1 Diabetes at the University Hospital Center of Dakar. Am J Pediatr. 2026;12(1):9-13. doi: 10.11648/j.ajp.20261201.12
Copy
|
Download
-
@article{10.11648/j.ajp.20261201.12,
author = {Aminata Mbaye and Ndeye Fatou Sow and Hiba Jeribi and Guillaye Diagne and Awa Kane and Mame Awa Ndao and Ibrahima Diop and Maryam Aida Kane and Amadou Sow and Djibril Boiro and Babacar Niang},
title = {Assessment of Therapeutic Adherence Among Adolescents with Type 1 Diabetes at the University Hospital Center of Dakar},
journal = {American Journal of Pediatrics},
volume = {12},
number = {1},
pages = {9-13},
doi = {10.11648/j.ajp.20261201.12},
url = {https://doi.org/10.11648/j.ajp.20261201.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261201.12},
abstract = {Introduction: Type 1 diabetes mellitus (T1DM) is a chronic disease that predominantly affects children and adolescents. Its management requires strict adherence to medical recommendations in order to prevent severe acute and chronic complications. However, during adolescence, therapeutic adherence often becomes challenging due to physical, psychological, and social factors specific to this stage of life. The objective of this study was to determine the prevalence of poor therapeutic adherence among adolescents with T1DM followed in pediatric departments of the University Hospital Center of Dakar and to identify the factors associated with non-adherence. Methods: This was a prospective, descriptive, analytical, and multicenter study conducted over a three-month period (March–April–May 2023) in the pediatric departments of Abass Ndao Hospital Center and Albert Royer National Children’s Hospital in Dakar, Senegal. All patients aged 10 to 18 years with a diagnosis of T1DM for at least three months who attended outpatient consultations during the study period were included. Data were collected at the end of consultations using a pre-established questionnaire. Written informed consent was obtained from all participants and their caregivers. Therapeutic adherence to insulin was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8). Results: A total of 106 adolescents were included among 219 children who attended consultations during the study period. The sex ratio was 0.66, and the mean age was 14.61 years. According to the Morisky score, low adherence to insulin therapy was observed in 18.87% of patients, while good adherence was found in 27.36%. Overall, the prevalence of poor therapeutic adherence was 61.32%. Several factors were significantly associated with adherence. Full parental supervision was associated with better adherence compared to minimal parental involvement (p = 0.003). A perceived loss of freedom related to treatment and the presence of treatment-related side effects were significantly associated with poor adherence (p = 0.029 and p = 0.003, respectively). Poor adherence was also associated with diabetes diagnosis disclosure by a general practitioner rather than a pediatrician (p = 0.03). Furthermore, poor therapeutic adherence was significantly correlated with poor glycemic control (p = 0.03). Conclusion: This study highlights the importance of considering adolescent-specific factors in the management of type 1 diabetes. Improved understanding of these determinants may contribute to more effective care strategies and better prevention of complications among adolescents living with T1DM.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessment of Therapeutic Adherence Among Adolescents with Type 1 Diabetes at the University Hospital Center of Dakar
AU - Aminata Mbaye
AU - Ndeye Fatou Sow
AU - Hiba Jeribi
AU - Guillaye Diagne
AU - Awa Kane
AU - Mame Awa Ndao
AU - Ibrahima Diop
AU - Maryam Aida Kane
AU - Amadou Sow
AU - Djibril Boiro
AU - Babacar Niang
Y1 - 2026/01/23
PY - 2026
N1 - https://doi.org/10.11648/j.ajp.20261201.12
DO - 10.11648/j.ajp.20261201.12
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 9
EP - 13
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20261201.12
AB - Introduction: Type 1 diabetes mellitus (T1DM) is a chronic disease that predominantly affects children and adolescents. Its management requires strict adherence to medical recommendations in order to prevent severe acute and chronic complications. However, during adolescence, therapeutic adherence often becomes challenging due to physical, psychological, and social factors specific to this stage of life. The objective of this study was to determine the prevalence of poor therapeutic adherence among adolescents with T1DM followed in pediatric departments of the University Hospital Center of Dakar and to identify the factors associated with non-adherence. Methods: This was a prospective, descriptive, analytical, and multicenter study conducted over a three-month period (March–April–May 2023) in the pediatric departments of Abass Ndao Hospital Center and Albert Royer National Children’s Hospital in Dakar, Senegal. All patients aged 10 to 18 years with a diagnosis of T1DM for at least three months who attended outpatient consultations during the study period were included. Data were collected at the end of consultations using a pre-established questionnaire. Written informed consent was obtained from all participants and their caregivers. Therapeutic adherence to insulin was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8). Results: A total of 106 adolescents were included among 219 children who attended consultations during the study period. The sex ratio was 0.66, and the mean age was 14.61 years. According to the Morisky score, low adherence to insulin therapy was observed in 18.87% of patients, while good adherence was found in 27.36%. Overall, the prevalence of poor therapeutic adherence was 61.32%. Several factors were significantly associated with adherence. Full parental supervision was associated with better adherence compared to minimal parental involvement (p = 0.003). A perceived loss of freedom related to treatment and the presence of treatment-related side effects were significantly associated with poor adherence (p = 0.029 and p = 0.003, respectively). Poor adherence was also associated with diabetes diagnosis disclosure by a general practitioner rather than a pediatrician (p = 0.03). Furthermore, poor therapeutic adherence was significantly correlated with poor glycemic control (p = 0.03). Conclusion: This study highlights the importance of considering adolescent-specific factors in the management of type 1 diabetes. Improved understanding of these determinants may contribute to more effective care strategies and better prevention of complications among adolescents living with T1DM.
VL - 12
IS - 1
ER -
Copy
|
Download