Abstract
Introduction: Atrial fibrillation (AF) is a frequent complication of rheumatic mitral valve disease and is based on a complex substrate of atrial remodeling. The pulmonary veins represent a key site for AF initiation; however, the cellular and histological determinants involved remain incompletely understood. By analogy with their pacemaker role in the gastrointestinal tract, interstitial cells of Cajal (ICCs) have been proposed as potential modulators of atrial electrical activity. Objectives: To investigate the histological and immunohistochemical characteristics of the left atrium–pulmonary vein junction, with particular emphasis on the presence of interstitial cells of Cajal (ICCs), in patients undergoing surgery for rheumatic mitral valve disease, and to analyze their association with atrial fibrillation. Methods: This was a prospective study conducted from August 2023 to July 2024 including 11 patients undergoing surgery for rheumatic mitral valve disease at Fann Teaching Hospital (Dakar). Tissue samples were obtained from the junction between the left atrium and the right superior pulmonary vein. Analyses included standard histological examination and immunohistochemical studies using CD34 and DOG1 markers. Clinical, electrocardiographic, and echocardiographic data were correlated with the anatomopathological findings. Results: The study population was predominantly young and female, with a high prevalence of advanced rheumatic heart disease. Four patients presented with atrial fibrillation, predominantly permanent. Histological analysis revealed diffuse interstitial fibrosis and marked architectural disorganization in nearly all specimens, regardless of cardiac rhythm. Interstitial cells of Cajal were identified at low density but more frequently in patients with atrial fibrillation, mainly within fibrotic areas and in close proximity to the atrial myocardial sleeve. CD34 staining was widely positive in all samples, indicating nonspecific fibro-interstitial remodeling, whereas DOG1 expression was negative in all patients. Conclusion: in this limited series, interstitial cells of Cajal were present at low density at the left atrium–pulmonary vein junction and appeared to be preferentially associated with atrial fibrillation in the context of chronic atrial remodeling. These cells seem to be integrated into a remodeled fibro-interstitial microenvironment without constituting a specific histological marker of atrial fibrillation. These findings support the hypothesis of a mainly modulatory role of Cajal-like interstitial cells in valvular atrial arrhythmogenesis and justify further studies combining morphological and functional analyses.
|
Published in
|
Cardiology and Cardiovascular Research (Volume 10, Issue 2)
|
|
DOI
|
10.11648/j.ccr.20261002.11
|
|
Page(s)
|
11-19 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Atrial Fibrillation, Rheumatic Mitral Valve Disease, Africa, Pulmonary Veins, Left Atrium, Interstitial Cells of Cajal
1. Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and represents a major global public health concern. Despite considerable progress in understanding its pathophysiological mechanisms, the cellular and tissue substrates involved in the initiation and maintenance of this arrhythmia remain incompletely understood. Pulmonary veins (PVs) are now recognized as the principal source of ectopic foci capable of triggering AF, as demonstrated by seminal studies. However, the precise nature of the substrate responsible for this abnormal electrical activity remains a subject of ongoing debate and continues to be the focus of extensive research
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
| [2] | Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circulation Research. 2017; 120(9): 1501-1517.
https://doi.org/10.1161/CIRCRESAHA.117.309732 |
[1, 2]
. In this context, growing interest has focused on interstitial cells of Cajal (ICCs), which were initially described in the gastrointestinal tract. These cells play a crucial physiological pacemaker role by generating and propagating slow waves responsible for digestive peristaltic activity. They form a specialized three-dimensional network that coordinates communication between smooth muscle cells and enteric neural plexuses, thereby regulating intestinal motility
. Alterations in their density or function have been associated with several gastrointestinal motility disorders, including gastroparesis, Hirschsprung disease, and chronic intestinal pseudo-obstruction
. By analogy with their well-established role in the gastrointestinal tract, the presence of cells exhibiting similar morphological and immunohistochemical characteristics within myocardial tissue, particularly in the pulmonary veins and atria, has been suggested. The identification of cells expressing markers characteristic of interstitial cells of Cajal, notably c-Kit (CD117), in pulmonary myocardial tissue has led to the hypothesis that they may be involved in the generation of ectopic foci and in the propagation of abnormal electrical discharges responsible for atrial fibrillation
| [4] | Suciu L, Nicolescu MI, Popescu LM. Cardiac telocytes: serial dynamic images in cell culture. Journal of Cellular and Molecular Medicine. 2017; 21(11): 2688-2702.
https://doi.org/10.1111/jcmm.13176 |
[4]
. These cells, sometimes described as cardiac Cajal-like interstitial cells or telocytes, may contribute to the modulation of myocardial excitability and to electromechanical coupling within atrial tissue
| [5] | Varga I, Kyselovič J, Danišovič L, Gálfiová P, Kachlík D. Interstitial cells of Cajal-like cells (telocytes) in the heart and their potential role in cardiac regeneration and repair. Cells. 2019; 8(9): 1176. https://doi.org/10.3390/cells8091176 |
[5]
. From this perspective, the anatomopathological investigation of these interstitial cell populations within atrial tissue and at the pulmonary vein junction may provide valuable insights into their potential role in the development of an arrhythmogenic substrate. A better characterization of their distribution, density, and microenvironment could contribute to a deeper understanding of the structural mechanisms involved in atrial remodeling and AF pathophysiology. The present study therefore aimed to investigate the histological and immunohistochemical characteristics of the left atrium–pulmonary vein junction in patients undergoing surgery for mitral valve disease, with particular emphasis on the identification and distribution of Cajal-like interstitial cells. Morphological analyses were performed to evaluate their density, spatial distribution, and association with structural remodeling in patients with atrial fibrillation compared with those in sinus rhythm.
2. Patients and Methods
2.1. Patients
This was a prospective and analytical study conducted over a one-year period, from August 2023 to July 2024. All tissue samples were collected within the Department of Thoracic and Cardiovascular Surgery at Fann Teaching Hospital, within the Cuomo Cardiac Surgery Center. The study was conducted in accordance with the current ethical guidelines, following the acquisition of written informed consent from all included patients. The study population consisted of patients treated for rheumatic mitral valve disease requiring valve replacement surgery. A total of 45 patients who underwent surgery for acquired mitral valve diseases, including mitral regurgitation and/or mitral stenosis, with or without a history of atrial fibrillation (AF), were recorded during the study period. Among these, 11 patients underwent targeted anatomopathological analysis to search for the presence of interstitial cells of Cajal (ICCs) in the collected tissues. The clinical data included age, sex, medical history, and associated clinical signs. Paraclinical data consisted of electrocardiogram (ECG) analysis to document the presence or absence of AF, whether paroxysmal, persistent, permanent, or postoperative. Echocardiographic data included characterization of the mitral valve pathology, measurement of left atrial size, and assessment of right and left ventricular function. Anatomopathological results, particularly the presence or absence of interstitial cells of Cajal, were integrated with clinical and paraclinical data to analyze their potential association with atrial fibrillation in the context of rheumatic mitral valve disease.
2.2. Methods
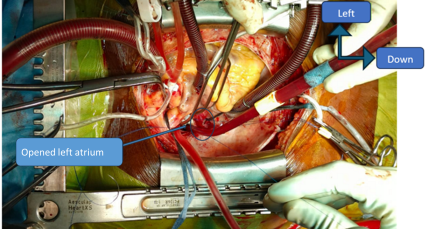
Each patient provided prior consent for the use and storage of collected tissue samples for research purposes through the signing of informed consent. A biobank was thus established using tissue samples collected from the junction between the left atrium (LA) and the right superior pulmonary vein (RSPV). The patients underwent surgery with cardiopulmonary bypass (CPB), which allowed for cardiac arrest and blood drainage. After median sternotomy and establishment of CPB, cardiac arrest was achieved by the administration of a cardioplegic solution, and access to the mitral valve was gained through the opening of the left atrium (
Figure 1). After precise identification of the sampling site at the LA–RSPV junction (
Figure 2), a tissue sample of approximately 1 cm², including a portion of the endocardium and underlying myocardium, was collected using a cold scalpel, and the site was closed with a 5/0 prolene suture. Each sample was then divided into two equal parts (
Figure 3) and prepared for subsequent analyses: fixation in formalin for histological study of interstitial cells of Cajal, or preservation in alcohol followed by freezing at −5°C for PITX2 gene analysis. The samples were prepared using different protocols depending on the analytical objectives, including fixation in AFA (alcohol, formalin, acetic acid) with paraffin embedding for histology and immunohistochemistry, 4% glutaraldehyde fixation with Epon resin embedding for electron microscopy studies, or conditioning in HBSS followed by cell culture for immunocytochemistry. Hematoxylin-phloxine-safran (HPS) staining was performed on paraffin sections to visualize muscle fibers and connective tissue, and both transverse and longitudinal sections were used to analyze the myocardial sleeve organization at the pulmonary veins and the LA–RSPV junction. Data entry and descriptive analysis were performed using Excel software.
Figure 1. Surgical access to the mitral valve (intraoperative view after median sternotomy and establishment of cardiopulmonary bypass, showing left atriotomy providing access to the mitral valve).
Figure 2. Tissue sampling site at the left atrium-pulmonary vein junction (intraoperative identification of the tissue sampling site at the junction between the left atrium and the right superior pulmonary vein, corresponding to the atrial myocardial sleeve region).
Figure 3. Processing of the tissue specimen.
Department of Thoracic and Cardiovascular Surgery, Fann Hospital, Dakar, Senegal.
Macroscopic view of the tissue sample divided into two equal parts: one fixed in formalin for histological and immunohistochemical analysis, and the other preserved for molecular studies.
3. Results
3.1. Epidemiological, Clinical, and Paraclinical Aspects
The eleven patients included consisted of 8 females and 3 males, yielding a male/female ratio of 0.4, with a mean age of 25 years (range: 14–54 years). The population was predominantly young, including 6 children and 5 adults, of whom 3 were over 40 years old. All patients were from West Africa, primarily Senegal (10/11), with one patient from The Gambia. The medical history revealed recurrent tonsillitis in 7 patients and polyarthralgia in 8, suggesting a rheumatic background, while two patients had experienced episodes of cardiac decompensation. Clinically, all patients presented symptoms compatible with mitral valve disease, including mitral regurgitation, mitral stenosis, or combined mitral disease. The mean cardiothoracic index was 0.64 (range: 0.4–0.8), reaching 0.71 in patients with atrial fibrillation, with cardiomegaly observed in 9 patients. On electrocardiogram, 7 patients were in sinus rhythm, while 4 had atrial fibrillation, including 3 permanent forms and 1 persistent form, which predominantly affected older patients, suggesting a mechanism related to chronic atrial remodeling. Echocardiography showed a mean left atrial diameter of 52 mm (range: 33–78 mm) and an average surface area of 41 cm² (range: 17–69 cm2), which increased to 62 mm and 43.5 cm2, respectively, in patients with atrial fibrillation, indicating more marked atrial dilation. The average left ventricular ejection fraction was 66% (range: 60–77%), indicating preserved systolic function and pointing to a predominantly atrial mechanism. Right ventricular function, assessed by TAPSE, averaged 19 mm (range: 12–28 mm), decreasing to 14 mm in patients with atrial fibrillation. Mitral valve diseases were mostly rheumatic (6 mitral regurgitations, 2 mitral stenoses, and 3 combined mitral diseases), associated with functional tricuspid regurgitation in 7 patients, with mean systolic pulmonary arterial pressures of 62 mmHg (range: 35–93 mmHg), reaching 71 mmHg in patients with atrial fibrillation; only one patient had a mitral valve disease of endocarditic origin. Biologically, no inflammatory syndrome was detected, with negative CRP and procalcitonin levels in all patients, a positive ASLO titer in only one patient without clinical significance, and negative infectious serologies. Histological examination of the left atrium–pulmonary vein junction allowed analysis of myocardial tissue organization, distribution of connective tissue, and potential inflammatory or fibrotic remodeling. Immunohistochemistry, including CD34 and DOG1 markers, provided a more detailed characterization of the interstitial compartment and tissue microenvironment to explore structural modifications potentially associated with atrial fibrillation and their relationship to preoperative cardiac rhythm.
3.2. Histological Aspects
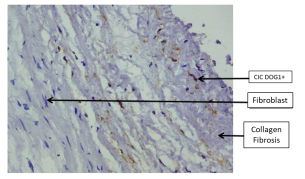
Histological examination of the left atrium–pulmonary vein junction revealed consistent fibrotic changes, most often of a fibrous (
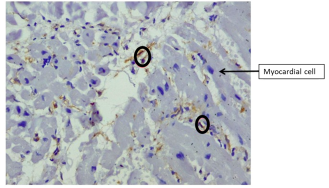
Figure 4) or muscle-fibrous (
Figure 5) nature. Rare fibrotic alterations were observed in a single patient with sinus rhythm. Both atrial fibrillation (AF) and sinus rhythm patients showed fibrosis, suggesting that it is a common structural substrate of atrial remodeling in mitral valve disease, without being rhythm-specific. A muscle component, identified in one patient (
Figures 6 and 7), reflected myocardial architectural heterogeneity at the LA–PV junction, which may favor local conduction abnormalities. Inflammatory signs were observed in several patients, irrespective of rhythm, with no direct correlation to AF, indicating a possible intercurrent or contributory process but not a distinguishing feature.
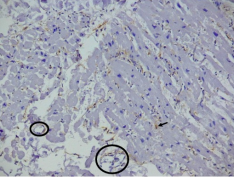
Figure 4. Fibrous tissue containing interstitial cells of Cajal highlighted by CD34 immunostaining (original magnification ×300).
Department of Pathology (Anatomical and Cytopathology), Cheikh Anta Diop University of Dakar, Senegal.
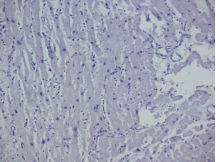
Figure 5. Myocardial tissue containing a few interstitial cells of Cajal highlighted by CD34 immunostaining (original magnification ×400).
Department of Pathology (Anatomical and Cytopathology), Cheikh Anta Diop University of Dakar, Senegal.
Figure 6. Myocardial tissue containing a few interstitial cells of Cajal highlighted by CD34 immunostaining (original magnification ×300).
Department of Pathology (Anatomical and Cytopathology), Cheikh Anta Diop University of Dakar, Senegal.
Figure 7. Higher magnification view highlighting myocardial fiber disorganization near the atrial myocardial sleeve (HPS staining, original magnification ×400).
Department of Pathology (Anatomical and Cytopathology), Cheikh Anta Diop University of Dakar, Senegal.
Immunohistochemistry for interstitial cells of Cajal (ICCs), using specific markers, was performed on all 11 patients. ICCs were present at low to moderate density, with variable distribution based on rhythm. They were more frequent in AF patients, particularly in fibrotic areas and near the atrial myocardial sleeve. In contrast, sinus rhythm patients had few or no detectable ICCs. Although the total number of ICCs remained low, their higher presence in AF patients suggests an association with atrial remodeling rather than a normal physiological state.
CD34 staining, a marker of endothelial cells, hematopoietic progenitors, and fibroblastic interstitial cells, was commonly positive, showing fibrous or muscle-fibrous patterns in both AF and sinus rhythm groups. This indicates diffuse fibro-interstitial remodeling, non-specific to the rhythm. ICCs were located in a CD34-positive microenvironment, suggesting they are integrated into a remodeled fibro-interstitial substrate. However, CD34’s nonspecific nature prevents it from distinguishing AF patients from those in sinus rhythm.
DOG1, a membrane protein involved in calcium-dependent ion channel activity, was negative across all patients. This lack of expression suggests that the observed ICCs do not represent a distinct or immunohistochemically dominant population based on this marker. Overall, these findings indicate that ICCs are present at low density but more frequently in AF patients, where they are closely associated with fibrotic and disorganized myocardial areas, potentially contributing to the remodeled, arrhythmogenic microenvironment. However, they do not serve as a specific or quantitatively discriminating marker of AF.
4. Discussion
4.1. Epidemiological, Clinical, and Paraclinical Aspects
The epidemiological, clinical, and paraclinical characteristics observed in this series align with the typical profile of rheumatic mitral valve disease complicated by atrial fibrillation (AF) in low- and middle-income countries, particularly in Sub-Saharan Africa. The strong female predominance (sex ratio M/F = 0.4) is consistent with the literature, which reports that women account for 60–75% of patients with chronic rheumatic heart disease
. This predominance is generally attributed to socio-economic, cultural, and healthcare-related factors, including delayed access to care, underdiagnosis of early-stage acute rheumatic fever, and prolonged progression of valve lesions in women, which favors atrial remodeling and the development of AF
| [8] | Zühlke L, Engel ME, Karthikeyan G, et al. Characteristics, complications, and gaps in evidence-based interventions in rheumatic heart disease: the Global Rheumatic Heart Disease Registry (REMEDY Study). European Heart Journal. 2020; 41(6): 823-830. https://doi.org/10.1093/eurheartj/ehz519 |
[8]
.
The particularly young average age of the study population, with a significant proportion of children and young adults, contrasts sharply with data from industrialized countries, where AF predominantly occurs after the age of 65 in a degenerative, hypertensive, or metabolic context
. This difference highlights the persistent burden of rheumatic heart disease in West Africa, which leads to early-onset "valvular" AF, as confirmed by Global Burden of Disease estimates, which show a disproportionate burden of rheumatic disease in low-income regions
| [11] | Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease. New England Journal of Medicine. 2017; 377: 713-722.
https://doi.org/10.1056/NEJMoa1603693 |
[11]
.
The frequent history of recurrent tonsillitis and polyarthralgia observed in this series is classically reported in cohorts of chronic rheumatic heart disease, even in the absence of recent biological documentation of acute rheumatic fever
| [12] | Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nature Reviews Disease Primers. 2016; 2: 15084. https://doi.org/10.1038/nrdp.2015.84 |
[12]
. These clinical features strengthen the hypothesis of longstanding rheumatic involvement evolving silently into severe valve lesions and late-onset rhythm complications.
Clinically and echocardiographically, the predominance of isolated mitral regurgitation or associated mitral stenosis is consistent with recent African data, where mitral regurgitation is the most frequent presentation of rheumatic heart disease
| [13] | Marijon E, Ou P, Celermajer DS, et al. Prevalence of rheumatic heart disease detected by echocardiographic screening. New England Journal of Medicine. 2021; 384: 1241-1250.
https://doi.org/10.1056/NEJMoa2028453 |
[13]
. Mixed forms, found in about one-third of patients, are particularly arrhythmogenic due to the chronic volume and pressure overload they impose on the left atrium, promoting structural and electrical remodeling conducive to AF
.
Radiological data confirm chronic hemodynamic impact, with an average cardiothoracic index of 0.64 (range: 0.4–0.8), and cardiomegaly observed in most patients. Similar results have been reported in several African series, where cardiomegaly is described in over 70% of patients with complicated rheumatic valve disease
. The more pronounced increase in cardiothoracic index in AF patients suggests a strong link between global cardiac dilation, chronic hemodynamic overload, and persistent arrhythmia
.
The high proportion of patients with AF in this series, mostly in its permanent form, aligns with contemporary data indicating that AF complicates 40–70% of hospitalized cases of rheumatic mitral valve disease in Africa
. The fact that AF predominantly affects older patients in the cohort strengthens the hypothesis of a mechanism related to the duration of valve disease and cumulative atrial remodeling, rather than a degenerative process linked to chronological aging
.
Echocardiography revealed significant left atrial dilation, particularly in AF patients, confirming the central role of this parameter as a major structural determinant of valvular AF
| [19] | Thomas L, Abhayaratna WP. Left atrial reverse remodeling: mechanisms and clinical significance. Journal of the American College of Cardiology. 2019; 73(7): 885-897.
https://doi.org/10.1016/j.jacc.2018.11.061 |
[19]
. Recent studies have shown that an increase in left atrial volume often precedes the onset of AF and serves as a reliable marker of advanced atrial remodeling
. The overall preservation of left ventricular ejection fraction observed in this series suggests an AF mechanism primarily atrial in origin, secondary to fibrosis, conduction heterogeneity, and alterations in the myocardial microenvironment, rather than primary left ventricular dysfunction
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
. The frequent association with functional tricuspid regurgitation and pulmonary hypertension, also described in recent series, contributes to bi-atrial remodeling and the chronicity of the arrhythmia
.
Finally, the low positivity of ASLO and the absence of biological inflammatory syndrome observed in this series are consistent with data showing that these markers lose their diagnostic value long after the acute phase of rheumatic fever, especially in adults
. The absence of elevated CRP and procalcitonin levels, along with negative infectious serologies, suggests that the AF observed is primarily related to a chronic remodeling process rather than persistent inflammatory activity, as emphasized by recent studies conducted in Africa and other regions with high rheumatic disease burden
.
4.2. Histological Results
Immunohistochemical analysis of the left atrium–pulmonary vein junction revealed the presence of Cajal-like interstitial cells (CICs) at low density, with a heterogeneous distribution according to cardiac rhythm. In this limited series, these cells appeared to be observed more frequently in patients with atrial fibrillation than in those with sinus rhythm. When present, CICs were predominantly located in regions considered critical from an arrhythmogenic standpoint, including areas of myocardial fibrosis, architectural disorganization, and the immediate vicinity of the atrial myocardial sleeve. These regions correspond to well-recognized sites involved in the initiation and maintenance of atrial fibrillation, as demonstrated by numerous anatomical, electrophysiological, and interventional studies focusing on the pulmonary veins and the left atrium
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
.
The preferential localization of CICs in these structurally remodeled areas suggests that they may contribute, directly or indirectly, to local modulation of myocardial excitability or to the propagation of ectopic electrical activity. However, given the limited sample size of the present study, these observations should be interpreted cautiously and considered descriptive rather than indicative of a definitive causal relationship. These observations suggest that Cajal-like interstitial cells (CICs) do not represent a major constitutive component of normal atrial tissue but may rather appear or persist in the context of pathological atrial remodeling. Their low presence in patients with sinus rhythm is consistent with previous studies showing that normal atrial tissue contains relatively few specialized interstitial cells, whereas their density tends to increase in conditions of hemodynamic overload, inflammation, or chronic fibrosis
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
.
CD34 immunostaining, which was widely positive in this series, highlights the presence of relatively consistent fibro-interstitial remodeling, regardless of cardiac rhythm. CD34 is classically expressed by various stromal cell populations, including endothelial cells, fibroblasts, and certain mesenchymal progenitor cells. In myocardial tissue, increased CD34 expression has been associated with processes of fibrosis, tissue repair, and chronic structural remodeling observed in several cardiac diseases
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
. The spatial association observed between Cajal-like interstitial cells (CICs) and areas strongly positive for CD34 suggests that these cells are embedded within a remodeled connective tissue microenvironment that may be favorable for their survival, differentiation, or participation in tissue remodeling processes. Such a modified stromal context may contribute to the formation of an arrhythmogenic substrate characterized by architectural disorganization of atrial tissue and alterations in electrical conduction properties. However, the relatively frequent CD34 positivity observed in both the atrial fibrillation and sinus rhythm groups confirms the nonspecific nature of this marker. Although it reflects the presence of stromal or vascular remodeling, its expression alone does not allow discrimination between pathological atrial tissue and tissue considered structurally normal, thereby limiting its value as a specific marker of atrial fibrillation
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
.
The absence of DOG1 expression in all patients represents a noteworthy finding. The homogeneous negativity of this marker in the present study suggests that the observed cardiac CICs do not correspond to a dominant DOG1-dependent phenotype but rather to a heterogeneous interstitial cell population, possibly closer to specialized fibroblast-like cells than to true autonomous pacemaker cells. This interpretation is consistent with previous reports describing the phenotypic diversity of cardiac interstitial cells, often grouped under the term telocytes or specialized interstitial cells, and characterized by the absence of a unique immunohistochemical signature
.
Taken together, these observations support the hypothesis that Cajal-like interstitial cells (CICs), when present in atrial tissue, are embedded within a deeply remodeled structural substrate. In this context, their potential role may be less that of primary generators of pacemaker activity and more that of local modulators of the electro-structural microenvironment. Through interactions with fibroblasts, myocardial fibers, and the extracellular matrix, these cells may contribute to conduction anisotropy and functional heterogeneity within atrial tissue, two central mechanisms in the pathophysiology of atrial fibrillation
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
.
This interpretation is consistent with experimental and clinical models showing that atrial fibrosis, myocardial architectural disorganization, and conduction abnormalities play a major role in the maintenance of persistent atrial fibrillation, often more so than the presence of isolated cellular pacemaker foci
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
.
However, several limitations should be considered. The relatively small sample size, the limited density of CICs observed, and the essentially semi-quantitative nature of the analysis restrict the scope of the conclusions. In addition, the absence of direct functional approaches (such as cellular electrophysiological analysis, ion channel studies, or high-resolution electrophysiological mapping) does not allow confirmation of an active electrophysiological role for these cells. Future studies integrating morphological, immunohistochemical, molecular, and functional approaches will be necessary to better define the precise role of CICs within the hierarchy of atrial arrhythmogenic mechanisms and to evaluate their potential contribution to the electro-structural remodeling characteristic of atrial fibrillation
| [1] | Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050 |
[1]
.
A methodological limitation of this study concerns the immunohistochemical identification of interstitial cells of Cajal. Classical ICCs are typically characterized by the expression of the tyrosine kinase receptor c-Kit (CD117), which is considered the reference marker for these cells. In the present study, immunohistochemical analysis relied on CD34 and DOG1 staining. Because DOG1 expression was negative in all cases and CD34 is not a specific marker for ICCs (being also expressed by endothelial cells, hematopoietic progenitors, fibroblastic stromal cells, and telocytes) the cells observed in this series cannot be definitively classified as classical ICCs. They should therefore be interpreted more cautiously as Cajal-like interstitial cells or CD34-positive interstitial cells within the atrial myocardial microenvironment. The absence of c-Kit immunostaining represents a limitation of the present study and reflects technical constraints related to antibody availability during the study period. Future studies combining CD34, c-Kit (CD117), and additional markers would allow a more precise characterization of these interstitial cell populations and help clarify their potential role in atrial arrhythmogenesis.
Because of the limited sample size, the observed differences should be interpreted as descriptive trends rather than statistically significant associations.
5. Conclusion
This study demonstrates that the left atrium–pulmonary vein junction is characterized by complex tissue remodeling dominated by diffuse interstitial fibrosis and marked architectural heterogeneity, constituting a structural substrate favorable to conduction abnormalities and atrial arrhythmogenesis in the setting of chronic rheumatic mitral valve disease. CD34 immunohistochemical staining highlights the consistent presence of fibro-interstitial remodeling regardless of cardiac rhythm, suggesting a common process related to prolonged hemodynamic overload rather than a specific marker of atrial fibrillation. In this limited series, Cajal-like interstitial cells appeared to be more frequently observed in patients with atrial fibrillation than in those with sinus rhythm. However, their overall density remained low, and they were predominantly located in areas of fibrosis and myocardial architectural disorganization near the atrial myocardial sleeve. This distribution suggests a potential indirect and contributory role within the arrhythmogenic microenvironment, without constituting a specific or quantitatively discriminative histological marker of atrial fibrillation in this limited cohort. These findings support the hypothesis that valvular atrial fibrillation primarily relies on a substrate of chronic structural remodeling, within which certain interstitial cell populations may locally modulate electrophysiological properties. Further studies involving larger cohorts and combined morphological, molecular, and functional approaches are warranted to clarify the exact role of these tissue alterations and to identify potential diagnostic or therapeutic targets in atrial fibrillation.
Abbreviations
AF | Atrial Fibrillation |
AFA | Alcohol–Formalin–Acetic Acid |
ASLO | Anti-Streptolysin O |
CD34 | Cluster of Differentiation 34 |
CIC | Cajal-like Interstitial Cells |
CPB | Cardiopulmonary Bypass |
CRP | C-Reactive Protein |
DOG1 | Discovered On Gastrointestinal Stromal Tumor-1 |
ECG | Electrocardiogram |
HBSS | Hanks’ Balanced Salt Solution |
HPS | Hematoxylin-Phloxine-Safran |
ICCs | Interstitial Cells of Cajal |
LA | Left Atrium |
LMIC | Low- and Middle-Income Countries |
LVEF | Left Ventricular Ejection Fraction |
PV | Pulmonary Vein |
RHD | Rheumatic Heart Disease |
RSPV | Right Superior Pulmonary Vein |
TAPSE | Tricuspid Annular Plane Systolic Excursion |
Author Contributions
Diagne Papa Amath: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – original draft
Ngom Khady: Formal Analysis, Methodology, Software
Diop Momar Sokhna: Data curation
Ba Papa Ousmane: Data curation
Diop Moussa Seck: Data curation
Mbaye Mareme Soda: Data curation
Faye Cheikh Abdou Khadre: Data curation
Dial Cherif Mouhamed: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing
Ba Papa Salmane: Data curation
Ciss Amadou Gabriel: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. Journal of the American College of Cardiology. 2020; 76(15): 1687-1700.
https://doi.org/10.1016/j.jacc.2020.07.050
|
| [2] |
Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circulation Research. 2017; 120(9): 1501-1517.
https://doi.org/10.1161/CIRCRESAHA.117.309732
|
| [3] |
Huizinga JD, Chen JH. Interstitial cells of Cajal: update on basic and clinical science. Current Gastroenterology Reports. 2014; 16(1): 363.
https://doi.org/10.1007/s11894-013-0363-9
|
| [4] |
Suciu L, Nicolescu MI, Popescu LM. Cardiac telocytes: serial dynamic images in cell culture. Journal of Cellular and Molecular Medicine. 2017; 21(11): 2688-2702.
https://doi.org/10.1111/jcmm.13176
|
| [5] |
Varga I, Kyselovič J, Danišovič L, Gálfiová P, Kachlík D. Interstitial cells of Cajal-like cells (telocytes) in the heart and their potential role in cardiac regeneration and repair. Cells. 2019; 8(9): 1176.
https://doi.org/10.3390/cells8091176
|
| [6] |
Mocumbi AO, Sliwa K. Women's cardiovascular health in sub-Saharan Africa. Heart. 2018; 104(23): 1960-1967.
https://doi.org/10.1136/heartjnl-2017-312371
|
| [7] |
Rothenbühler M, O'Sullivan CJ, Stortecky S, et al. Active surveillance for rheumatic heart disease in endemic regions. The Lancet Global Health. 2014; 2(12): e717-e726.
https://doi.org/10.1016/S2214-109X(14)70343-0
|
| [8] |
Zühlke L, Engel ME, Karthikeyan G, et al. Characteristics, complications, and gaps in evidence-based interventions in rheumatic heart disease: the Global Rheumatic Heart Disease Registry (REMEDY Study). European Heart Journal. 2020; 41(6): 823-830.
https://doi.org/10.1093/eurheartj/ehz519
|
| [9] |
Chugh SS, Roth GA, Gillum RF, Mensah GA. Global burden of atrial fibrillation in developed and developing nations. Global Heart. 2018; 13(4): 263-271.
https://doi.org/10.1016/j.gheart.2017.10.004
|
| [10] |
Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation. European Heart Journal. 2021; 42(5): 373-498.
https://doi.org/10.1093/eurheartj/ehaa612
|
| [11] |
Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease. New England Journal of Medicine. 2017; 377: 713-722.
https://doi.org/10.1056/NEJMoa1603693
|
| [12] |
Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nature Reviews Disease Primers. 2016; 2: 15084.
https://doi.org/10.1038/nrdp.2015.84
|
| [13] |
Marijon E, Ou P, Celermajer DS, et al. Prevalence of rheumatic heart disease detected by echocardiographic screening. New England Journal of Medicine. 2021; 384: 1241-1250.
https://doi.org/10.1056/NEJMoa2028453
|
| [14] |
Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases. The Lancet. 2020; 368(9540): 1005-1011.
https://doi.org/10.1016/S0140-6736(06)69208-8
|
| [15] |
Diao M, Kane A, Ndiaye MB, et al. Rheumatic heart disease in Senegal. Cardiovascular Journal of Africa. 2018; 29(2): 90-95.
https://doi.org/10.5830/CVJA-2017-051
|
| [16] |
Karthikeyan G, Mayosi BM. Is primary prevention of rheumatic fever the missing link in the control of rheumatic heart disease? Circulation. 2021; 124(12): 1324-1326.
https://doi.org/10.1161/CIRCULATIONAHA.111.050427
|
| [17] |
Sliwa K, Mocumbi AO. Forgotten cardiovascular diseases in Africa. Clinical Research in Cardiology. 2020; 109: 65-74.
https://doi.org/10.1007/s00392-019-01528-4
|
| [18] |
Zulkifly H, Lip GYH, Lane DA. Epidemiology of atrial fibrillation. International Journal of Clinical Practice. 2018; 72: e13070.
https://doi.org/10.1111/ijcp.13070
|
| [19] |
Thomas L, Abhayaratna WP. Left atrial reverse remodeling: mechanisms and clinical significance. Journal of the American College of Cardiology. 2019; 73(7): 885-897.
https://doi.org/10.1016/j.jacc.2018.11.061
|
| [20] |
Tops LF, Delgado V, Schalij MJ, Bax JJ. Left atrial remodeling in atrial fibrillation. Heart. 2020; 96: 113-119.
https://doi.org/10.1136/hrt.2009.175638
|
| [21] |
Gertz ZM, Raina A, Saghy L, et al. Evidence of atrial remodeling in pulmonary hypertension. Journal of the American College of Cardiology. 2022; 59: 1768-1775.
https://doi.org/10.1016/j.jacc.2012.01.038
|
| [22] |
Gewitz MH, Baltimore RS, Tani LY, et al. Revision of the Jones criteria for the diagnosis of acute rheumatic fever. Circulation. 2015; 131: 1806-1818.
https://doi.org/10.1161/CIR.0000000000000205
|
| [23] |
Beaton A, Okello E, Engelman D, et al. Rheumatic heart disease in Africa: the Mosi-o-Tunya call to action. The Lancet Global Health. 2021; 9: e105-e108.
https://doi.org/10.1016/S2214-109X(20)30425-4
|
| [24] |
Cretoiu D, Popescu LM. Telocytes revisited. Biomolecular Concepts. 2017; 8(1): 39-48.
https://doi.org/10.1515/bmc-2017-0005
|
Cite This Article
-
APA Style
Amath, D. P., Khady, N., Sokhna, D. M., Ousmane, B. P., Seck, D. M., et al. (2026). Tissue Substrate of Rheumatic Atrial Fibrillation: Atrial Fibrosis and Cajal-Like Interstitial Cells at the Left
Atrial–Pulmonary Vein Junction. Cardiology and Cardiovascular Research, 10(2), 11-19. https://doi.org/10.11648/j.ccr.20261002.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Amath, D. P.; Khady, N.; Sokhna, D. M.; Ousmane, B. P.; Seck, D. M., et al. Tissue Substrate of Rheumatic Atrial Fibrillation: Atrial Fibrosis and Cajal-Like Interstitial Cells at the Left
Atrial–Pulmonary Vein Junction. Cardiol. Cardiovasc. Res. 2026, 10(2), 11-19. doi: 10.11648/j.ccr.20261002.11
Copy
|
Download
AMA Style
Amath DP, Khady N, Sokhna DM, Ousmane BP, Seck DM, et al. Tissue Substrate of Rheumatic Atrial Fibrillation: Atrial Fibrosis and Cajal-Like Interstitial Cells at the Left
Atrial–Pulmonary Vein Junction. Cardiol Cardiovasc Res. 2026;10(2):11-19. doi: 10.11648/j.ccr.20261002.11
Copy
|
Download
-
@article{10.11648/j.ccr.20261002.11,
author = {Diagne Papa Amath and Ngom Khady and Diop Momar Sokhna and Ba Papa Ousmane and Diop Moussa Seck and Mbaye Mareme Soda and Faye Cheikh Abdou Khadre and Dial Cherif Mouhamed and Ba Papa Salmane and Ciss Amadou Gabriel},
title = {Tissue Substrate of Rheumatic Atrial Fibrillation: Atrial Fibrosis and Cajal-Like Interstitial Cells at the Left
Atrial–Pulmonary Vein Junction},
journal = {Cardiology and Cardiovascular Research},
volume = {10},
number = {2},
pages = {11-19},
doi = {10.11648/j.ccr.20261002.11},
url = {https://doi.org/10.11648/j.ccr.20261002.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20261002.11},
abstract = {Introduction: Atrial fibrillation (AF) is a frequent complication of rheumatic mitral valve disease and is based on a complex substrate of atrial remodeling. The pulmonary veins represent a key site for AF initiation; however, the cellular and histological determinants involved remain incompletely understood. By analogy with their pacemaker role in the gastrointestinal tract, interstitial cells of Cajal (ICCs) have been proposed as potential modulators of atrial electrical activity. Objectives: To investigate the histological and immunohistochemical characteristics of the left atrium–pulmonary vein junction, with particular emphasis on the presence of interstitial cells of Cajal (ICCs), in patients undergoing surgery for rheumatic mitral valve disease, and to analyze their association with atrial fibrillation. Methods: This was a prospective study conducted from August 2023 to July 2024 including 11 patients undergoing surgery for rheumatic mitral valve disease at Fann Teaching Hospital (Dakar). Tissue samples were obtained from the junction between the left atrium and the right superior pulmonary vein. Analyses included standard histological examination and immunohistochemical studies using CD34 and DOG1 markers. Clinical, electrocardiographic, and echocardiographic data were correlated with the anatomopathological findings. Results: The study population was predominantly young and female, with a high prevalence of advanced rheumatic heart disease. Four patients presented with atrial fibrillation, predominantly permanent. Histological analysis revealed diffuse interstitial fibrosis and marked architectural disorganization in nearly all specimens, regardless of cardiac rhythm. Interstitial cells of Cajal were identified at low density but more frequently in patients with atrial fibrillation, mainly within fibrotic areas and in close proximity to the atrial myocardial sleeve. CD34 staining was widely positive in all samples, indicating nonspecific fibro-interstitial remodeling, whereas DOG1 expression was negative in all patients. Conclusion: in this limited series, interstitial cells of Cajal were present at low density at the left atrium–pulmonary vein junction and appeared to be preferentially associated with atrial fibrillation in the context of chronic atrial remodeling. These cells seem to be integrated into a remodeled fibro-interstitial microenvironment without constituting a specific histological marker of atrial fibrillation. These findings support the hypothesis of a mainly modulatory role of Cajal-like interstitial cells in valvular atrial arrhythmogenesis and justify further studies combining morphological and functional analyses.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Tissue Substrate of Rheumatic Atrial Fibrillation: Atrial Fibrosis and Cajal-Like Interstitial Cells at the Left
Atrial–Pulmonary Vein Junction
AU - Diagne Papa Amath
AU - Ngom Khady
AU - Diop Momar Sokhna
AU - Ba Papa Ousmane
AU - Diop Moussa Seck
AU - Mbaye Mareme Soda
AU - Faye Cheikh Abdou Khadre
AU - Dial Cherif Mouhamed
AU - Ba Papa Salmane
AU - Ciss Amadou Gabriel
Y1 - 2026/04/10
PY - 2026
N1 - https://doi.org/10.11648/j.ccr.20261002.11
DO - 10.11648/j.ccr.20261002.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 11
EP - 19
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20261002.11
AB - Introduction: Atrial fibrillation (AF) is a frequent complication of rheumatic mitral valve disease and is based on a complex substrate of atrial remodeling. The pulmonary veins represent a key site for AF initiation; however, the cellular and histological determinants involved remain incompletely understood. By analogy with their pacemaker role in the gastrointestinal tract, interstitial cells of Cajal (ICCs) have been proposed as potential modulators of atrial electrical activity. Objectives: To investigate the histological and immunohistochemical characteristics of the left atrium–pulmonary vein junction, with particular emphasis on the presence of interstitial cells of Cajal (ICCs), in patients undergoing surgery for rheumatic mitral valve disease, and to analyze their association with atrial fibrillation. Methods: This was a prospective study conducted from August 2023 to July 2024 including 11 patients undergoing surgery for rheumatic mitral valve disease at Fann Teaching Hospital (Dakar). Tissue samples were obtained from the junction between the left atrium and the right superior pulmonary vein. Analyses included standard histological examination and immunohistochemical studies using CD34 and DOG1 markers. Clinical, electrocardiographic, and echocardiographic data were correlated with the anatomopathological findings. Results: The study population was predominantly young and female, with a high prevalence of advanced rheumatic heart disease. Four patients presented with atrial fibrillation, predominantly permanent. Histological analysis revealed diffuse interstitial fibrosis and marked architectural disorganization in nearly all specimens, regardless of cardiac rhythm. Interstitial cells of Cajal were identified at low density but more frequently in patients with atrial fibrillation, mainly within fibrotic areas and in close proximity to the atrial myocardial sleeve. CD34 staining was widely positive in all samples, indicating nonspecific fibro-interstitial remodeling, whereas DOG1 expression was negative in all patients. Conclusion: in this limited series, interstitial cells of Cajal were present at low density at the left atrium–pulmonary vein junction and appeared to be preferentially associated with atrial fibrillation in the context of chronic atrial remodeling. These cells seem to be integrated into a remodeled fibro-interstitial microenvironment without constituting a specific histological marker of atrial fibrillation. These findings support the hypothesis of a mainly modulatory role of Cajal-like interstitial cells in valvular atrial arrhythmogenesis and justify further studies combining morphological and functional analyses.
VL - 10
IS - 2
ER -
Copy
|
Download